2163
Probabilistic Tractography of Key Language Tracts: MNI-based Spherical ROIs Improve Sensitivity and Specificity1King's College Hospital NHS Foundation Trust, London, United Kingdom, 2King's College London, London, United Kingdom, 3Department of Neuroradiology, King's College Hospital, London, United Kingdom, London, United Kingdom
Synopsis
Keywords: Tractography, Tractography & Fibre Modelling
Motivation: Pre-surgical tractography aids neurosurgical planning around key language tracts. Standard reconstruction approaches lead to a trade-off between sensitivity and specificity, and may not characterise all aspects of the target tract.
Goal(s): Increase sensitivity and specificity of reconstruction methods for the inferior fronto-occipital fasciculus and arcuate fasciculus and language tracts.
Approach: A new set of three spherical seed, end, and supplementary waypoint regions of interest (ROIs), defined in MNI space, were implemented using volunteer datasets, and results compared to a reference atlas.
Results: The new 3-ROI approach achieved greater overlap with the reference tracts (higher Dice coefficient), with increased sensitivity and/or specificity.
Impact: Improvements in sensitivity and specificity of reconstructed language tracts using 3-ROI based tractography optimise the characterisation of tracts in healthy volunteers. Further evaluation should now be done to allow extension to clinical cases.
Introduction
Pre-surgical tractography of the brain’s white matter structures aids neurosurgical planning around key functional tracts. Functional mapping of language pathways, including the inferior fronto-occipital fasciculus (IFOF) and arcuate fasciculus (AF), is particularly useful as these tracts are highly patient-specific and may re-organise in response to injury or pathology. Options for standardised clinical approaches to reconstructing the IFOF and AF are available in the literature1,2,3; however, in our experience they often lead to a trade-off between sensitivity and specificity of the reconstruction2. In this work, we propose a set of spherical seed, end, and supplementary waypoint regions of interest (ROIs) defined in MNI space to maximise sensitivity and specificity of language tracts.Methods
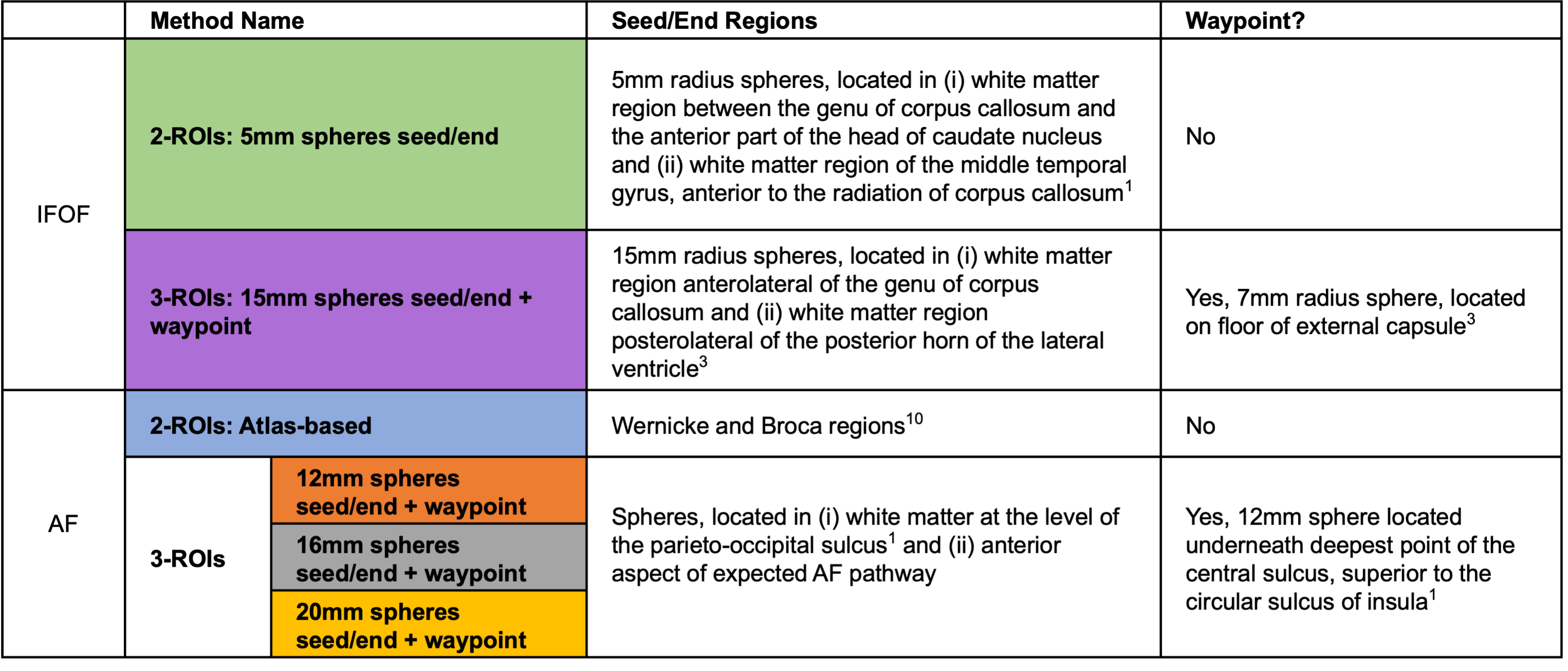
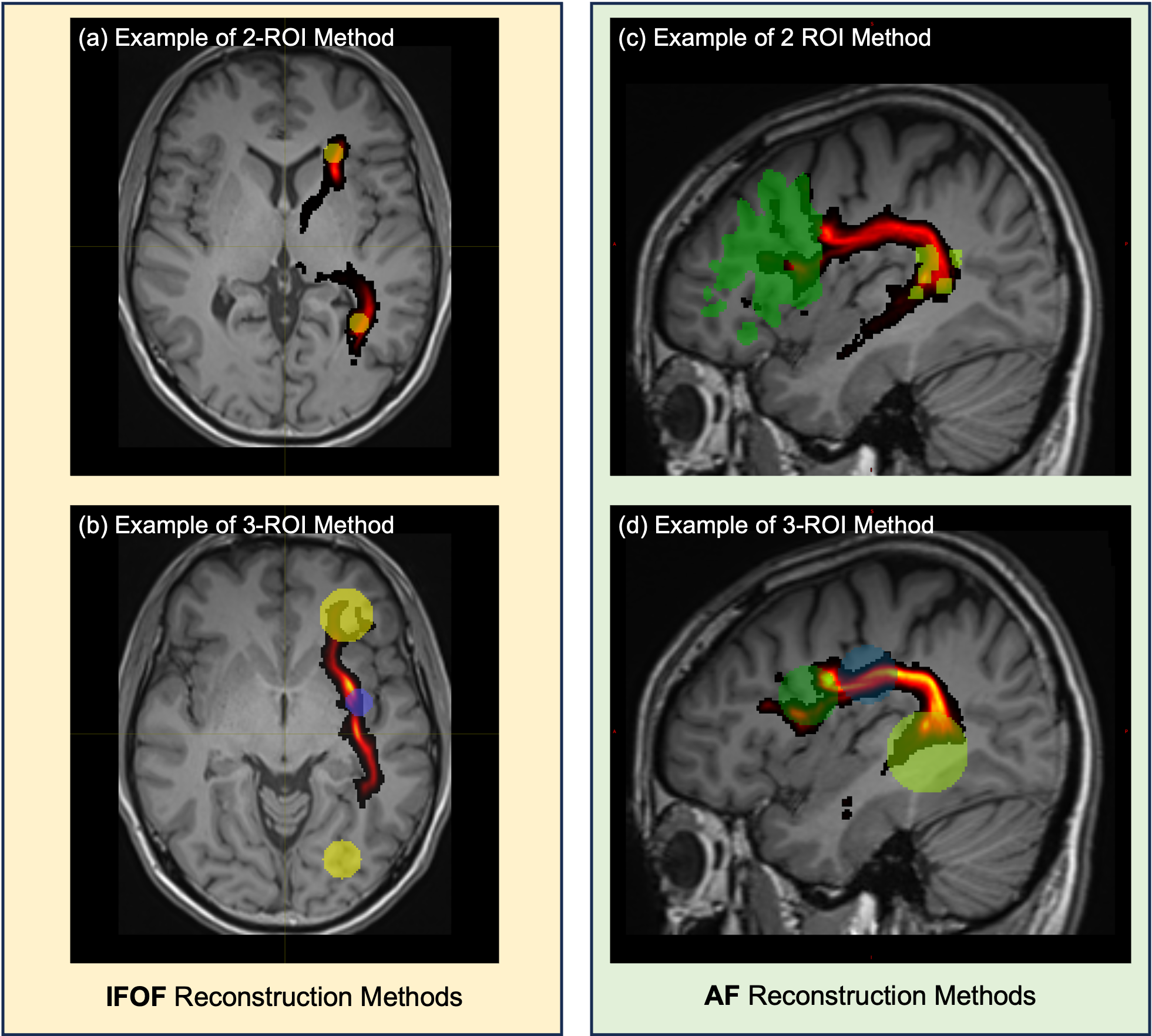
Datasets from 15 healthy right-handed volunteers were acquired at 3T (Siemens Magnetom Vida, Erlangen, Germany) with SE-EPI sequence (TE/TR = 86/6500ms, voxel size = 2x2x2mm3, 6 baseline images (b=0 s/mm2) and 64 diffusion directions (b = 1500s/mm2)). Constrained spherical deconvolution4 tractography was performed separately for the IFOF and AF on all 15 datasets, using MRTrix35 and the probabilistic iFOD2 tractography algorithm6.For both tracts, 3-ROI approaches were implemented alongside the 2-ROI approaches proposed in the literature, which adopt either manually defined small spheres (IFOF) or atlas-defined regions (AF) - see Table 1 for details. The 3-ROI approaches employed two larger spheres as seed and end regions and a waypoint sphere to confine the core of the tract. The spheres were defined in MNI space, following literature guidance1 and the predicted path of the tract3.
For each approach, tractography was performed on the dominant hemisphere (left) and run from seed to end region and vice-versa. These two tract images were then combined, preserving only voxels present in both images. Quantitative evaluation was performed following registration of all tracts into MNI space using SPM127. Tracts were compared to a reference probabilistic IFOF and AF atlases8 using FSL9 and MATLAB to calculate sensitivity, specificity, and Dice coefficient measures:
$$ Sensitivity= \frac{True.Positives}{(True.Positives+False.Negatives}\times100$$
$$ Specificity= \frac{True.Negatives}{(True.Negatives+False.Positives}\times100$$
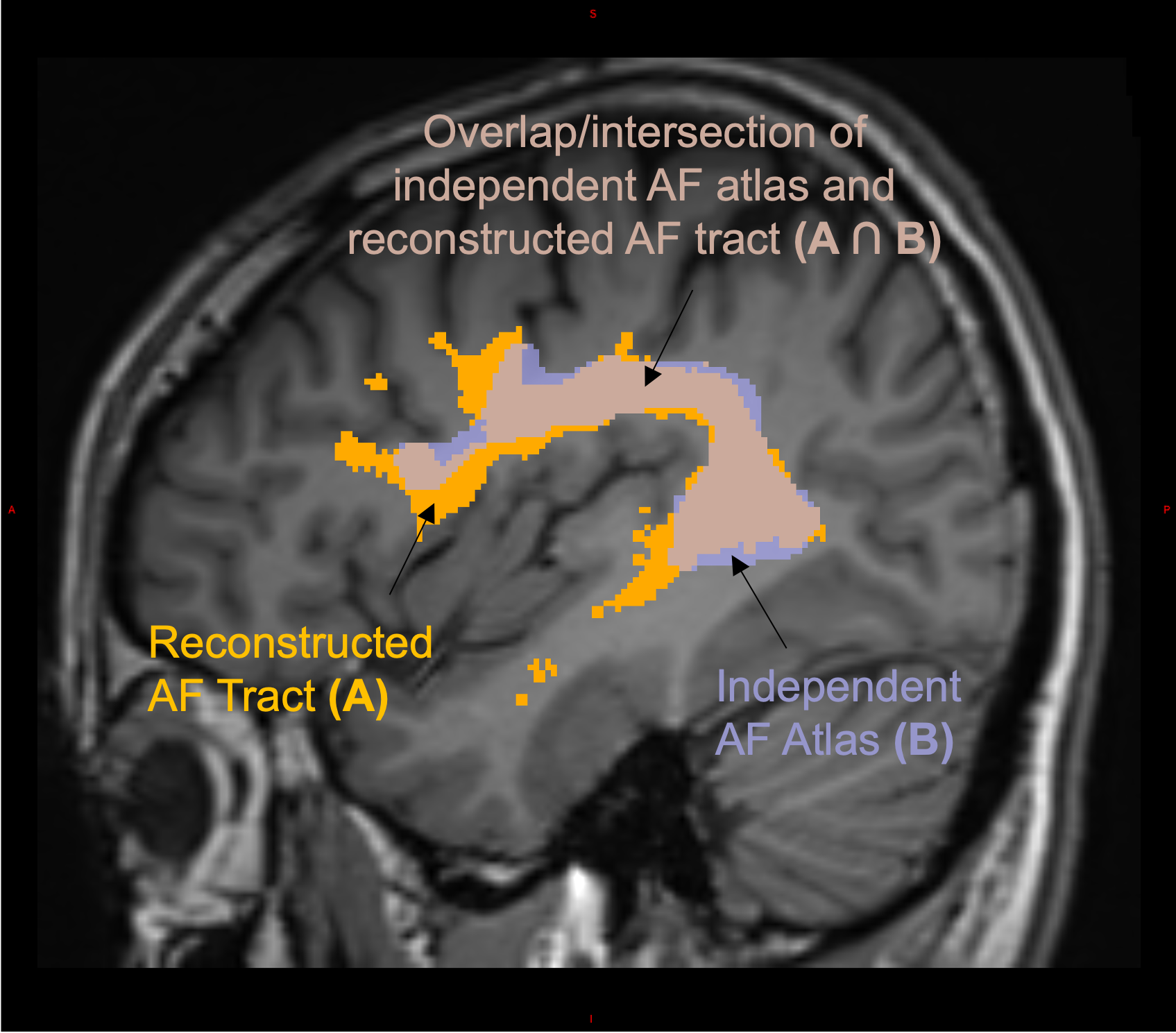
$$ Dice.Similarity.Coefficient = \frac{2\times (A\cap B)}{A+B}$$
where A = independent atlas tract image and B = tractography tract image (see Figure 1).
For evaluation, tracts were thresholded at 2 streamlines/voxel and the reference atlas at 0.15 probability density to preserve all aspects of the tracts (Figure 1).
Results
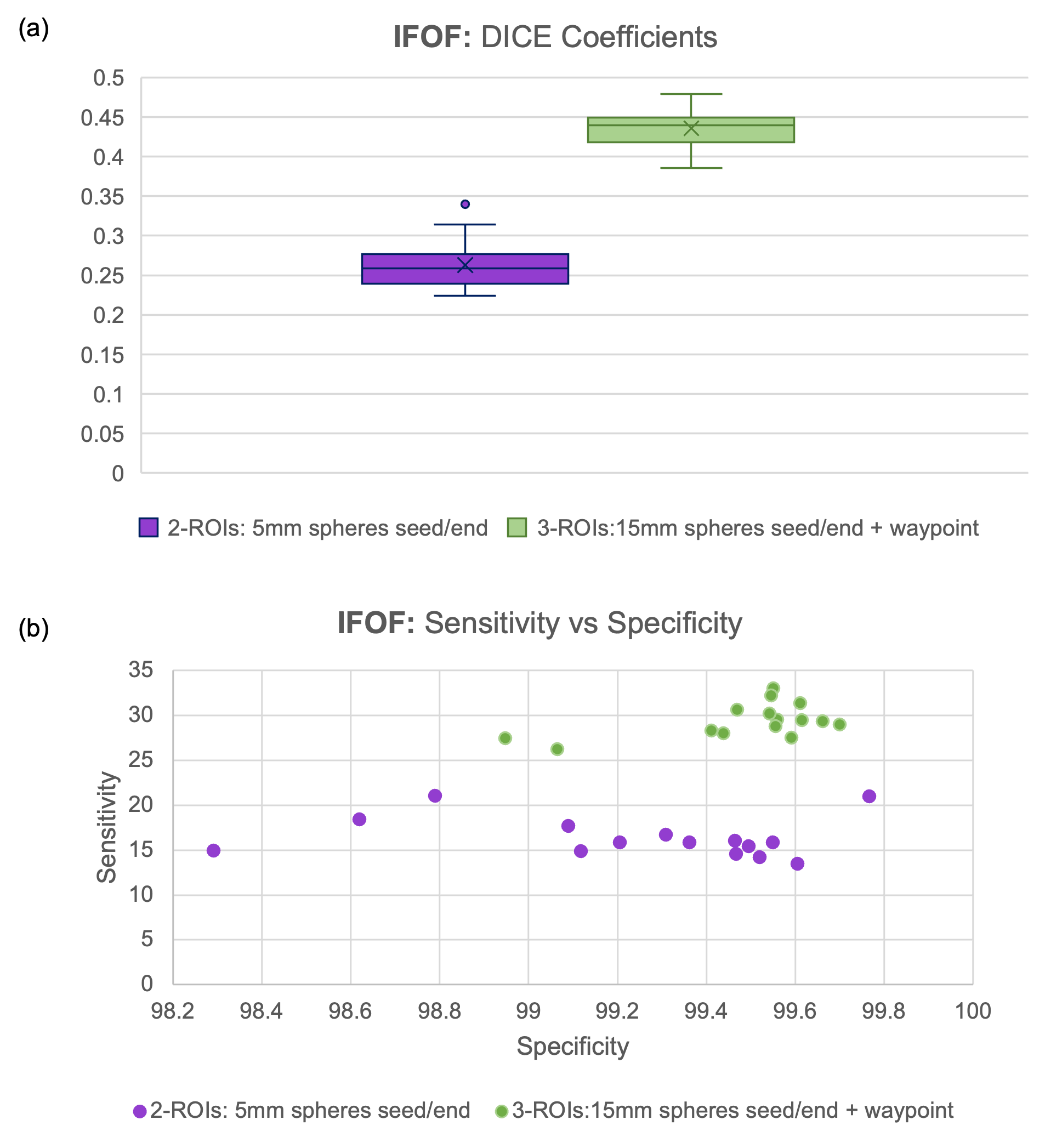
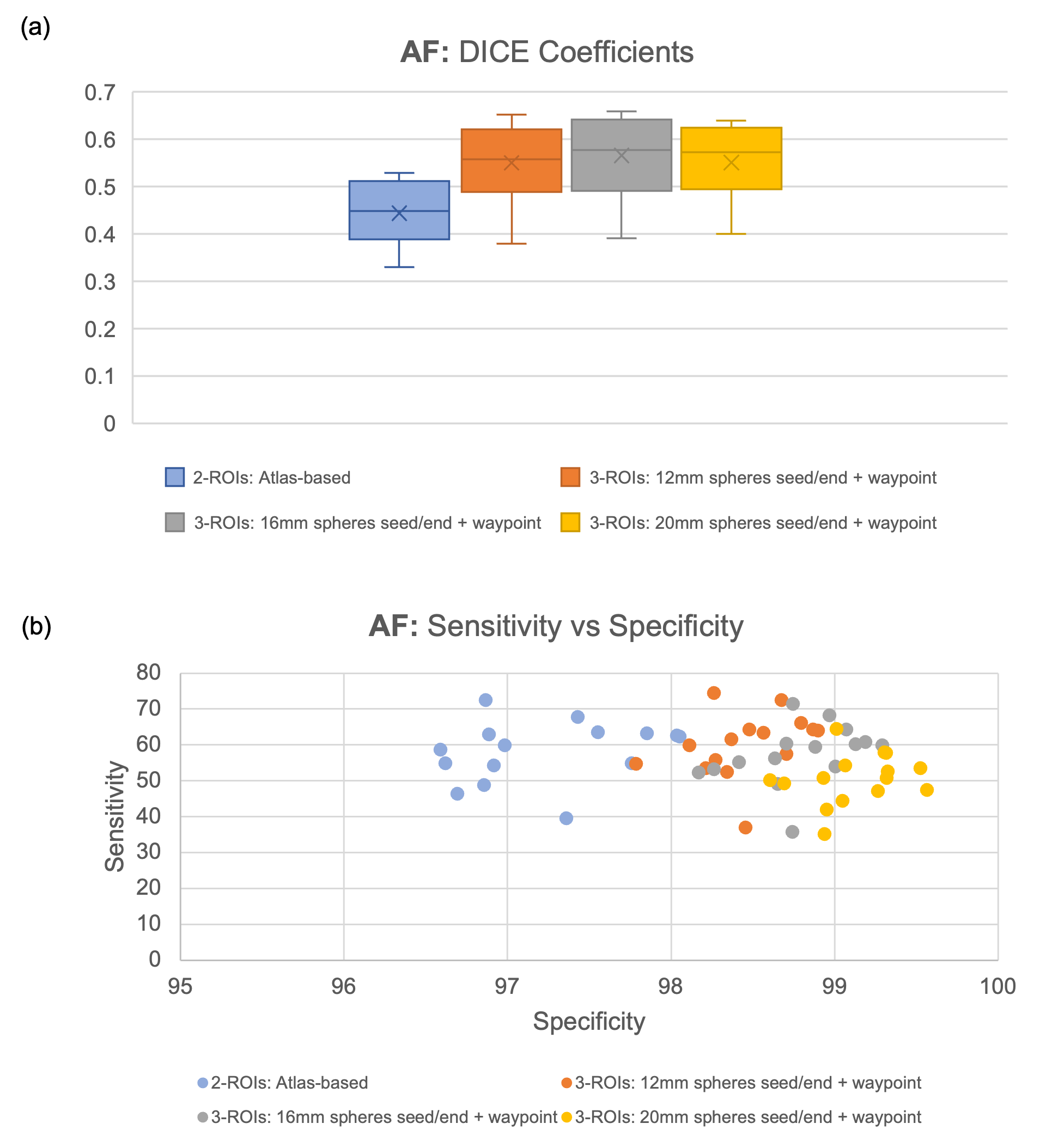
For the IFOF, the 3-ROI method had a higher Dice coefficient compared to the 2-ROI method (mean 0.44 vs 0.25), and increased sensitivity and specificity (Figure 2).For the AF, all 3-ROI methods showed higher Dice coefficients (mean 0.55-0.58 vs 0.45) and increased specificity, while maintaining sensitivity, compared to the 2-ROI method (Figure 3). For this tract, the sizes of the seed and end spheres were also investigated. The mean specificity level increased with sphere size and, in general, the sphere size did impact the overlap with the reference atlas (as measured by the Dice coefficient) with 16mm seed/end spheres optimal.
Discussion
In this work, 3-ROI approaches to IFOF and AF tractography achieved greater overlap with the reference tracts, as compared to 2-ROI approaches, as well as increased sensitivity and/or specificity.For the IFOF, the 2-ROI approach including two relatively small spheres as seed/end regions led to a lack of sensitivity and a partial characterisation of the tract. The 3-ROI approach, by increasing the size of the seed/end spheres and adding a waypoint, increased the sensitivity without decreasing the specificity of the tract (Figure 3).
For the AF, the use of large atlas ROIs led to a loss of specificity with large sprawl at the tract ends. The use of 3-ROI sets of appropriately sized spheres increased specificity by focussing the tractography, with no loss of sensitivity in the core (Figure 4).
For both tracts, the use of standardised spheres placed using anatomical landmarks in MNI space and registered to patient space ensured a reproducible delineation of tractography regions.
In this work, we compared Dice coefficients and sensitivity/specificity on a relative basis, as the values are influenced by the choice of reference atlas and thresholds for the tract and can therefore not be interpreted as absolute measures. Future evaluation will compare population probability distributions directly, as well as consider both hemispheres and extension to clinical data.
Conclusion
Our results suggest that current standard 2-ROI methods can be further optimised. New 3-ROI methods showed a relative increase in overlap with an independent reference atlas, and greater sensitivity without reducing specificity (IFOF) or specificity without reducing sensitivity (AF). The optimised methods maintain a standardised approach using MNI-space defined spheres. Further work is required to assess the proposed approaches in patient cases.Acknowledgements
No acknowledgement found.References
1 Fekonja, L., Wang, Z., Bährend, I. et al. Manual for clinical language tractography. Acta Neurochir 161, 1125–1137 (2019) https://doi.org/10.1007/s00701-019-03899-0
2 Ansell J et al., Probabilistic Tractography of the Arcuate Fasciculus: Sensitivity and Specificity of Standardised fMRI and Atlas-based Approaches (Abstract 4290), Proc. Intl. Soc. Mag. Reson. Med. 29 (2021), https://cds.ismrm.org/protected/21MProceedings/PDFfiles/4290.html
3 Hadijgeorgiou V et al,, Standardisation of multi-fiber probabilistic tractography of the inferior fronto-occipital fasciculus, Proceedings of BIC-ISMRM Annual Meeting, 2021
4 Tournier J-D, Calamante F, Connelly A. Robust determination of the fibre orientation distribution in diffusion MRI: Non-negativity constrained super-resolved spherical deconvolution. NeuroImage 35.4 (May 2007).
5 MRTrix3 http://mrtrix.org
6 Tournier J-D, Calamante F, Connelly A. Improved probabilistic streamlines tractography by 2nd order integration over fibre orientation distributions. Proceedings of the International Society for Magnetic Resonance in Medicine 2010
7 SPM12 (Wellcome Trust Centre for Neuroimaging, UCL, UK [Ashburner et al., 2012])
8 Mega Track Atlas https://megatrackatlas.org
9 M. Jenkinson, C.F. Beckmann, T.E. Behrens, M.W. Woolrich, S.M. Smith. FSL. NeuroImage, 62:782-90, 2012
10 Julich Histological Atlas and Harvard-Oxford Cortical Structural Atlas
Figures