2161
Intraoperative fiber tractography during pediatric posterior fossa tumor surgery - initial experience.1Prinses Máxima Centrum, Utrecht, Netherlands, 2University Medical Centre Utrecht, Utrecht, Netherlands
Synopsis
Keywords: Tractography, Surgery
Motivation: Intraoperative fiber tractography could help to elucidate the nature of cerebellar mutism syndrome after tumor resection in pediatric posterior fossa tumor (pPFT) patients.
Goal(s): To explore the feasibility of reconstructing eloquent fiber tracts with a short intraoperative diffusion MRI scan in pPFT patients.
Approach: We reconstructed tracts intraoperatively in four pPFT patients and compared their structural properties to preoperative scans obtained with the same settings.
Results: It is in general possible, but challenging, to reconstruct the eloquent tracts in pre- and intraoperative data of pPFT patients. However, further optimization of the fiber tractography model is required to increase their quality.
Impact: The impact of the mechanical manipulation of the surgical procedure on the eloquent pathways in pediatric posterior fossa tumor patients is investigated through the development of a reliable fiber tractography model for intraoperative diffusion MRI.
Introduction
Intraoperative fiber tractography can help the neurosurgeon to identify eloquent tissue and prevent neurological damage. In pediatric posterior fossa tumor (pPFT) patients, cerebellar mutism syndrome (CMS) could be associated with damage to eloquent dentate-rubro-thalamic tracts (DRTTs)1. Intraoperative DRTT reconstruction could provide new information about the integrity of the DRTT after tumor debulking and re-expansion of the cerebellum. This might aid neurosurgeons in understanding how to avoid affecting CMS-related connectivity2. To investigate intraoperative DRTT fiber integrity, we first need to evaluate whether the DRTT can be identified with the limited amount of diffusion MRI (dMRI) data available intraoperatively due to time constraints, brain shift, and fewer RF coils. Here, we present our initial experience of intraoperative fiber tractography in pPFT patients.Methods
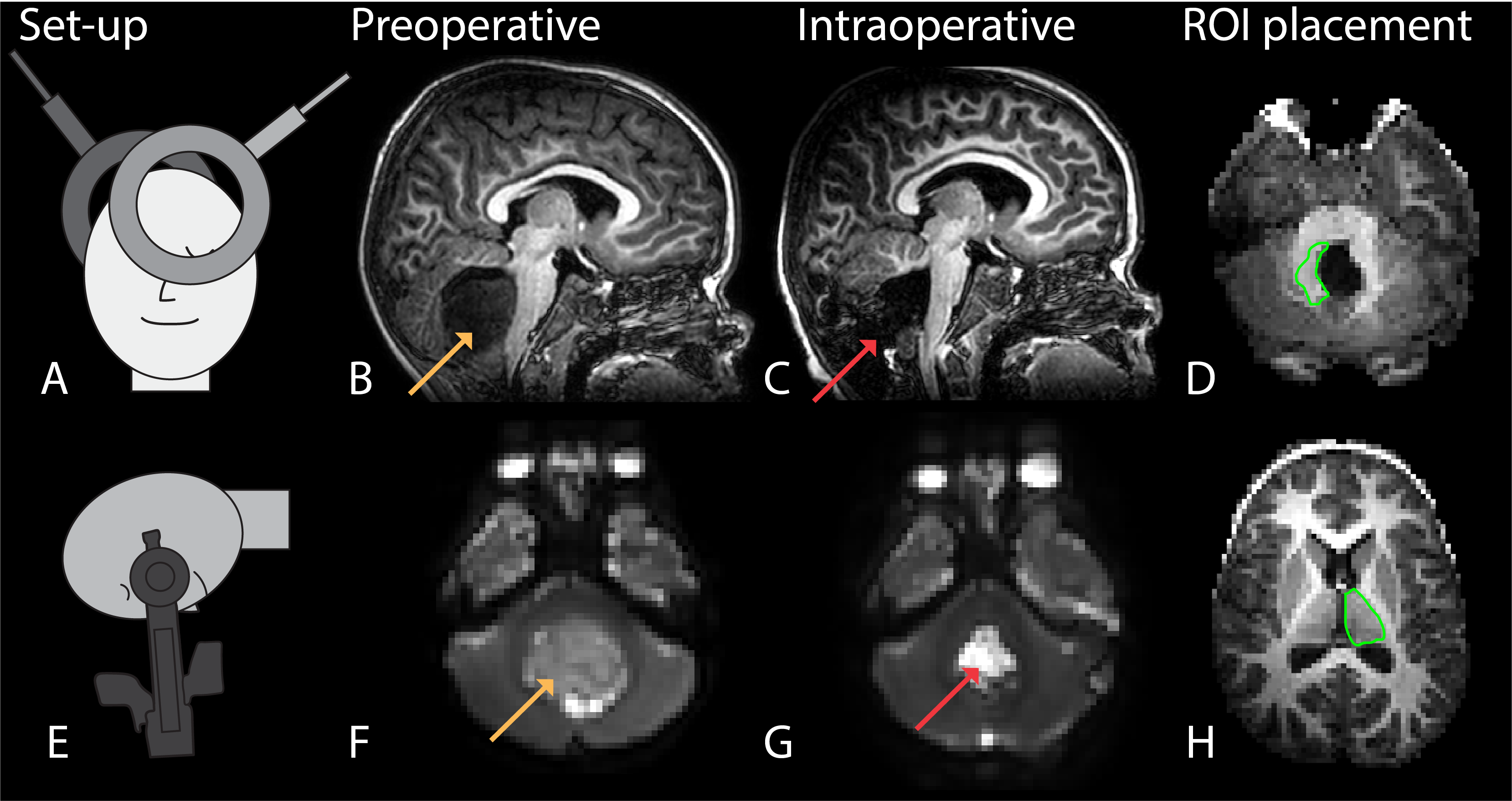
Experimental set-upThis study was approved by the local ethical review board. Four pPFT patients (age 21months-4years) that underwent surgery were included in this study. We obtained all MR-images with a 3T Philips Ingenia ElitionX with two RF coils (Fig.1A). Both pre- and intraoperative images were acquired on the day of surgery under the same anesthetics with the patient in the prone position and the head secured in the DORO head-clamp (Fig.1E). The intraoperative scan is acquired with an open skull, and most of the tumor resected (Fig.1C).
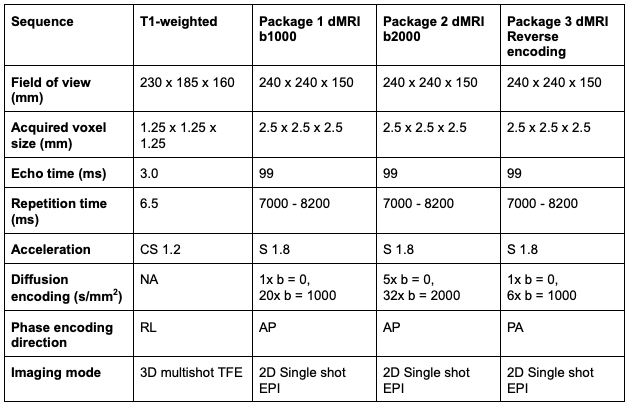
Imaging parameters can be found in table 1.
Image post-processing
Data of a 5-minutes multi-shell dMRI scan (Fig.1F,G) was used to reconstruct the DRTT and a control tract outside the resection area (i.e., thalamo-frontal tract, TF). Preprocessing was done with the fully automated MRIToolkit pipeline3 and ExploreDTI4,5. Preprocessing steps were similar to Goghari et al.6. We corrected for EPI distortions by means of the reverse phase encoding direction data7. After preprocessing, the DKI model was fit to the data using the MK-curve correction method8,9. The Generalized Richardson Lucy spherical deconvolution method4 was applied to reconstruct fiber orientation distributions in white matter while accounting for partial volume with gray matter and cerebrospinal fluid, consequently deterministic fiber tractography was performed. Whole-brain tractography was performed by seeding all voxels within the brain mask, with parameters step-size 1mm. We tried both 45- and 60-degrees angle thresholds. The T1-weighted image was linearly registered to the dMRI data and was then used to draw the inclusion ROIs for the DRTT segmentation in ExploreDTI (Fig.1D,H). The TF tracts were segmented from the whole-brain tractography by applying the white matter analysis pipeline10. When a tract could not be found with intraoperative tractography, non-linear image registration was used to transform a mask of preoperative tractography to the intraoperative space. The transformation was computed with Elastix in three steps (rigid, affine, bspline).
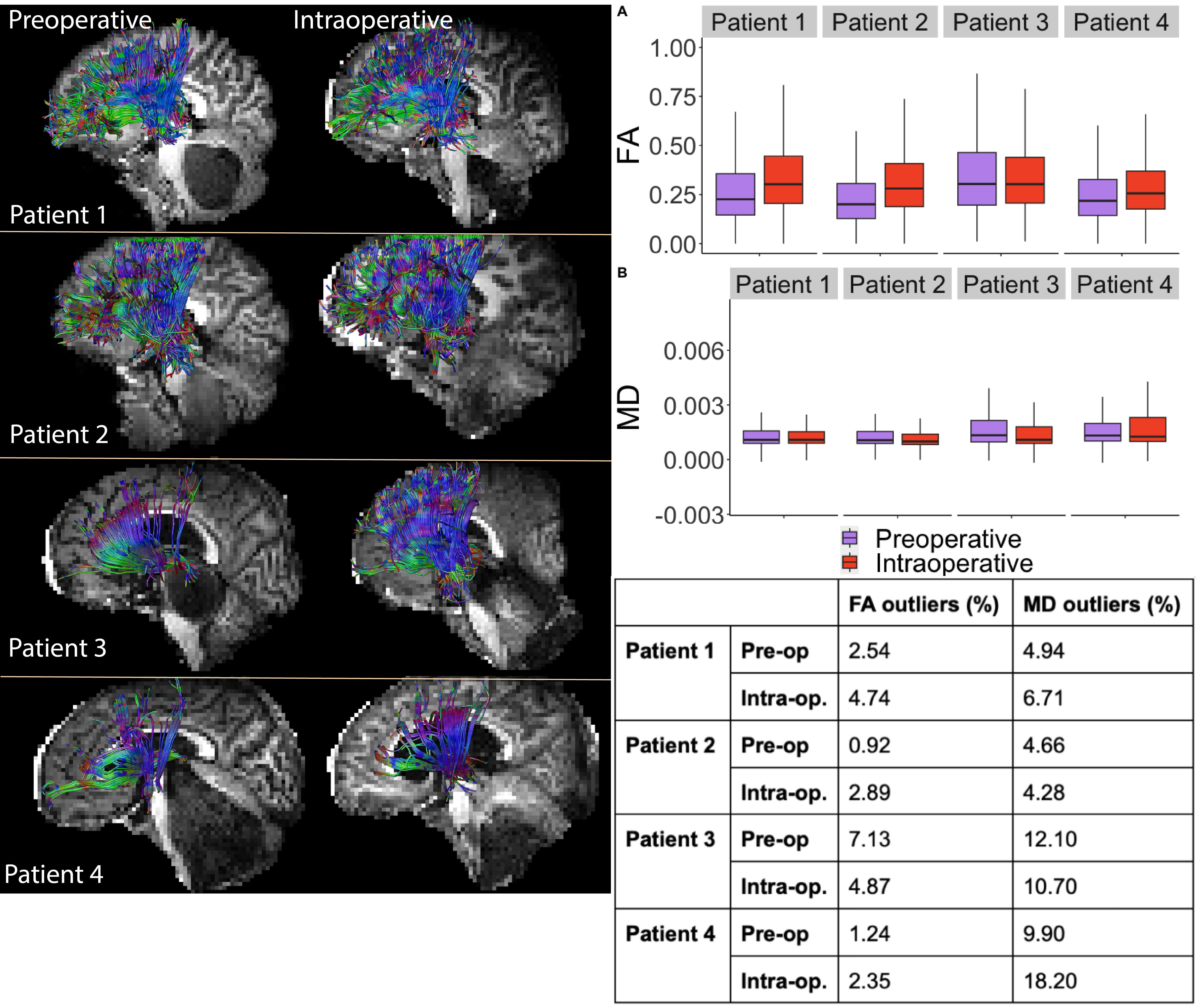
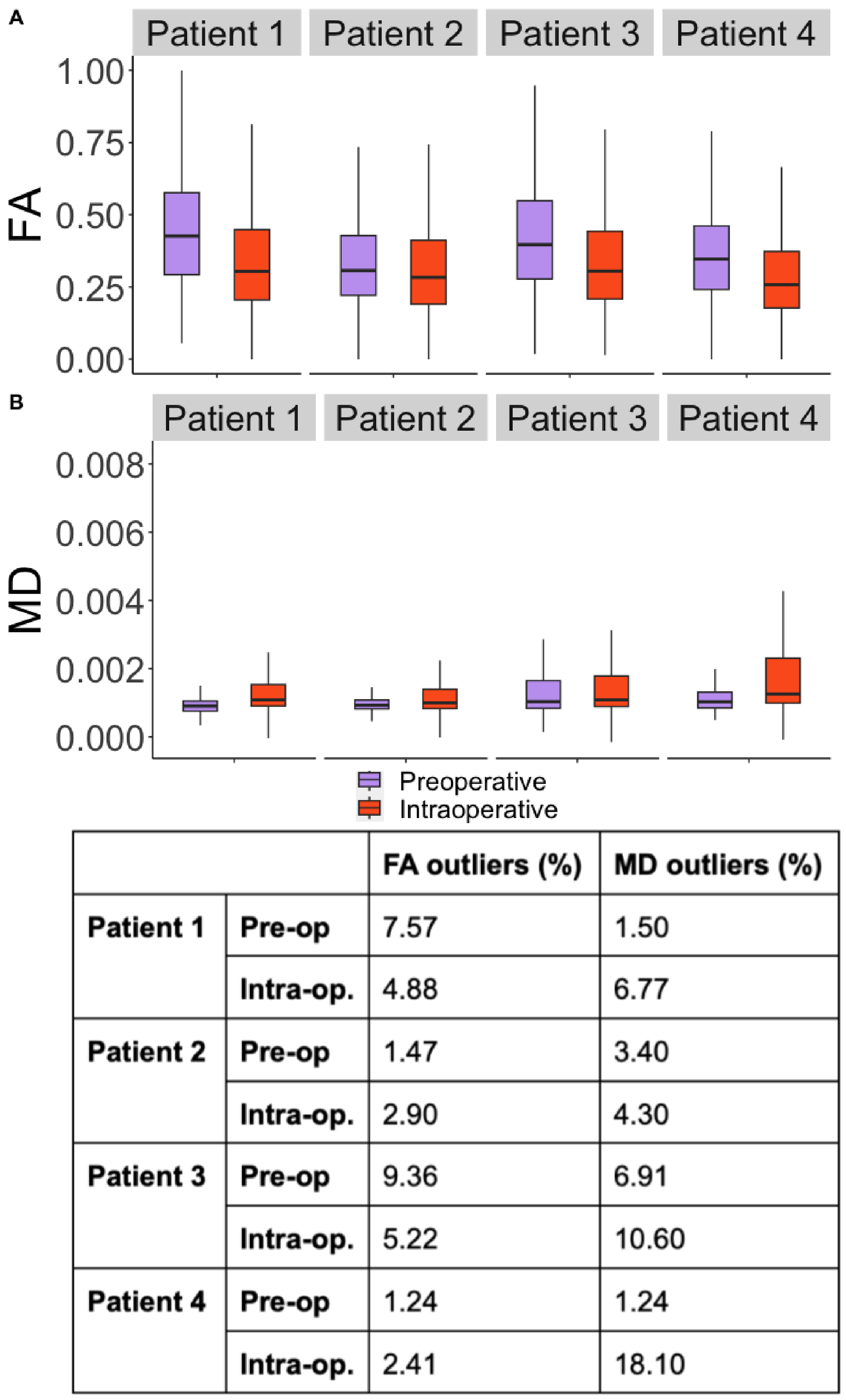
The mean fractional anisotropy (FA) and mean diffusivity (MD) of the tracts were then calculated and compared between preoperative and intraoperative scans.
Results
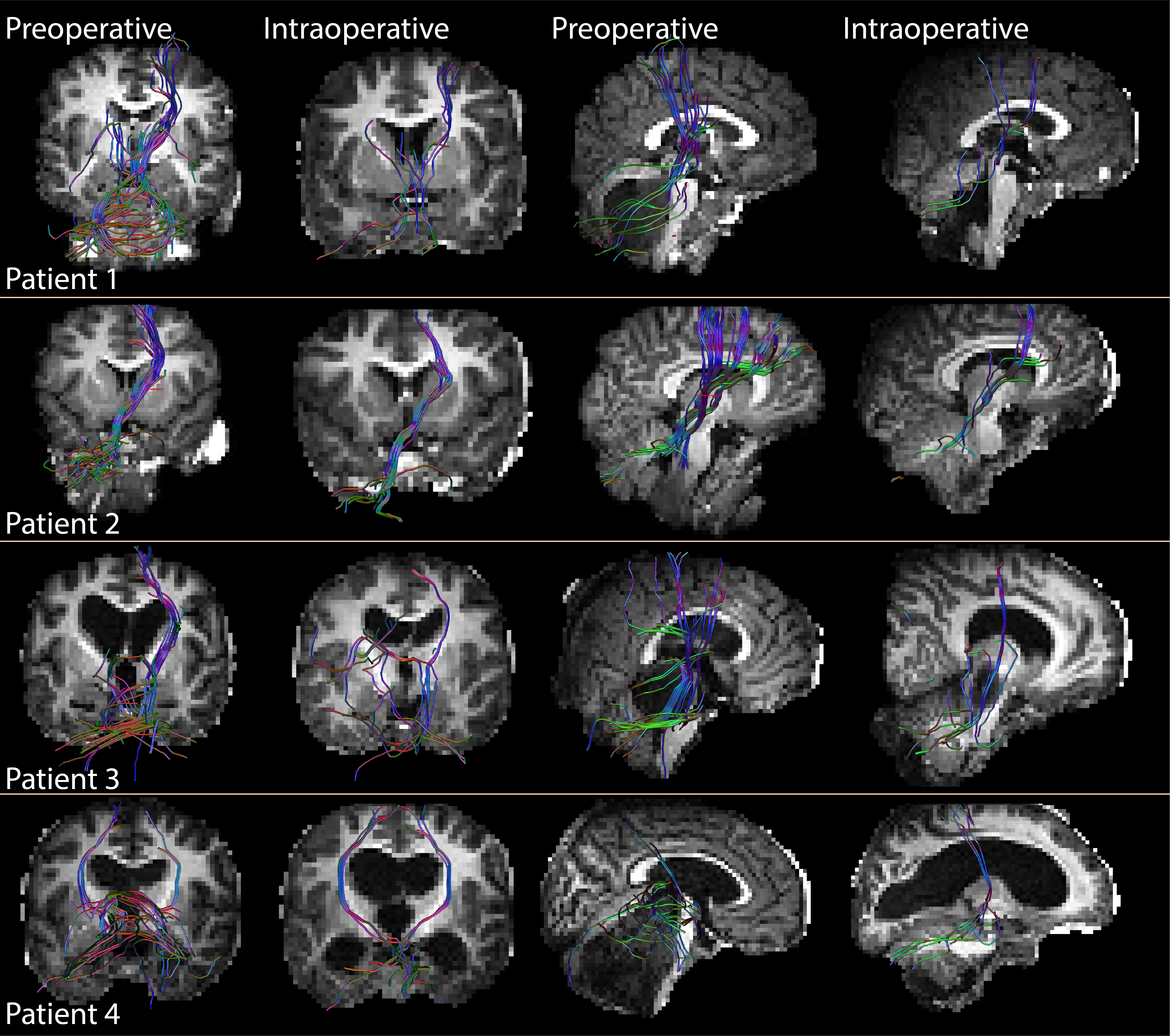
The fiber tractography model with a 45-degrees angle threshold proved sufficient to reconstruct the core of the DRTT in the preoperative data but did not yield results in the intraoperative data. The model with the 60-degrees threshold visually yielded more complete reconstructions of the DRTT segmentations with the preoperative data, but lower quality with the intraoperative data (Fig.2). For that reason, we continued our analysis of the DRTT and TF tract on the 60-degrees model.The DRTT could not be reliably reconstructed with intraoperative tractography, and non-linear registration of the preoperative DRTT masks was used for all patients. TF tracts were not non-linear registered, but reconstructed in the pre- and intraoperative native space (Fig.3). All mean DRTT (Fig.4) and TF (Fig.3) FA values were within the same range, while the MD values showed an increased spread in the intraoperative setting.
Discussion
Despite identical hardware and patient positioning in both scan sessions, differences can be observed in the feasibility of DRTT segmentation. The lower quality of intraoperative DRTT could be explained by a lower SNR in the resection cavity resulting from a B0-field disturbance due to the open skull, leading to EPI distortions. This could result in decreased sensitivity of the fiber tractography model. Furthermore, it could be interesting to optimize other tractography parameters (e.g., step-size and fiber orientation distribution threshold) as well.Before we can interpret differences in FA and MD between the pre- and intraoperative data as surgery-related morphology, we shall need to further examine control tracts and determine reproducibility of the tractography.
Conclusion
Despite limited scan time and number of RF coils in the intraoperative setting, we showed that it is possible to segment the DRTT in pre- and intraoperative data of pPFT patients. However, further optimization is required to increase the quality of the DRTT.Acknowledgements
No acknowledgement found.References
1. Avula S. Radiology of post-operative paediatric cerebellar mutism syndrome. Childs Nerv Syst. 2020;36:1187-1195. doi:10.1007/s00381-019-04224-x
2. Toescu SM, Hales PW, Aquilina K, Clark CA. Quantitative MRI in post-operative paediatric cerebellar mutism syndrome. Eur J Radiol. 2018;108(August):43-51. doi:10.1016/j.ejrad.2018.09.007
3. https://github.com/delucaal/MRIToolkit.git
4 Guo F, Leemans A, Viergever MA, Dell’Acqua F, De Luca A. Generalized Richardson-Lucy (GRL) for analyzing multi-shell diffusion MRI data. Neuroimage. 2020;218:1-16. doi:10.1016/j.neuroimage.2020.116948
5. Leemans A, Jeurissen B, Sijbers J, Jones DK. ExploreDTI: a graphical toolbox for processing, analyzing, and visualizing diffusion MR data. Proc Int Soc Magn Reson Med. 2009;17:3537.
6. Goghari VM, Kusi M, Shakeel MK, et al. Diffusion kurtosis imaging of white matter in bipolar disorder. Psychiatry Res - Neuroimaging. 2021;317(February):111341.
7. Andersson JLR, Skare S, Ashburner J. How to correct susceptibility distortions in spin-echo echo-planar images: Application to diffusion tensor imaging. Neuroimage. 2003;20(2):870-888. doi:10.1016/S1053-8119(03)00336-7
8. Jensen JH, Helpern JA, Ramani A, Lu H, Kaczynski K. Diffusional kurtosis imaging: The quantification of non-Gaussian water diffusion by means of magnetic resonance imaging. Magn Reson Med. 2005;53:1432-1440. doi:10.1002/mrm.20508
9. Zhang F, Ning L, O’Donnell LJ, Pasternak O. MK-Curve - Characterizing the Relation between Mean Kurtosis and Alterations in the Diffusion MRI Signal Fan. Neuroimage. 2019;196:68-80. doi:10.4049/jimmunol.1801473.The
10. Zhang F, Wu Y, Norton I, et al. An anatomically curated fiber clustering white matter atlas for consistent white matter tract parcellation across the lifespan. Neuroimage. 2018;179:429-447. doi:10.1016/j.neuroimage.2018.06.027
Figures