2205
Comparison of Time Efficiency Between CT and MRI Multimodal Scan for Patients with Acute Ischemic Stroke in the Late Window1The Affiliated Hospital of Northwest University·Xi’an No.3 Hospital, Xi'an, China, 2GE HealthCare MR Research, Beijing, China, Beijing, China
Synopsis
Keywords: Blood Vessels, Stroke, Acute ischemic stroke,Multimodal Scan,Time Efficiency
Motivation: The matter of time efficiency for both CT and MRI remains a topic of ongoing debate.
Goal(s): To provide an objective comparison of time efficiency between CT multimodal and MRI multimodal scans in patients with acute ischemic stroke in the late time window.
Approach: Efficiency in terms of time was compared between AIS patients who underwent CT scans and those who underwent MRI scans.
Results: The evaluation time for the MRI multimodal scan was found to be shorter than that of CT. MRI scans were recommended for use during the night shift. Furthermore, more experienced technicians had shorter scanning times.
Impact: Implementing this approach can streamline the scanning procedure for radiology departments when dealing with acute stroke patients, aid in the training of technicians, and recommend a preference for MRI scans during nighttime shifts.
1.Introduction
As the effectiveness of recanalization in acute ischemic stroke (AIS) is highly time-sensitive, expediting the workflow process becomes paramount[1,2]. Computed tomography (CT) is the most prevalent diagnostic modality due to its widespread availability and swift image acquisition. Nevertheless, magnetic resonance imaging (MRI) offers distinct advantages over CT in providing more comprehensive information. For example, diffusion-weighted imaging (DWI) excels in the early detection of acute ischemia and stroke-like events and serves as the gold standard for assessing the extent of infarct core, a pivotal factor in identifying patients eligible for endovascular treatment during extended time frames[3]. However, MRI has some inherent limitations, including the time required for screening for contraindications, restricted accessibility, additional time for patient preparation and table positioning, and longer scan duration. Yet, the issue of time efficiency for both CT and MRI continues to be a subject of debate. In this study, we aim to objectively compare the time efficiency of CT multimodal versus MRI multimodal scan in late window AIS patients.2.Methods
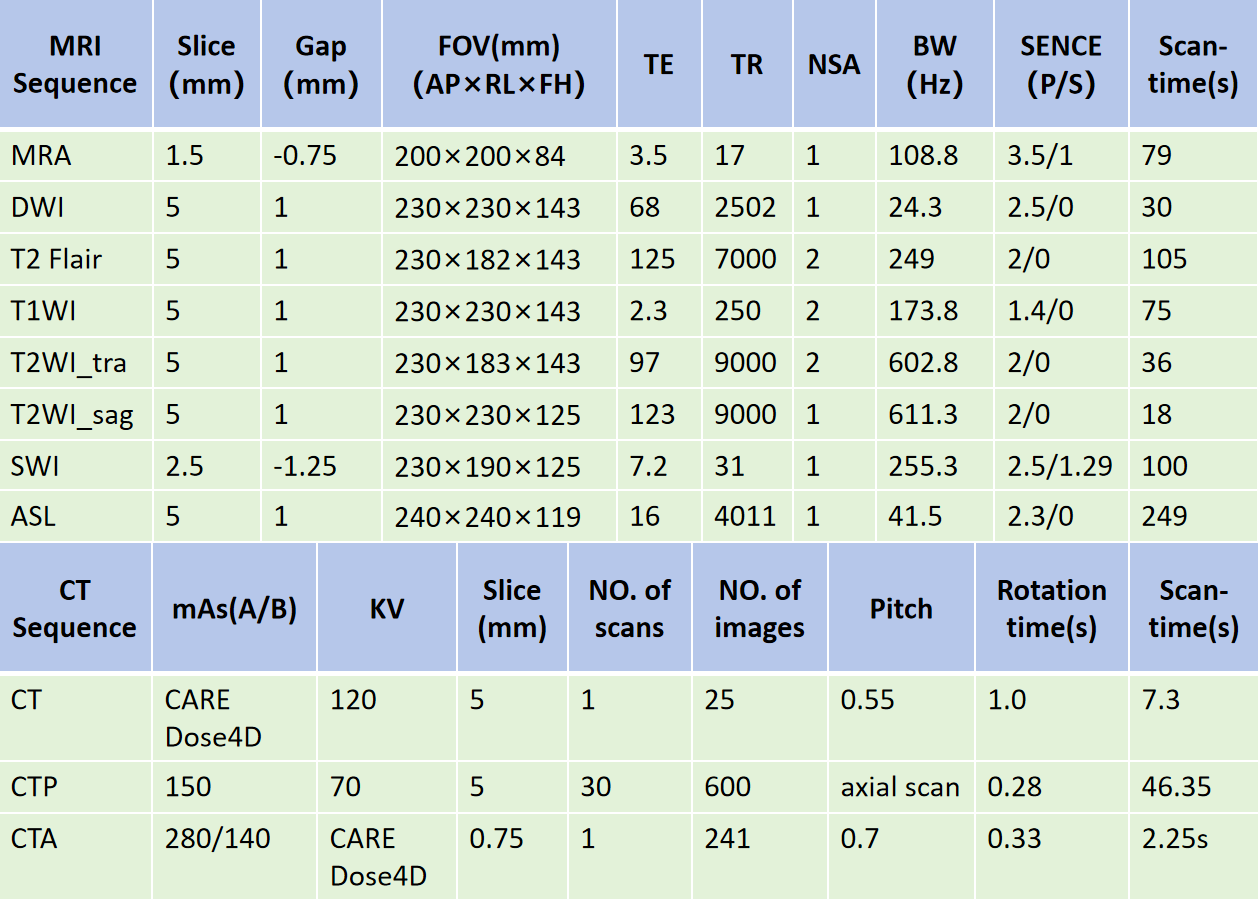
Participants: This retrospective study has been approved by the Ethics Committee of our Hospital, which eliminates the requirements of the informed consent. From December 2020 to July 2023, a total of 108 patients with late-window acute ischemic stroke were collected, including 85 cases of MRI and 23 cases of CT. Among them, there were 66 males and 42 females, with an average age of 65.5 (ranging from 37 to 91 years old).Radiological Data: The imaging devices employed in our investigation consist of a dual-source CT system and a 3.0T MRI scanner equipped with a 16-channel head coil. The CT scanning protocol encompassed non-contrast CT, Cerebral Perfusion CT (CTP), and CT Angiography (CTA), while the MRI scanning protocol encompassed MRA, DWI, MRI, SWI, and ASL. Detailed scanning parameters can be found in Table 1.
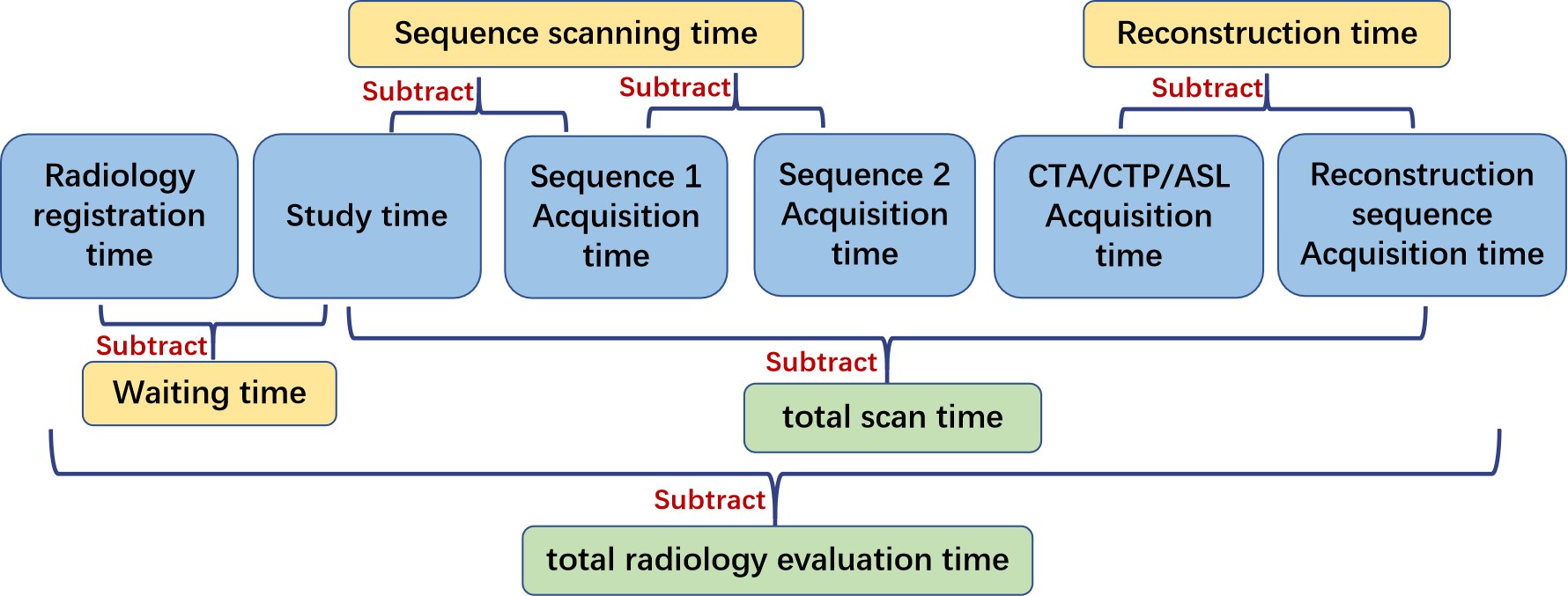
Time Efficiency Measurement: For CT and MRI multimodal scans, the study time, acquisition time, and reconstruction time of each sequence are extracted from the DICOM source data. Then calculate the patient’s waiting time, the time required for each sequence scan, the total scan time, and the total radiology evaluation time (Figure 1).
Statistical Analysis: Statistical analysis of the aforementioned data was conducted using SPSS statistical software, employing the Mann-Whitney U test, followed by visualization of the statistical results.
3.Results
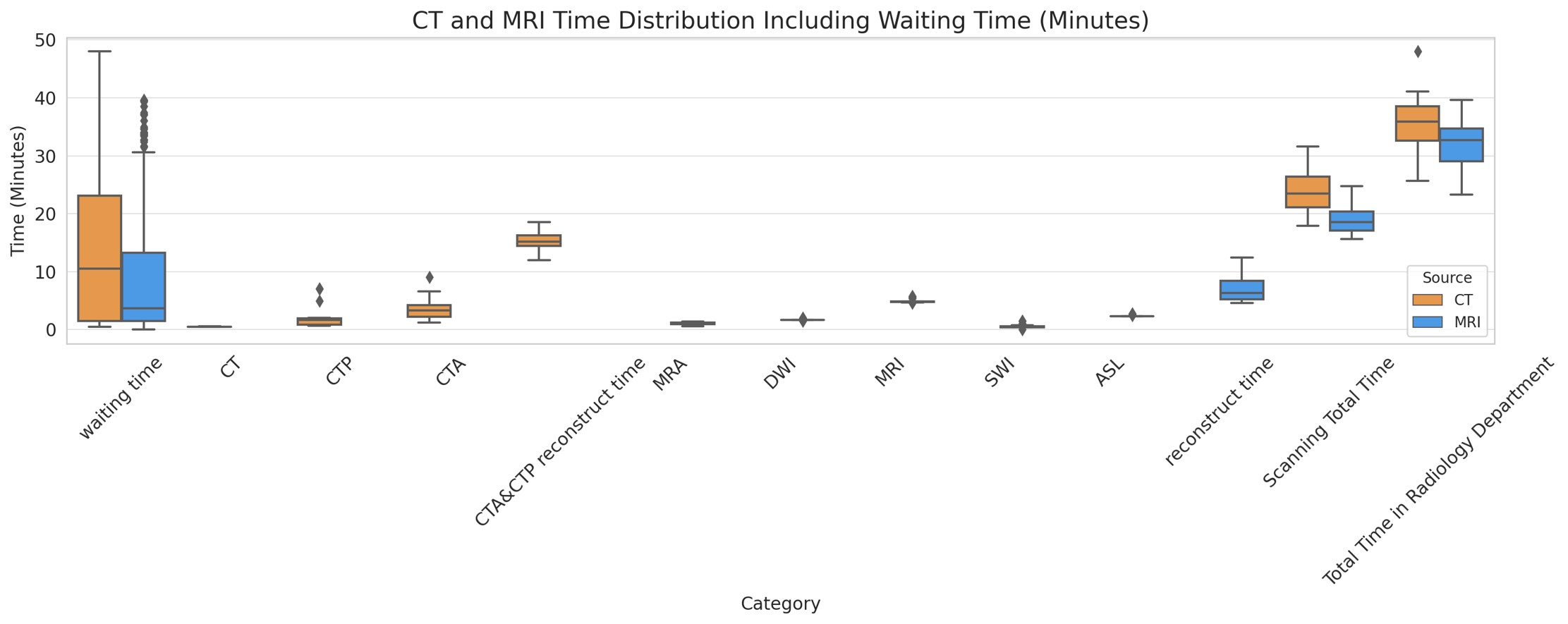
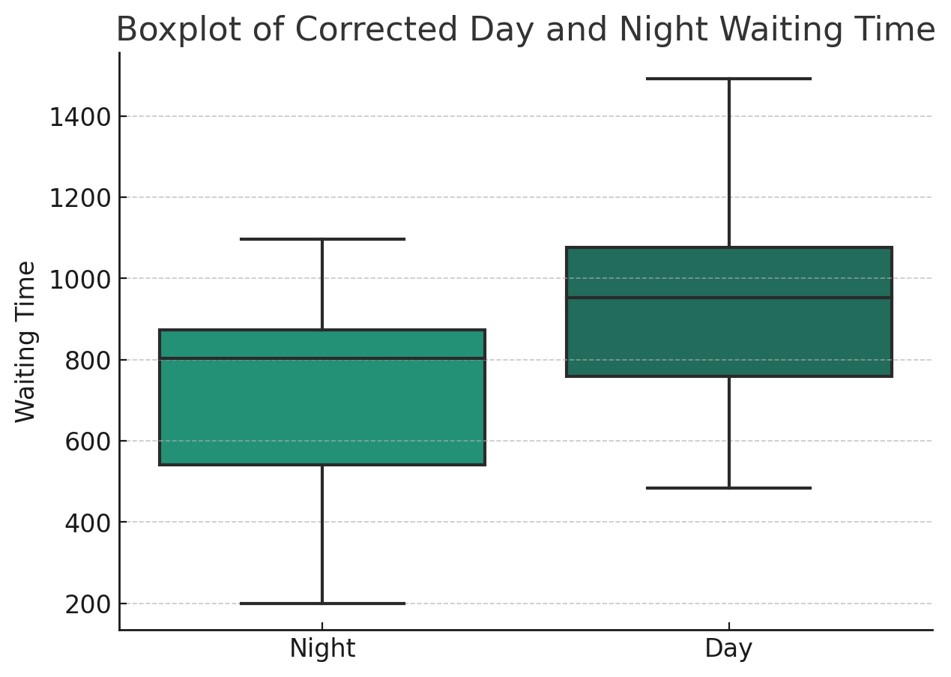
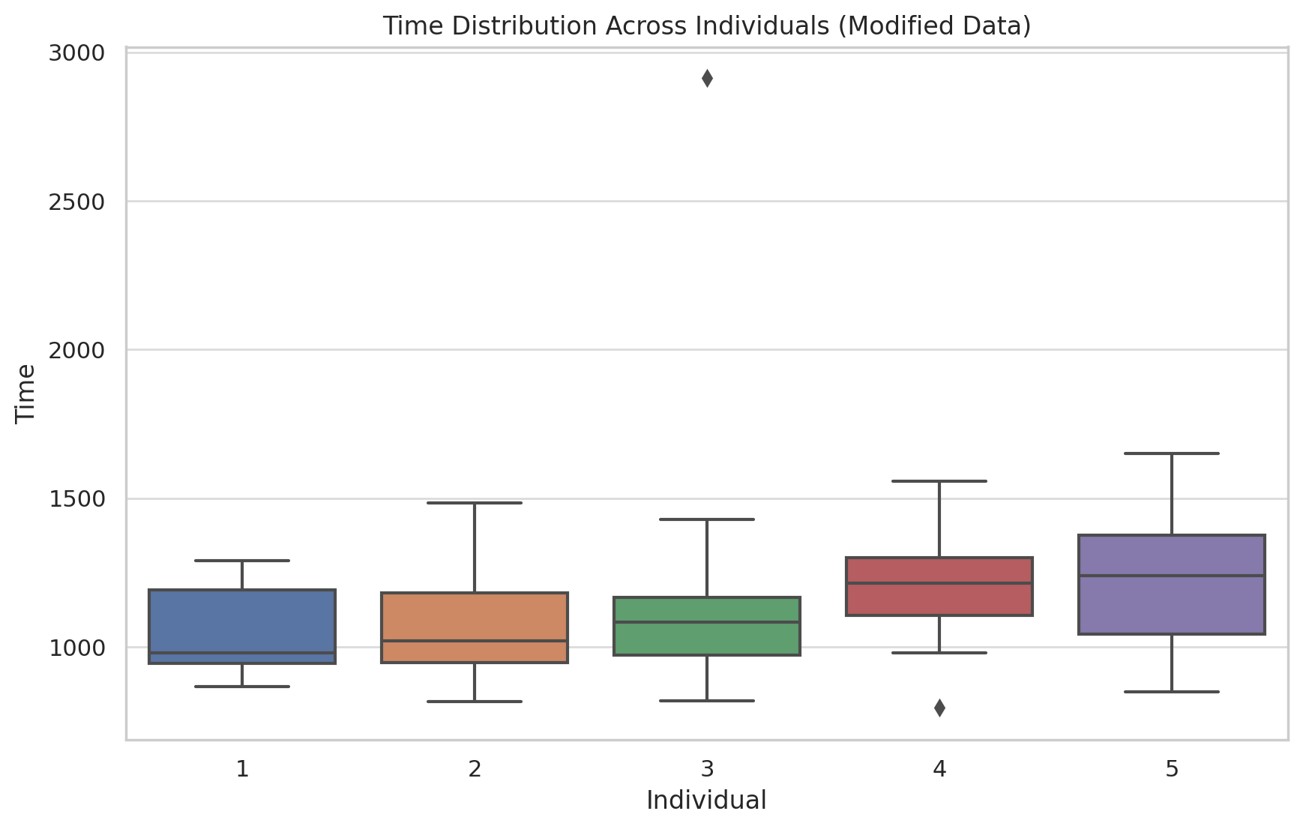
Main results are summarized in Figure 2. The sequence reconstruction time was longer for CT than MRI (p<0.05), but the total scanning time and radiology evaluation time were longer for CT than MRI (p<0.05) (Fig2.a). Additionally, daytime patients had longer waiting time than nighttime patients (p<0.05) (Fig2.b), Furthermore, we observed significant differences in scanning time between different technicians (p<0.05) (Fig2.c).4.Discussion
The objective of this study was to assess the time efficiency of CT and MRI multimodal scans in patients diagnosed with acute ischemic stroke (AIS). Our results demonstrate that MRI multimodal scans exhibit a longer total sequence time compared to CT scans. However, the reconstruction time for MRI is shorter, ultimately resulting in higher overall time efficiency when compared to CT. These findings have significant implications for the radiological diagnosis of acute stroke, particularly during the late window period recommended by acute stroke guidelines. Furthermore, MRI multimodal scans offer the advantage of providing additional diagnostic information, and as technology continues to advance, the scanning time for MRI is anticipated to be further reduced[4].Additionally, our study revealed that the implementation of the green channel system effectively minimized the waiting time disparity between CT and MRI multimodal scans. However, it is noteworthy that MRI demonstrated higher time efficiency during nighttime, potentially due to increased patient volume or limited resource allocation during daytime hours. Moreover, we observed a significant correlation between the technician's expertise and scanning time, aligning with previous research findings[5]. Consequently, it is crucial for radiology management to enhance technician training programs to optimize work efficiency and enhance patient satisfaction.
Finally, our study highlights the importance of considering multiple factors in the selection of imaging modes for acute stroke assessment, including imaging time, technician experience, and time period. However, future research should focus on evaluating imaging quality, diagnostic accuracy, and their impact on the clinical prognosis of patients.
5.Conclusion
For patients in the late window of acute stroke, MRI multimodal scanning may have advantages in time efficiency and imaging diagnosis over CT multimodal scan, especially during the night shift. Meanwhile, the experience of technicians provide important references for the optimization of radiology workflow.Acknowledgements
In the process of writing this paper, I would first like to express my deepest gratitude to Mr. Gao Yanjun, the director of my department at the hospital where I work, for his valuable comments and suggestions on my research. In addition, I would like to extend my special thanks to the Third Hospital of Xi’an City for providing me with an excellent platform for scientific research. I am also grateful to all the patients for their cooperation. Lastly, I would like to thank my family for their understanding and support of my work.References
[1] Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, Jauch EC, Kidwell CS, Leslie-Mazwi TM, Ovbiagele B, Scott PA, Sheth KN, Southerland AM, Summers DV, Tirschwell DL. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2019 Dec;50(12):e344-e418. doi: 10.1161/STR.0000000000000211. Epub 2019 Oct 30. Erratum in: Stroke. 2019 Dec;50(12):e440-e441. PMID: 31662037.
[2] Akbarzadeh, M.A., Sanaie, S., Kuchaki Rafsanjani, M. et al. Role of imaging in early diagnosis of acute ischemic stroke: a literature review. Egypt J Neurol Psychiatry Neurosurg 57, 175 (2021).
[3] Lansberg MG, Albers GW, Beaulieu C, Marks MP. Comparison of diffusion-weighted MRI and CT in acute stroke. Neurology. 2000 Apr 25;54(8):1557-61. doi: 10.1212/wnl.54.8.1557. PMID: 10762493.
[4]Provost C, Soudant M, Legrand L, Ben Hassen W, Xie Y, Soize S, Bourcier R, Benzakoun J, Edjlali M, Boulouis G, Raoult H, Guillemin F, Naggara O, Bracard S, Oppenheim C. Magnetic Resonance Imaging or Computed Tomography Before Treatment in Acute Ischemic Stroke. Stroke. 2019 Mar;50(3):659-664. doi: 10.1161/STROKEAHA.118.023882. PMID: 30744542.
[5] Brunnquell CL, Avey GD, Szczykutowicz TP. Objective Evaluation of CT Time Efficiency in Acute Stroke Response. J Am Coll Radiol. 2018 Jun;15(6):876-880. doi: 10.1016/j.jacr.2018.01.011. Epub 2018 Feb 19. PMID: 29467093.
Figures