2195
White matter hyperintensities: A MRI marker of brain injury in patients with Cardiovascular diseases1Department of Radiology, Chinese PLA General Hospital, Beijing, China, 2Department of cardiology, Chinese PLA General Hospital, Beijing, China
Synopsis
Keywords: Blood Vessels, White Matter
Motivation: Cardiovascular disease (CVD) is closely related to cerebrovascular injury. However, even when the ejection fraction (EF) is normal, the cardiac microvascular system may still be abnormal.
Goal(s): Explore the relationship between CVD with preserved EF and cerebrovascular injury.
Approach: The heart and brain MRI of the participants were scanned with 3.0T MRI scanner. Different cardiac ejection parameters and high signal images of white matter were obtained.
Results: Patients with CVD, when EF is normal, are still associated with WMH and are still a risk factor for brain injury.
Impact: t is crucial to pay early attention to the early indicators of cerebrovascular abnormalities in patients with heart failure, as timely intervention is essential for reducing the risk of stroke.
Introduction
Increasing incidence and prevalence rates of cerebrovascular diseases have been observed globally, maintaining a consistently high level [1]. There is a close association between cardiovascular diseases (CVD) and vascular brain injuries[2]. Severe CVD was related to subclinical brain injuries such as lacunar infarcts and white matter hyperintensities(WHM)[3]. However, even in cases with normal ejection fraction (EF), abnormalities can still occur in the cardiac microvasculature. Hence, exploring the relationship between CVD with preserved EF and cerebrovascular diseases is crucial for a deeper understanding of their manifestations on brain magnetic resonance imaging (MRI). WMH considered markers of vascular brain injury clinically, are increasingly observed on MRI scans and have become more prevalent[4]. Therefore, we collected preserved EF in CVD patients to explore the relationship between this and WMH.Methods
Cardiac and brain MRI were acquired using a 3.0 T scanner (Philips) with 16-channel body phased array coil and 32-channel head coil. The cardiac protocol included short-axis multislice cine steady-state free precision (TR 3.2 ms; TE 1.61; flip angle 45°; breath-hold; number of slices dependent on size of LV (range 10–12 slices), resolution 1.8 × 1.79 × 8.0 mm3). The brain MRI protocol included fluid-attenuated inversion recovery (FLAIR) images (TR 4800 ms; TE 310 ms; TSE factor 162, resolution 0.6 × 0.8 × 6 mm3).The participants the following parameters were derived from MRI by an experienced neurologist: the EF was using a semi-automatic contour detection with manual correction: Left ventricular-end diastolic volume (LV-EDV) and left ventricular end-systolic volume (LV-ESV). FLAIR sequences were used for identifying WMH. The Fazekas score is a visual rating of WMH.
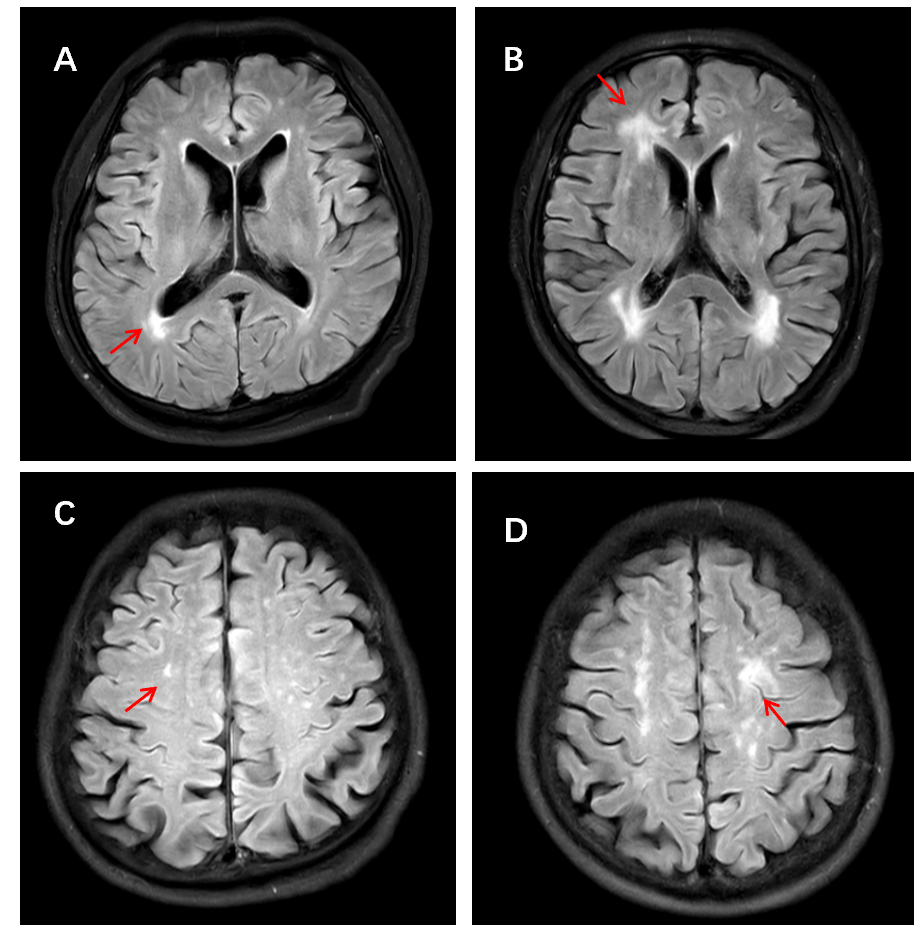
WMH was based on the STandards for ReportIng Vascular changes on Euroimaging (STRIVE)[5]. The severity of WMH is rated by using the Fazekas score (the scale ranges from 0 to 3), which reflects the overall burden of WML[5].WMH were classified as deep and periventricular and assessed with a validated four-point visual rating scale (0 = none; 1 = 1–10; 2 = 11–20; 3 = 21–40; and 4=>40) (Figure 1). We calculated the total WMH score as the sum of the periventricular and deep WMH scores.
The purpose of this study was to explore the relationship between CVD with preserved EF and WMH. Participants were required to meet the following conditions: (1) underwent cardiac and brain examinations, (2) had no MRI contraindications, and (3) had no previous stroke or peripheral vascular disease. And the case group was diagnosed with CVD.
Continuous variables are given as mean ± standard deviation (SD) and as percentages for categorical variables. Student’s t-test were used for continuous variables. Categorical data are given as numbers of patients (%) and were compared using χ2 test or Fishers’ exact test.
Results
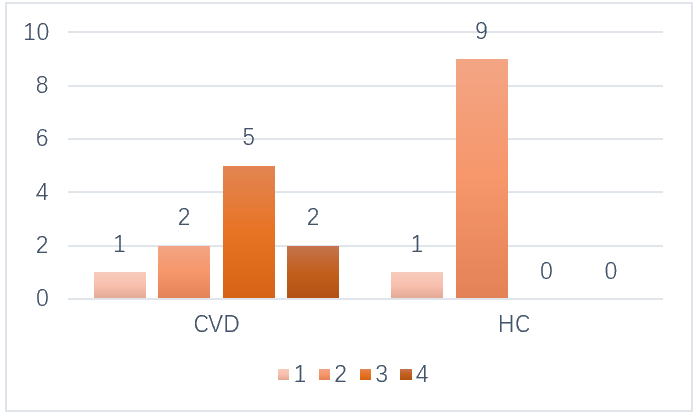
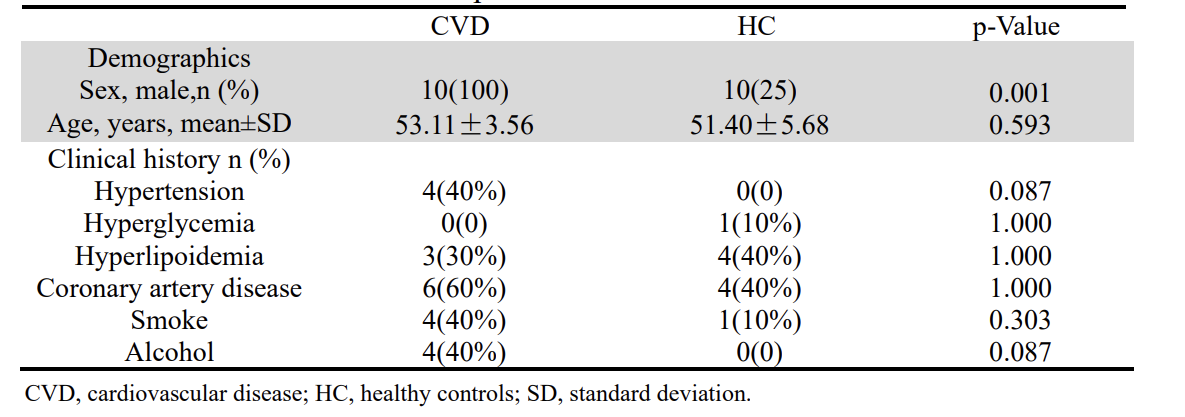
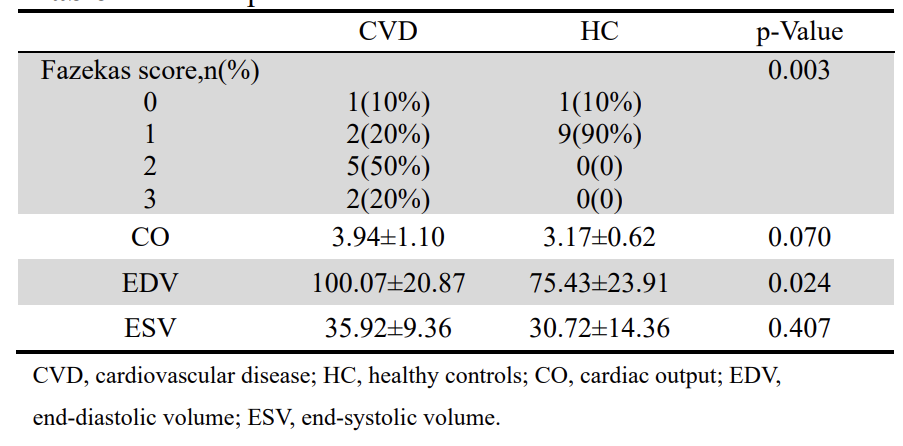
A total of 20 individuals were included in the full analysis. They did not suffer from stroke or peripheral vascular diseases. For further analysis, patients were stratified into two groups: EF-preserved CVD Group and Healthy Controls (HC). Patients with CVD were without women and had similar vascular risk factors with HC. Patients with CVD BMI was obviously higher than HC (Table 1).In patients with CVD, there is a significant correlation between the presence of WMH and EF (P=0.003). Compared to HC, a higher proportion of individuals with higher Fazekas scores were observed in the CVD group (Figure 2). In terms of other cardiac parameters (Table 2), such as cardiac output (CO), end-diastolic volume (EDV), and end-systolic volume (ESV), a statistical difference was found for EDV (P=0.26
Discussion and Conclusion
In the presence of normal EF, there may still be cardiac microvascular abnormalities, which can trigger an inflammatory response in the body, stimulating endothelial cell inflammation and increasing oxidative stress, leading to vascular dysfunction[6]. WMH, as markers of vascular brain injury, are widely observed in patients with cardiovascular disease and older individuals. This study found a correlation between the severity of WMH and CVD Therefore, even with normal EF, CVD remains a risk factor for WMH-related brain damage.Acknowledgements
This work was supported by the National Natural Science Foundation of China (No.81825012, No. 82151309 to X.L. and No. 82271952 to J.H.L)References
[1] CHEN W, LI Z, ZHAO Y, et al. Global and national burden of atherosclerosis from 1990 to 2019: trend analysis based on the Global Burden of Disease Study 2019 [J]. Chin Med J (Engl), 2023, 136(20): 2442-50.
[2] HAVAKUK O, KING K S, GRAZETTE L, et al. Heart Failure-Induced Brain Injury [J]. J Am Coll Cardiol, 2017, 69(12): 1609-16.
[3] HILAL S, CHAI Y L, VAN VELUW S, et al. Association Between Subclinical Cardiac Biomarkers and Clinically Manifest Cardiac Diseases With Cortical Cerebral Microinfarcts [J]. JAMA Neurol, 2017, 74(4).
[4] HASSELL M E, NIJVELDT R, ROOS Y B, et al. Silent cerebral infarcts associated with cardiac disease and procedures [J]. Nat Rev Cardiol, 2013, 10(12): 696-706.
[5] WANG X, LYU J, MENG Z, et al. Small vessel disease burden predicts functional outcomes in patients with acute ischemic stroke using machine learning [J]. CNS Neurosci Ther, 2023, 29(4): 1024-33.
[6] RUSSO C, JIN Z, HOMMA S, et al. Subclinical Left Ventricular Dysfunction and Silent Cerebrovascular Disease [J]. Circulation, 2013, 128(10): 1105-11.
Figures