2208
Evaluation of altered vascular function in patients with unilateral middle cerebral artery stenosis at 7T-MRI1Department of Radiology, Chinese PLA General Hospital, Beijing, China, 2Research Collaboration Team, Siemens Healthineers, Beijing, China
Synopsis
Keywords: Blood Vessels, Brain
Motivation: It is important to understand the mechanisms underlying middle cerebral artery stenosis and detect altered vascular function prior to the alteration in brain parenchyma. 7T MRI, benefited from much increased signal-to-noise ratio
Goal(s): Evaluate vascular function in the affected and healthy middle cerebral arteries of patients with unilateral middle cerebral arterial stenosis.
Approach: 7T-MRI to assess blood flow velocities and pulsatility indices (PI).
Results: Flow velocity and PI in the middle cerebral artery were lower on the affected side than on the healthy side. These markers will facilitate mechanistic and interventional studies of middle cerebral artery stenosis.
Impact: Flow velocity and PI were lower on the affected side than on the healthy side in patients with middle cerebral artery stenosis. These findings may improve the understanding of middle cerebral artery stenosis pathogenesis.
Introduction
Stenosis of the middle cerebral artery (MCA) is a common cerebrovascular disorder that can lead to ischemic stroke and cognitive impairment. It is important to identify imaging biomarkers that can detect MCA stenosis before it causes irreversible damage to the brain tissue. One such biomarker is the blood flow velocity and pulsatility index (PI) of the MCA, which reflect the hemodynamic changes in the intracranial arteries1,2. Previous studies have used conventional MRI scanners to measure these parameters in patients with MCA stenosis, but the spatial resolution and signal-to-noise ratio may limit the accuracy and reliability of the measurements3. Therefore, we aimed to use a 7T-MRI scanner, which offers higher resolution and contrast, to measure the blood flow velocity and PI of the MCA in patients with unilateral MCA stenosis and compare them with the contralateral healthy side.Methods
Eight patients (age 61.00 ± 9.05 years, five men and three women), diagnosed with unilateral middle cerebral artery stenosis, were enrolled in this study. Demographic and vascular risk profiles were recorded for all participants. Stroke, hypertension, and diabetes statuses were recorded based on medical history. Inclusion criteria were magnetic resonance imaging findings of unilateral middle cerebral artery stenosis (including severe stenosis or occlusion of the middle cerebral artery, sometimes accompanied by infarction of the common carotid artery) and age >18 years. Exclusion criteria were contraindications to MRI scanning (e.g., metal implants, dentures, claustrophobia, contrast allergy, and renal failure). All the patients underwent MR examination in a whole-body 7T scanner (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany) equipped with an 8Tx/32Rx head coil. The MRI protocol included T1-weighted, T2-weighted, dark-fluid, time-of-flight MR angiography (TOF-MRA), and phase-contrast based velocity imaging (PC-Velocity) sequences. For PC-Velocity, a single slice was placed perpendicular to the middle cerebral artery (MCA) and was retrospectively gated with a peripheral pulse signal. The PC-Velocity utilized the following parameters: field of view 150 mm, acquisition matrix 432x432,slice thickness 2.0 mm, number of slices 30, flip angle 20-degree, echo time of 6.56 ms and repetition time of 40.88 ms. Mean blood flow velocities and PI, defined as the difference between the maximum and minimum velocity over mean velocity4, were calculated for the middle cerebral artery region. Statistical analyses were performed using SPSS version 26.0 (IBM Corporation, Armonk, NY, USA). Paired t-tests were utilized to compare changes in blood flow velocity between vessels on the affected and normal sides. Wilcoxon rank-sum tests were utilized to compare changes in PI between vessels on the affected and normal sides. Interobserver agreement concerning MRI interpretation was assessed using intraclass correlation coefficients5,6.Results
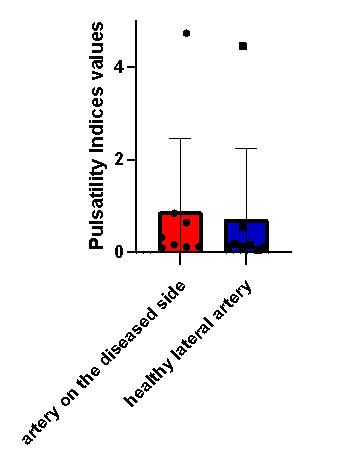
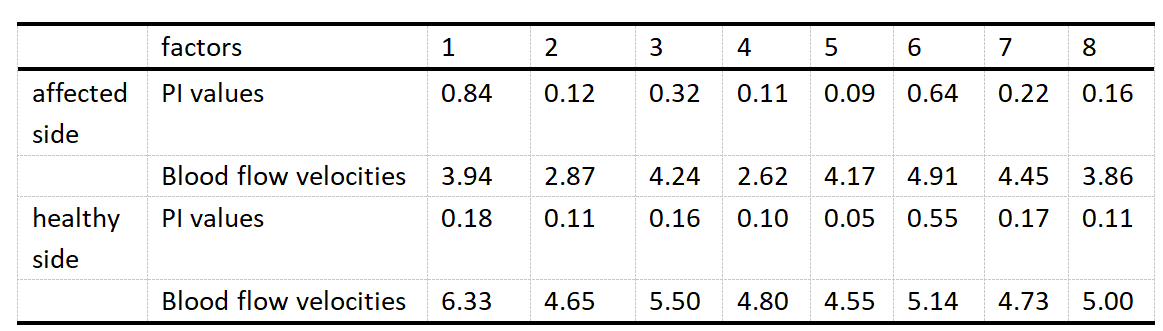
The mean blood flow velocity of the affected MCA was 3.88 ± 0.78 cm/s, which was lower than that of the healthy MCA (5.09 ± 0.59 cm/s). The mean PI of the affected MCA was 0.88 ± 1.58, which was higher than that of the healthy MCA (0.71 ± 1.51)(Table 1). Figure 1 shows the blood flow velocity trajectories of the MCA on both sides for each patient. Figure 2 shows a comparison of the PI between the affected and healthy side. The paired t-tests and Wilcoxon rank-sum tests did not show statistically significant differences in blood flow velocity (P = 0.21) and PI (P = 0.27) between the two sides, but there was a trend of lower velocity and higher PI on the affected side.Discussion and Conclusion
In this study, we used 7T-MRI to measure the blood flow velocity and PI of the MCA in patients with unilateral MCA stenosis. We found that the affected MCA had lower velocity and higher PI than the healthy MCA, suggesting impaired hemodynamics in the stenotic artery. These parameters may serve as potential imaging biomarkers for the early detection of MCA stenosis and the prevention of ischemic complications. However, our study had some limitations, such as the small sample size. Future studies with larger cohorts are needed to validate our findings and to explore the relationship between blood flow velocity, PI, and brain tissue changes in patients with MCA stenosis.Acknowledgements
This work was supported by the National Natural Science Foundation of China (No.81825012, No. 82151309 to X.L. and No. 82271952 to J.H.L)References
1.Wang Y, Zhao X, Liu L, et al. Prevalence and outcomes of symptomatic intracranial large artery stenoses and occlusions in China: the Chinese Intracranial Atherosclerosis (CICAS) Study. Stroke. 2014 Mar;45(3):663-669.
2.Saber H, Amiri A, Thrift AG, et al. Epidemiology of Intracranial and Extracranial Large Artery Stenosis in a Population-Based Study of Stroke in the Middle East. Neuroepidemiology. 2017;48(3-4):188-192.
3. van den Brink H, Kopczak A, Arts T, Onkenhout L, et al. CADASIL Affects Multiple Aspects of Cerebral Small Vessel Function on 7T-MRI. Ann Neurol. 2023 Jan;93(1):29-39.
4. Marieke van den Kerkhof, et al. Impaired damping of cerebral blood flow velocity pulsatility is associated with the number of perivascular spaces as measured with 7T MRI. JCBFM, 2023
5. Springer E, Dymerska B, Cardoso PL, et al. Comparison of Routine Brain Imaging at 3 T and 7 T. Invest Radiol. 2016;51(8):469-482.
6. Stahl R, Krug R, Kelley DA, et al. Assessment of cartilage-dedicated sequences at ultra-high-field MRI: comparison of imaging performance and diagnostic confidence between 3.0 and 7.0 T with respect to osteoarthritis-induced changes at the knee joint. Skeletal Radiol. 2009;38(8):771-783.
Figures