2209
Reshaping of the lenticulostriate artery in middle cerebral artery occlusion1Radiology, Chinese PLA General Hospital, Beijing, China, 2Chinese PLA General Hospital, Beijing, China, 3State Key Laboratory of Brain and Cognitive Science, Institute of Biophysics, Chinese Academy of Sciences, Beijing, China, 4Research Collaboration Team, Siemens Healthineers, Beijing, China
Synopsis
Keywords: Blood Vessels, Blood vessels, 7T MRI,MR angiography, middle cerebral artery occlusion
Motivation: Territory supplied by lenticulostriate arteries includes deep subcortical grey matter nucleus which pose vast influence on neurological function.
Goal(s): To elaborate the modification of lenticulostriate arteries when middle cerebral artery occluded.
Approach: Patients with MCA occlusion were performed 7T time-of-flight MR angiography with voxel size of isotropic 0.3mm.
Results: Origination of LAS were modified to originated from the proximal end of occluded segment in 64.3%. While their morphometrical features were identical with the normal contralateral side LSA.
Impact: The finding may be helpful for the protection of LSA in endovascular procedure, and provide critical knowledge about the angiogenesis of middle cerebral artery. Future large sample size 7T MRI study is warranted.
INTRODUCTION:
The lenticulostriate arteries (LSA) are small arteries that arise from the middle cerebral artery and supply blood to the basal ganglia and internal capsule of the brain. Knowledges about anatomy and function of lenticulostriate artery have been gaining attention and interests for decades, from cadaver study to in vivo imaging1, because territory supplied by lenticulostriate arteries includes deep subcortical grey matter nucleus which pose vast influence on neurological function. Typically, ischemic lesions occurred when the main stem of middle cerebral artery (MCA) occlude since the LSA will be chocked with no blood flow. However, about 23% patients with MCA occlusion are asymptomatic2. There is little known about the changes of LSA and its relationship with the occluded MCA. Hence, we hypothesis that in patients with MCA stem occlusion who is free of ischemia, LSA may reshape in anatomy to maintain the blood supply of subcortical deep nucleus. We aimed to depict the pattern and morphometrical features of LSA in these patients.METHODS:
The study was a prospective observational study that was conducted in one center. Patients with unilateral MCA-M1 occlusion and no relating lesions in the LSA supply territory were recruited to perform 7T (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany, with 32Rx head coil in Research Mode) time-of-flight MRA. Patients who confirmed of Moyamoya disease were excluded. Imaging parameters: repetition time = 23.0 ms, echo time = 3.42 ms, spatial resolution = 0.3×0.3×0.3 mm3, FOV = 220×180 mm2, flip angle = 24°, bandwidth = 187 Hz/Px. The total scan time was 7 mins 40 s. High-resolution black-blood vessel wall imaging was also acquired to cross-confirm the arterial occlusion rather than stenosis. Reshaping was defined as the origination of LSA altered to a different location that was not identical to normal side or what had been reported in previous studies. The origination pattern of LSA were then categorized as proximal origination to the occlusion, distal origination to the occlusion. Absence of reshaping was defined as normal LSA anatomical type, and the origination was not altered to the distal or proximal end of the occlusion. The length, diameter, curvature, and number of LSA both in the lesional side and contralateral normal side were calculated by an in-house developed workflow and deep learning based algorithm3. Parameters of LSA were compared between lesional side and normal side by leveraging students’ t test or non-parametric test when appropriate.RESULTS:
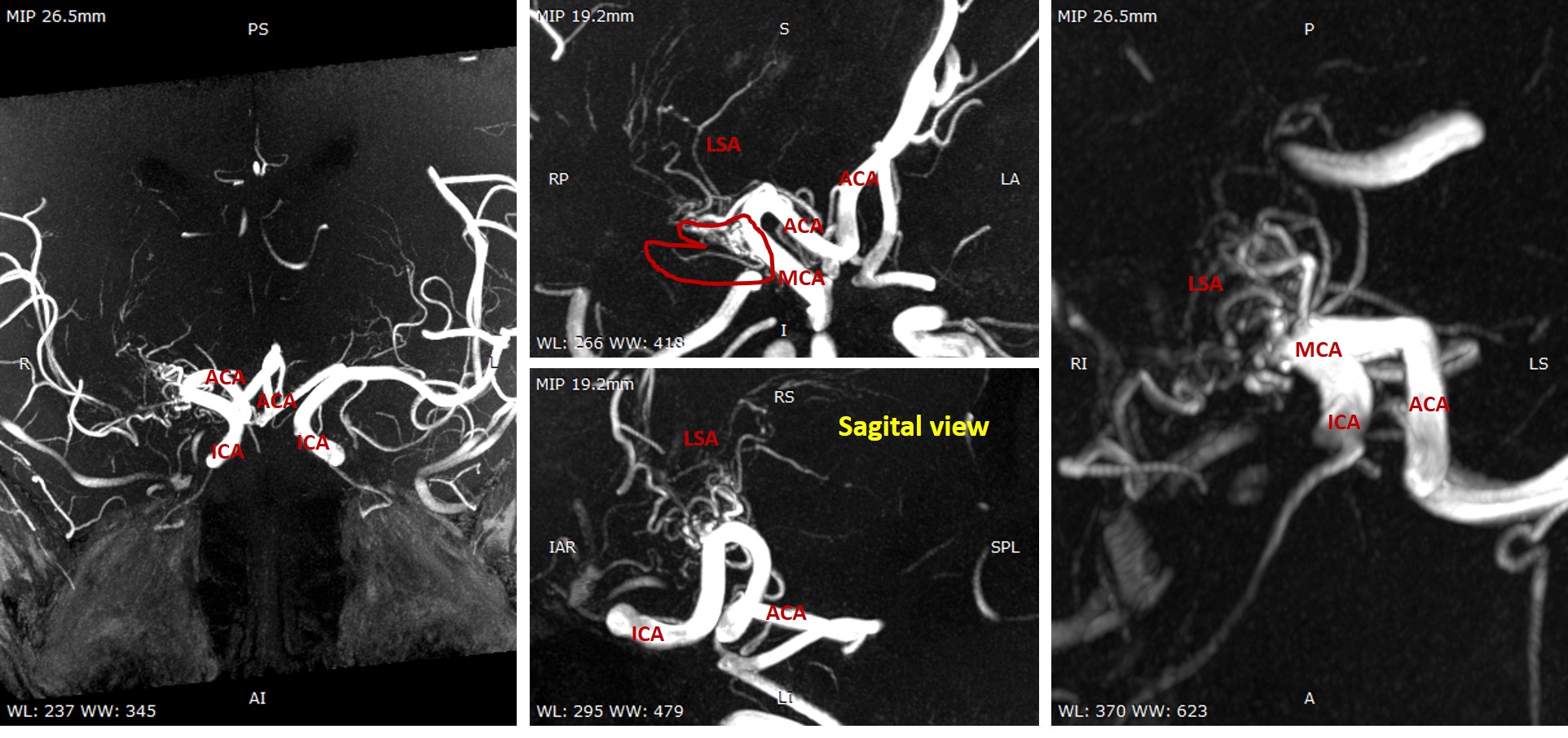
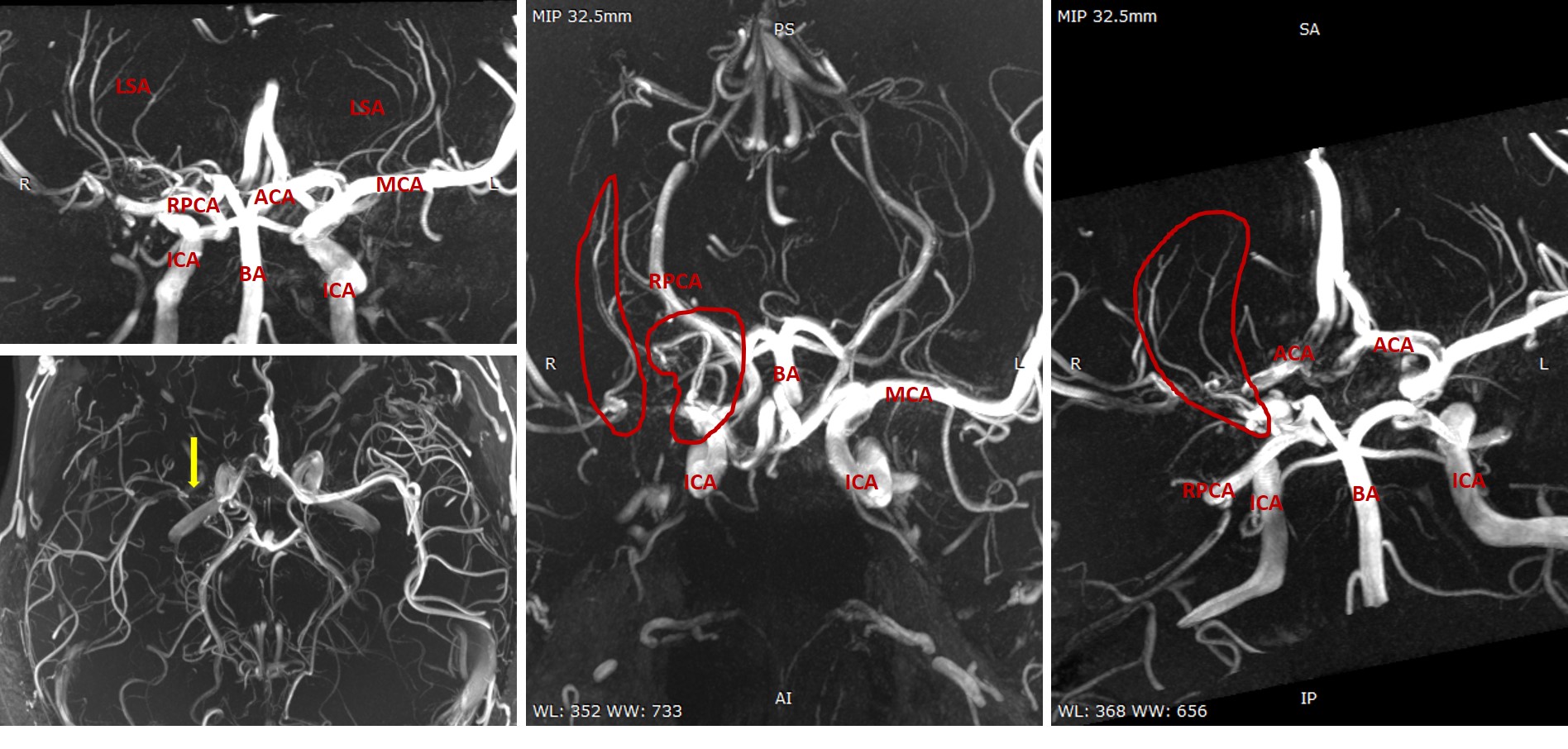
Nineteen patients were included in the analysis (Figure 1). 3 patients showed both the proximal and distal origination along the occluded segment. Totally, proximal origination was observed in 18/28, while distal origination was observed in 4/28 and 2/24 showed no reshaping origination. The number of LSA branches in each side was similar (21 versus 23, p=0.487). There were no significant differences between LSA of lesional side and normal side either in length (13.35mm versus 13.79mm, p=0.409) or in curvature (22° versus 26°, p=0.203), while the diameter in lesional side was significantly smaller than the normal side (0.19mm versus 0.21mm, p=0.028). Representative cases are shown in Figure 2-3.DISCUSSION:
Cadaver studies of LSA showed the anatomical knowledge in normal case and seldomly seen in MCA occlusion. These studies provide valuable reference for interpreting the imaging manifestations of LSA as well as its parent main trunk. The modification of LSA orifices may be considered as cerebrovascular reserve in the setting of intracranial artery occlusion. The end, especially the proximal end of the occlusion, was found to be the important location where modified LSA originated.CONCLUSION:
Reshaping of the origination of the lenticulostriate artery may be a key mechanism in blood supply hemostasis in MCA occlusion. Proximal reshaping is the most prevalent pattern in this condition. The finding may be helpful for the protection of LSA in endovascular procedure, and provide knowledge about the angiogenesis of middle cerebral artery. Future large sample size 7T MRI study is warranted.Acknowledgements
This work was supported by the National Natural Science Foundation of China (No.81825012, No. 82151309 to X.L. and No. 82271952 to J.H.L)References
1. Marinkovic S, Gibo H, Milisavljevic M, Cetkovic M. Anatomic and clinical correlations of the lenticulostriate arteries. Clin Anat. 2001;14(3):190-5.
2. Kang BS, Kwon HM, Ryu WS, et al. Prognosis of symptomatic and asymptomatic middle cerebral artery occlusion. Cerebrovasc Dis. 2008;26(5):489-93.
3. Zhixin Li, Dongbiao Sun, Yue Wu, et al. Small-patch CNN and random forest to model and quantify the lenticulostriate artery from 7T time-of-flight MR angiography, ISMRM 2022.
Figures