2193
Comparison of whole-brain cerebrovascular reactivity mapping measured by resting-state and carbogen-based BOLD fMRI for moyamoya disease1Department of Radiology, Taipei Veterans General Hospital, Taipei, Taiwan, 2Institute of Brain Science, National Yang Ming Chiao Tung University, Taipei, Taiwan, 3Department of Medical Research, Taipei Veterans General Hospital, Taipei, Taiwan
Synopsis
Keywords: Blood Vessels, fMRI (resting state), cerebrovascular reactivity
Motivation: Mapping of cerebrovascular reactivity (CVR) using resting-state BOLD fMRI (RS-fMRI) was raised in 2017 and 2021 with verification using the moyamoya disease (MD). But pathological hemodynamics of MD was missing by RS-fMRI.
Goal(s): Arterial stealing phenomenon can be demonstrated by carbogen-based fMRI (CO2-CVR), but not by RS-fMRI.
Approach: Both RS-CVR and CO2-CVR using a 3T MR and an automatic delivery system of carbogens were acquired for eleven subjects and ten patients with MD. Bland-Altman plots was applied for both RS-CVR and CO2-CVR.
Results: By using CO2-CVR, unique negative CVR of MD verified the arterial stealing phenomenon which was missed by RS-CVR.
Impact: Arterial stealing phenomenon of moyamoya disease/syndrome can be demonstrated as negative cerebrovascular reactivity by carbogen-based fMRI (CO2-CVR), but not by resting-state fMRI (RS-CVR).
Introduction
Non-invasive mapping of cerebrovascular reactivity (CVR) using resting-state blood-oxygenation-level-dependent (BOLD) fMRI (RS-CVR) was raised in 2017 and 2021 [1,2] with clinical verification using the disease model of moyamoya disease/syndrome (MD). But information of pathological hemodynamics for MD was missing with CVR measured by RS-CVR. Arterial stealing phenomenon, associated with moderate to severe stenosis of individual arterial branch of circle of Willis, caused negative CVR using carbogen-based fMRI (CO2-CVR) [3]. In this study, MD patients with critical hemodynamics as verified by negative CVR using CO2-CVR and increase of oxygen extraction fraction (OEF) using task-based fMRI was selected for comparison of the CVR mapping using RS-CVR and CO2-CVR.Database and Methods
1. Eleven normal subjects (25±4, M/F:6/5) and ten patients of moyamoya disease (32±12, M/F:5/5; before and after external carotid/internal carotid bypass (EC-IC bypass)) were included for this MRI study using a 3T MR with written IRB-proved consent forms. Head fixation was obtained by soft pads. Gas delivery to subject (air or 1~5% carbogen) was designed by a non-rebreathing mask with a custom-designed automatic switching system. Subjects were instructed to close their eyes during study.2. FID-EPI (TR/TE/flip angle = 2000ms/30ms/90 degrees, matrix size = 3.6x3.6x4mm) were applied for CO2-CVR (NR=360), RS-CVR (NR=200) and task-based BOLD-based fMRI with scan time ~12 minutes, ~ 6.7 minutes and 4 minutes, respectively. Structural images (T1-weighted FSPGR images with inversion preparation, TR/TE/TI//flip angle = 8.2ms/3.2ms/450ms/12 degrees, 0.9 mm isotropic matrix) was also obtained.
3. CO2-CVR:Inclusion criteria by the off-line/on-line real-time fMRI analysis were translational motion < 1 mm and rotation < 1 degree. After standard preprocessing (slice-timing, re-alignment, co-registration and normalization) using SPM12, Carbogen Response Function (CRF) was derived from Infomax ICA algorithm based on (1) data reduction by principal component analysis, (2) minimum length description and (3) correlation analysis of the temporal profiles using the recorded end-tidal CO2. Final CRF was obtained using the weighted summation of components with correlation >0.3. General linear model (GLM) and contrast of resting-state fMRI with design matrix of “head motion” + ”CRF” for generating voxel-based t-map using SPM12.
4. RS-CVR: Band–pass filter (0-0.1164 Hz, [2]) was integrated into the data processing using DPARSF (Data Processing Assistant for Resting-State fMRI) package with (RS-Reg-CVR) or without (RS-NoReg-CVR) nuisance regressors (head motion and averaged signals of white matter/cerebrospinal fluid). With brain mask of EPI, the mean time course (TC) of whole brain was derived. General linear model (GLM) and contrast of resting-state fMRI with design matrix of “head motion” + ”mean TC” was applied for generating voxel-based t-map.
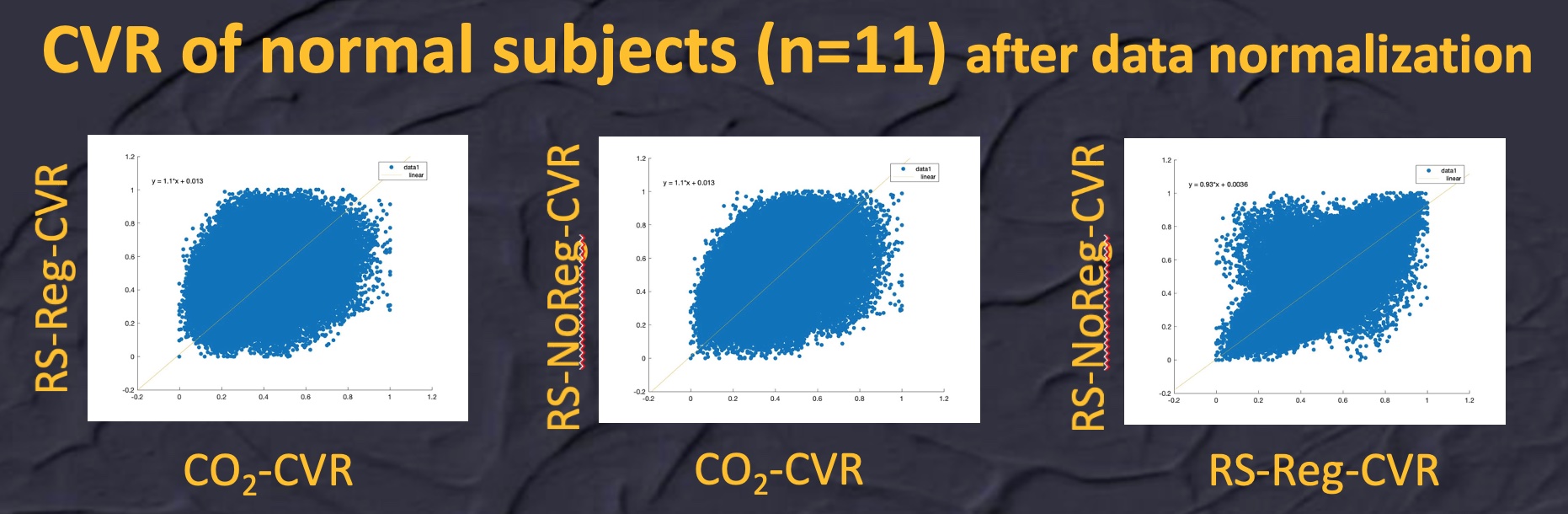
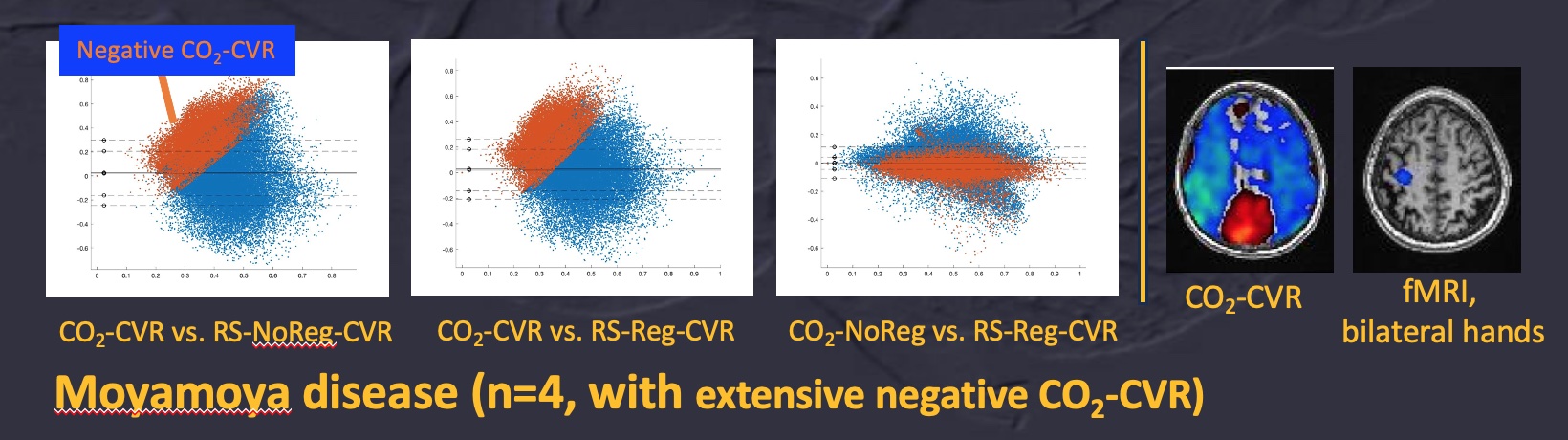
5. Optimal mask of data analysis for each subject was obtained using (1) gray/white matters of structural images using ”segment” batch of SPM12 with tissue probability of 0.4 and (2) mean EPI image. Under the optimal mask, scatter and Bland-Altman plots were obtained using MATLAB (R2018a) by merging all data of normal subjects or moyamoya syndrome with data normalization of each subject/patient [Xnew=(X-Xmin) / (Xmax-Xmin)]. For demonstrating the effects of impaired CO2-CVR in Bland-Altman plots, 4 patients with extensive territorial defects of CO2-CVR were selected from 10 patients.
6. Task-based BOLD fMRI was obtained by the block-designed paradigm and synchronized visual projection with MRI. Standard protocol using SPM12 was used for data analysis with the statistical criteria of p<0.001.
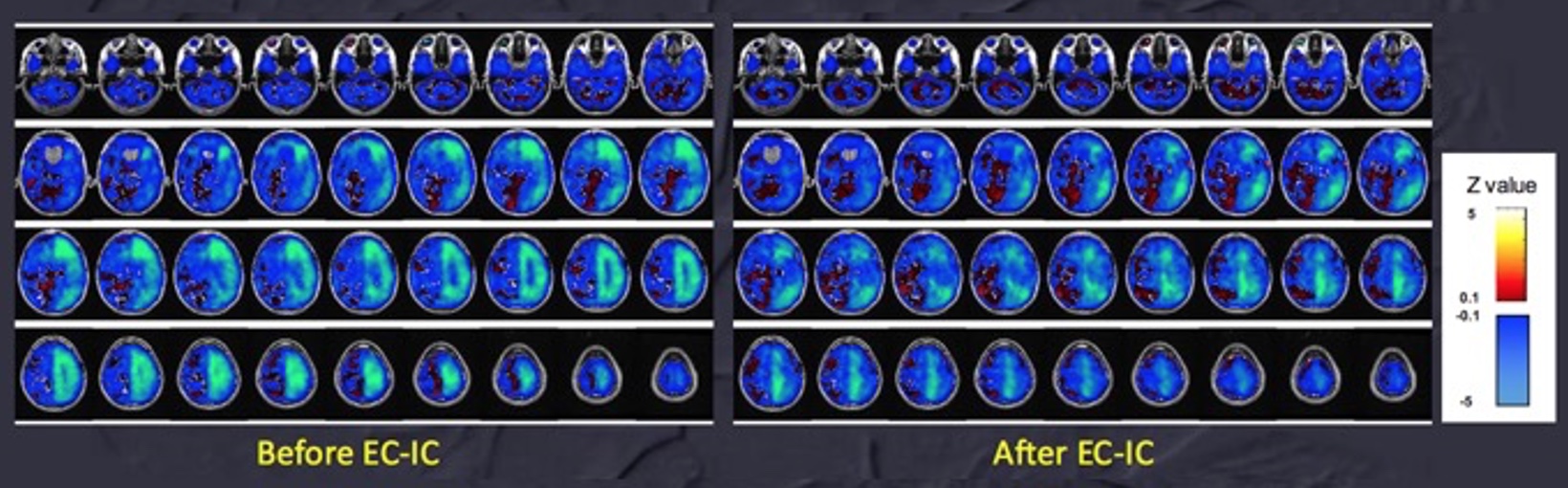
7. Brain cloud of CO2-CVR:126 normal subjects received the studies of CO2-CVR in 2010-2012. And the ad hoc normative control database of 90 subjects [45 male subjects (24.8 +/- 3.0 years old, mean +/- one standard deviation) and 45 female subjects (23.4 +/- 3.2 years old)] were constructed for z-mapping of CO2-CVR (|z|>3) with less confounding effects of head motion (the maximal translation and rotational displacement of head less than 1 mm and 1 degree, respectively).
Results
Data of normal subjects showed good correlation between CO2-CVR and rs-fMRI CVR by normalized scatter plots [Figure 1]. By Bland-Altman plots of four MD patients with moderate-to-severe arterial stenosis, negative CO2-CVR in compromised arterial territories suggested pathological hemodynamics of arterial stealing phenomenon which was missed by RS-CVR [Figure 2]. And longitudinal follow-up using the brain cloud of CO2-CVR of normal subjects (N=90) demonstrated the partial normalization of CO2-CVR after successful external carotid/internal carotid bypass (EC-IC bypass) [Figure 3].Discussion and Conclusion
Unique territorial negative CO2-CVR of MD patients demonstrated the pathological hemodynamics of arterial stealing phenomenon which was missed by RS-CVR. By combining task-based fMRI for demonstrating increase of OEF in compromised arterial territory, the CO2-CVR may guide the surgical intervention, which can be monitored by CO2-CVR using our brain cloud of CO2-CVR.Acknowledgements
Authors appreciated the grant supports from MOST, NHRI and Taipei VGH of Taiwan.References
1.Liu et al, Cerebrovascular reactivity mapping without gas challenges, Neuroimage (2017), 146, 320-326
2.Liu et al, Cerebrovascular reactivity mapping using resting-state BOLD functional MRI in healthy adults and patients with moyamoya disease, Radiology (2021) 299, 419-425
3.Arteaga et al, The vascular steal phenomenon is an incomplete contributor to negative cerebrovascular reactivity in patients with symptomatic intracranial stenosis, JCBFM (2014) 34, 1453-1462
Figures