2187
Arterial Spin Labeling and Phase-Contrast MRI suggest impaired cerebral blood flow autoregulation in cerebral small vessel disease1Department of Radiology & Nuclear Medicine, Maastricht University Medical Centre, Maastricht, Netherlands, 2School for Mental Health and Neuroscience (MHeNs), Maastricht University, Maastricht, Netherlands, 3Department of Neurology, Maastricht University Medical Centre, Maastricht, Netherlands, 4School for Cardiovascular Diseases (CARIM), Maastricht University, Maastricht, Netherlands, 5Department of Electrical Engineering, Eindhoven University of Technology, Eindhoven, Netherlands
Synopsis
Keywords: Blood Vessels, Perfusion, Small vessel disease
Motivation: Largely unidentified pathophysiological mechanisms in cerebral small vessel disease (cSVD) hamper treatment development. One of the potentially affected functions is cerebral blood flow (CBF) autoregulation.
Goal(s): Establish whether brain tissue perfusion is (in)dependent of macrovascular blood supply in cSVD patients.
Approach: The relationship between internal carotid artery blood flow (blood supply), measured with phase-contrast MRI, and gray matter CBF (CBFGM), measured with arterial spin labeling, was determined separately for cSVD patients (n=41) and controls (n=18).
Results: A significant, positive relationship between CBFGM and blood supply was found in cSVD patients, but not in controls, suggesting impaired autoregulation in cSVD.
Impact: We revealed a positive relationship between internal carotid artery blood supply and the cerebral blood flow in gray matter in cerebral small vessel disease patients, but not in controls, which could indicate compromised autoregulatory capacity.
Introduction
Cerebral small vessel disease (cSVD) is a disorder of the brain microvasculature and can lead to cognitive impairment and/or stroke1, 2. Malfunction of the neurovascular unit (NVU) has been associated with cSVD and contributes to several types of dementia3. The NVU is unit comprising endothelial cells, pericytes, smooth muscle cells, glial cells and neurons3. One of the potentially compromised functions of the NVU in cSVD is cerebral autoregulation. Cerebral autoregulation represents the brain’s ability to maintain a steady cerebral blood flow (CBF) even when confronted with variations in systemic blood pressure (BP) and/or blood supply, ensuring stable and adequate tissue perfusion4. Unfortunately, the exact underlying mechanisms of NVU dysfunction in cSVD are still unknown, which is a considerable hurdle towards cSVD specific therapy development3. In order to deepen our insight into the hemodynamics and autoregulation in cSVD patients, we aimed to study the relationship between blood supply by the internal carotid arteries (ICA) and the CBF in the gray matter.Methods
Study population: We recruited 41 patients with vascular cognitive impairment (VCI) due to cSVD (mean age (SD) = 70 (9) years, 13 females) and 18 healthy age-matched controls (HC) (mean age (SD) = 68 (7) years, 6 females). Only the cSVD patients had objective cognitive decline (MoCA<26 or cognitive impairment in at least 1 cognitive domain in neuropsychological assessment), and imaging evidence of cSVD (Fazekas ≥ 2 or Fazekas 1 and lacunar infarcts/microbleeds).Image acquisition: We acquired structural images, pCASL, and phase-contrast MRI (PCMRI) of both ICAs for all participants on a 3T Philips Achieva MRI scanner. For the pCASL scans, 5 control-label pairs were acquired with a 3D readout, together with a proton density image. The labelling plane was positioned perpendicular to the ICAs on a vessel scout. We used a post labeling delay (PLD) of 2500ms, as we observed an underestimation of the CBF when using the recommended PLD of 2000ms, because of the slower hemodynamics in cSVD5, 6. Figure 1 shows examples of both post labeling delays. PCMRI was acquired at the same location as the labeling plane of the pCASL scan. Table 1 shows an overview of all scan parameters.
Image analyses: The gray matter (GM) was segmented using the structural images (Freesurfer7). CGM CBF was calculated using FSLBASIL with correction for motion and partial volume effects8, 9. Masks were manually drawn in the ICAs using the magnitude images10. ICA blood flow was obtained by multiplying the mean velocity with the cross-sectional area of the ICAs. Figure 2 shows an example of the ICA blood flow calculation.
Statistical analyses: Group differences in CBF in GM (CBFGM) and mean blood flow of both ICAs were tested using independent samples t-tests. The mean±SD CBFGM and ICA flow was reported for both groups. To investigate the relation between the blood flow in the ICA and CBFGM, we conducted a linear regression analysis per group, controlling for age and sex.
Results
CBFGM was 42±8 mL/100g/min and 45±5 mL/100g/min for patients and controls, respectively. We observed a trend towards significance of lower CBFGM in cSVD patients, compared to controls (p-value: 0.07). Furthermore, blood flow in the ICA was 3.0±0.6 mL/s for patients and 3.1±0.6 mL/s for controls, the groups did not differ significantly (p-value: 0.49). ICA blood flow was positively correlated to the CBFGM in the cSVD patient group (β=0.51, p-value = <0.001), whereas this relation was not found in the control group (β=-0.12, p-value = 0.66) (Figure 3).Discussion & conclusion
Our study revealed a positive correlation between the blood flow in the supplying ICAs and gray matter perfusion in cSVD patients with VCI, which was not found in the control group. This result suggests a reduced ability to autoregulate the CBF and compensate for blood supply changes in cSVD patients, possibly because of impaired autoregulation by the NVU3. The reduction in autoregulatory capacity could be due to various pathophysiological effects including microvascular rarefaction6, 11. Alternatively, decreased ASL-derived brain perfusion may be measured due to remaining effects of a constant (instead of a multi) post labeling delay or label duration over a range of patients with variable ICA flow, which needs to sorted out.Acknowledgements
This work has received funding from the European Union’s Horizon 2020 research and innovation programme ‘CRUCIAL’ under grant number 848109.
This work received funding from MODEM, a Dutch national consortium part of the Dementia Research Program of ZonMw (grant #10510032120006) supported by the National Dementia Strategy 2021-2030 of the Dutch Ministry of Health, Welfare and Sport.
This work received funding from Alzheimer Nederland (#WE.30-2022-04) supporting MODEM research.
We thank M. van Osch for initial help on the ASL setup.
References
1. Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. The Lancet Neurology. 2013;12(8):822-38.
2. Chojdak-Łukasiewicz J, Dziadkowiak E, Zimny A, Paradowski B. Cerebral small vessel disease: A review. Adv Clin Exp Med. 2021;30(3):349-56.
3. Yang Q, Wei X, Deng B, Chang Z, Jin D, Huang Y, et al. Cerebral small vessel disease alters neurovascular unit regulation of microcirculation integrity involved in vascular cognitive impairment. Neurobiol Dis. 2022;170:105750.
4. Caruso P, Signori R, Moretti R. Small vessel disease to subcortical dementia: a dynamic model, which interfaces aging, cholinergic dysregulation and the neurovascular unit. Vascular Health and Risk Management. 2019;15(null):259-81.
5. Alsop DC, Detre JA, Golay X, Günther M, Hendrikse J, Hernandez-Garcia L, et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med. 2015;73(1):102-16.
6. van Dinther M, Voorter PH, Jansen JF, Jones EA, van Oostenbrugge RJ, Staals J, Backes WH. Assessment of microvascular rarefaction in human brain disorders using physiological magnetic resonance imaging. J Cereb Blood Flow Metab. 2022;42(5):718-37.
7. Fischl B, Dale AM. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc Natl Acad Sci U S A. 2000;97(20):11050-5.
8. Chappell MA, Groves AR, MacIntosh BJ, Donahue MJ, Jezzard P, Woolrich MW. Partial volume correction of multiple inversion time arterial spin labeling MRI data. Magn Reson Med. 2011;65(4):1173-83.
9. Chappell MA, Groves AR, Whitcher B, Woolrich MW. Variational Bayesian inference for a nonlinear forward model. Trans Sig Proc. 2009;57(1):223–36.
10. Khan MA, Liu J, Tarumi T, Lawley JS, Liu P, Zhu DC, et al. Measurement of cerebral blood flow using phase contrast magnetic resonance imaging and duplex ultrasonography. J Cereb Blood Flow Metab. 2017;37(2):541-9.
11. Voorter PHM, van Dinther M, Drenthen GS, Elschot EP, Staals J, van Oostenbrugge RJ, et al. Cerebral vessel size imaging reveals altered microvascular architecture in patients with vascular cognitive impairment. ISMRM; 2023; Toronto.
Figures
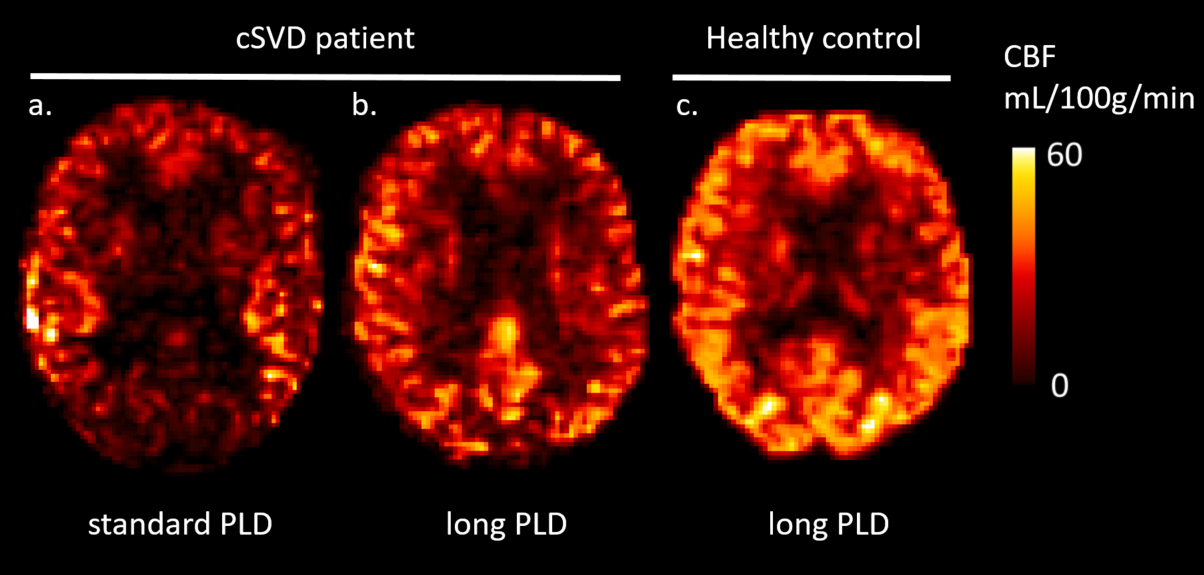
Figure 1. a. A cerebral blood flow (CBF) map measured with arterial spin labeling (ASL), using the standard post labeling delay (PLD) (labeling duration LD: 1800ms, PLD: 2000ms) b. The CBF map measured with ASL, using a longer PLD (LD: 3000ms , PLD: 2500ms) for the same patient with cerebral small vessel disease (female, 82 years). The rightmost CBF map is measured with ASL using the longer PLD for a healthy control (female, 79 years)
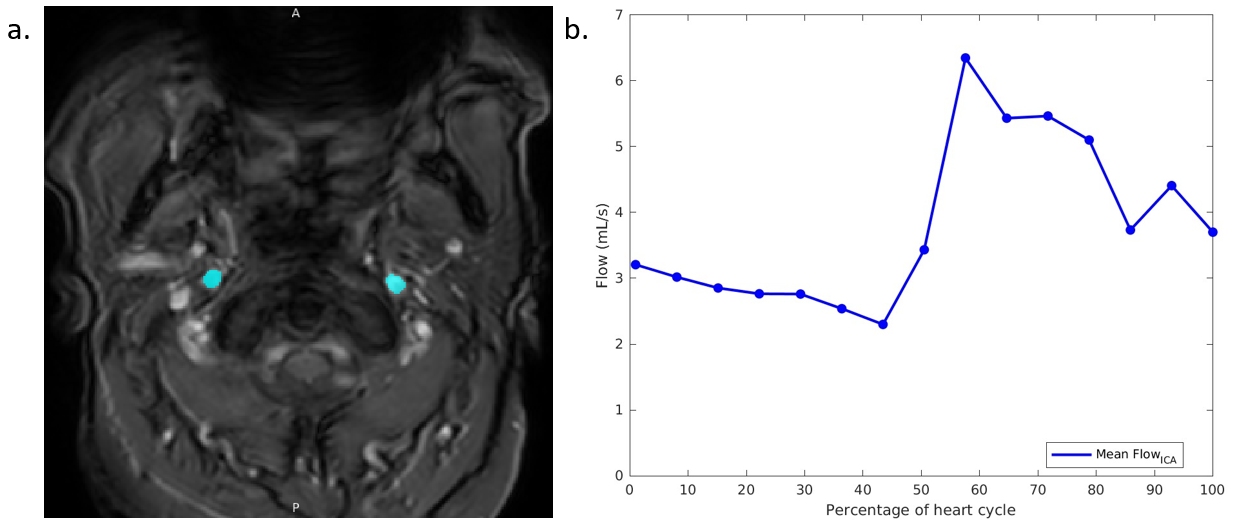
Figure 2: a: An example of a phase-contrast MRI (PCMRI) magnitude image with internal carotid artery (ICA) segmentation (blue). b: ICA blood flow over the heart cycle, measured by phase-contrast MRI. Both images for a patient with cerebral small vessel disease (male, 79 years)
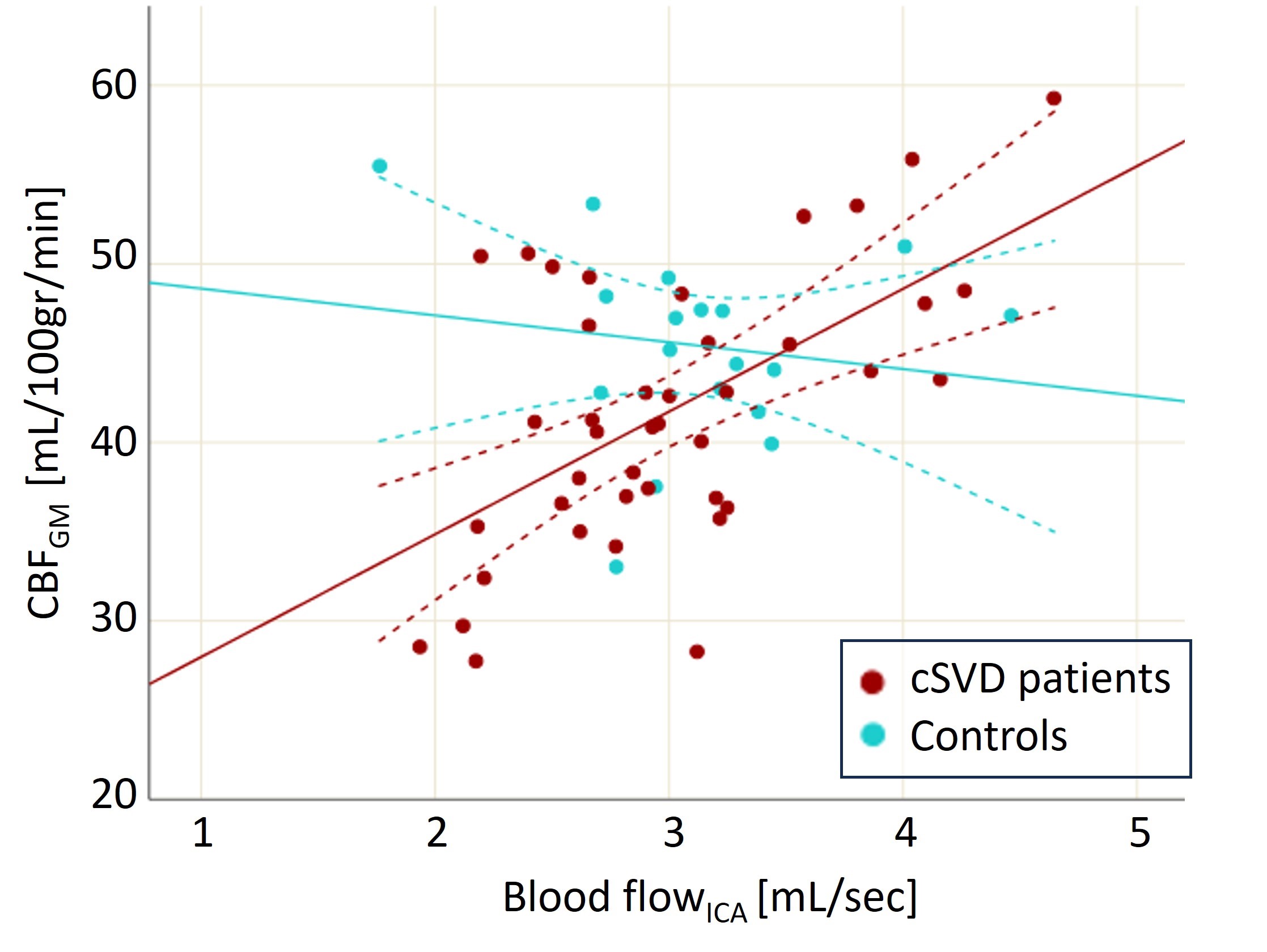
Figure 3: Relation between internal carotid artery (ICA) blood flow, measured by phase-contrast MRI, and the cerebral blood flow in the gray matter (CBFGM), measured by arterial spin labeling. The dotted lines give confidence intervals of the population means. The relation between blood flowICA and CBFGM in the cerebral small vessel disease (cSVD) patient group (β=0.51, p-value = <0.001) suggests impaired cerebral autoregulation, which was not found in the control group (β=-0.12, p-value = 0.66).
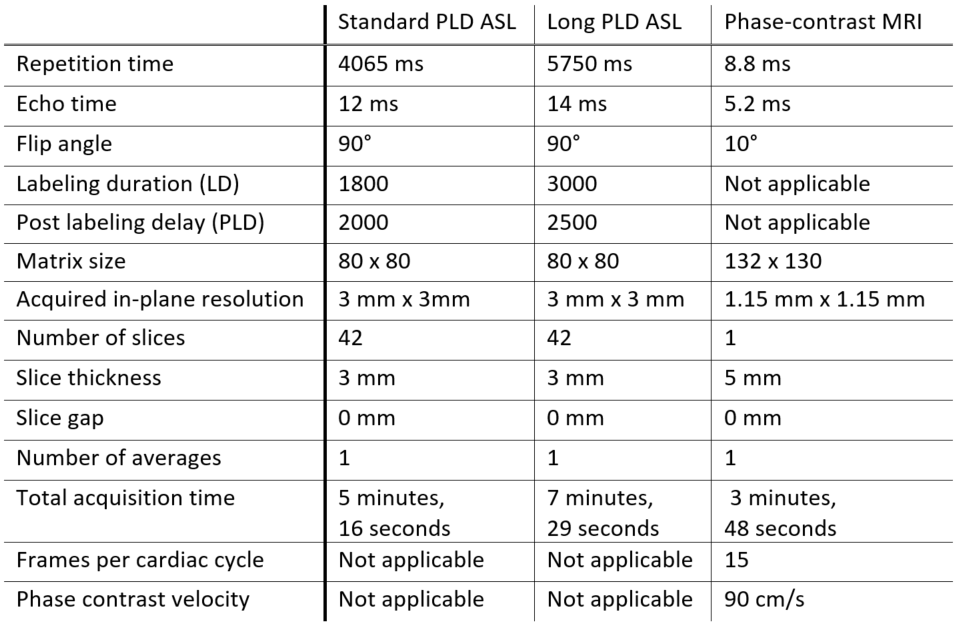
Table 1: Scan parameters for the arterial spin labeling (ASL) scans with both standard and long PLDs and the phase-contrast MRI scan.