2151
Subject-specific analysis approach to longitudinal tracing of heterogeneous white matter abnormalities in sports-related concussion1Department of Radiology and Imaging Sciences, Indiana University School of Medicine, Indianapolis, IN, United States, 2Department of Neurology, Indiana University School of Medicine, Indianapolis, IN, United States, 3Department of Biostatistics and Health Data Science, Indiana University School of Medicine, Indianapolis, IN, United States, 4Michigan Concussion Center, University of Michigan, Ann Arbor, MI, United States, 5Department of Neurosurgery, Medical College of Wisconsin, Milwaukee, WI, United States, 6Department of Psychiatry, Indiana University School of Medicine, Indianapolis, IN, United States, 7Department of Epidemiology and Biostatistics, School of Public Health, Indiana University, Bloomington, IN, United States, 8Stark Neurosciences Research Initiative, Indiana University School of Medicine, Indianapolis, IN, United States
Synopsis
Keywords: DWI/DTI/DKI, Diffusion Tensor Imaging, Sport-related concussion, Subject-specific analysis
Motivation: Unlike groupwise approaches, subject-specific analysis has the potential to pinpoint highly individualized abnormalities in white matter structure caused by sport-related concussion (SRC).
Goal(s): Develop a subject-specific analysis approach to investigate the heterogeneity and longitudinal changes in white matter microstructures after SRC.
Approach: The DTI metrics were voxel-by-voxel Z-transformed using a normal distributed template created from non-contact sport controls. The extreme Z maps were obtained, and averaged extreme Z-scores were compared across three study time points.
Results: The existence of heterogeneity in the concussed brains can be appreciated in the projected extreme Z maps and their longitudinal trajectories.
Impact: We developed a subject-specific analysis pipeline to demonstrate heterogeneity in sport-related concussion with respect to anatomical locations and recovery trajectories.
Introduction
While sport-related concussion (SRC) is a mild form of traumatic brain injury, it may result in acute as well as long-lasting consequences for the brain1-4. MRI has been used to detect post-SRC neuropathophysiologicalprogression noninvasively. Diffusion tensor imaging (DTI), one of the MRI techniques for detecting white-matter microarchitectures, has demonstrated the ability to identify acute changes of the brain post-SRC5,6 as well as persistent white matter alterations up to six months post-injury7. These microstructural changes have shown associations with clinical symptoms8, recovery times1, and blood biomarkers9.Nevertheless, these groupwise analyses require concurrent pathophysiological changes of the brain at the same anatomical locations to reach statistical significance and fail to account for cross-subject heterogeneity. SRC injury arises from unique biomechanical forces, with a highly-individualized potential impact10. Therefore, the heterogeneity in SRC white matter injury is best characterized by a subject-specific analysis that accounts for inter-subject variation11-13. In this work, we developed a subject-specific analysis approach to investigate longitudinal alterations in white matter after SRC.
Method
Study cohortsThe participants were recruited in a multisite study of the natural history of concussion conducted through the Concussion Assessment, Research and Education (CARE) Consortium14. Our analysis included 122 concussed and 143 non-contact sport control collegiate athletes and their neuroimaging data at three time points: (1) 24-48 hours post-injury (acute), (2) time when the concussed athletes became asymptomatic (Asymp), and (3) 7 days after unrestricted return to play (RTP)15.
MRI acquisition
The participants from the four imaging sites underwent MRI on 3T scanners (Siemens Tim Trio, Prisma, or GE 750). A 3D MPRAGE sequence was used for T1W images with TR/TE/TI=2300/2.98/900ms, flip angle=9°, whole brain coverage with a 1mm cubic voxel. A single-shot spin-echo EPI sequence with a twice-refocused spin echo was used for diffusion imaging with TE/TR=98/7900ms and a 2.7mm cubic voxel covering the whole brain. The 30 diffusion-weighted directions at b-value of 1000s/mm2 were used for DTI computation, while a reversed phase-encoding b0 was used for geometric distortion correction.
Image processing
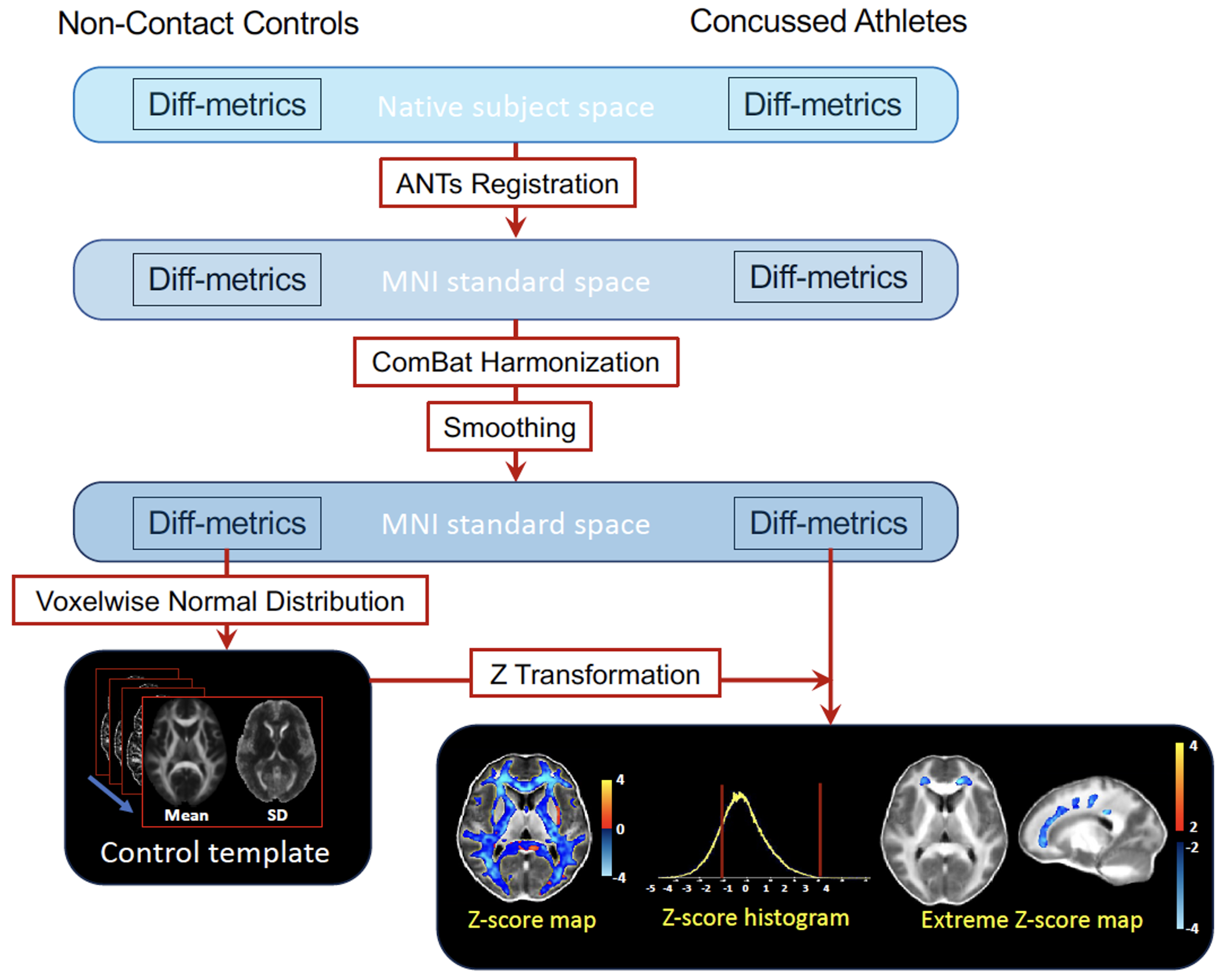
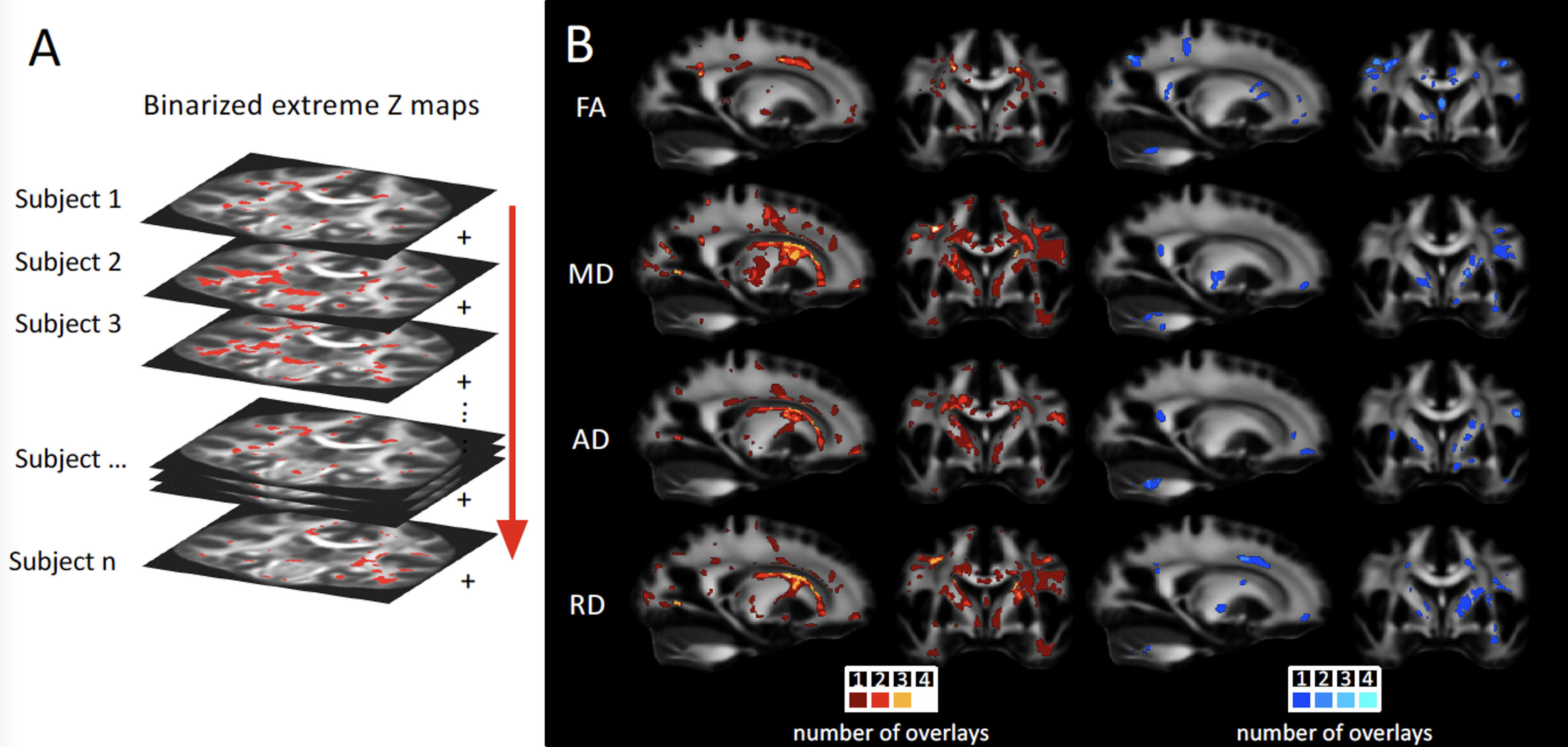
The preprocessing steps were detailed previously9. Briefly, the diffusion-weighted images were first denoised with the local principal component analysis approach16 and were motion, eddy current, and geometric distortion corrected using FSL’s eddy_openmp17. The DTI metrics (FA, MD, AD, and RD) were computed with a linear fitting algorithm (FSL dtifit). As shown in Figure 1, DTI metrics images were registered to the standard space using ANTs nonlinear registration18 and smoothed with a Gaussian kernel at 4 mm full-width half maximum. To voxel-by-voxel harmonize the DTI-metrics, a batch-effect correction tool, ComBat, was used19. The harmonized DTI metrics for the concussed participants were first Z transformed using the normal distribution template created from the non-contact sport control group. The subject-specific extreme z maps were obtained by thresholding at the level of and cluster size >50 voxels. To assess the longitudinal changes of the concussed brains, we averaged the Z-scores of the extreme voxels at the acute time point and the Z-scores of the same voxels at the following time points for each DTI metric of each concussed athlete.
Results
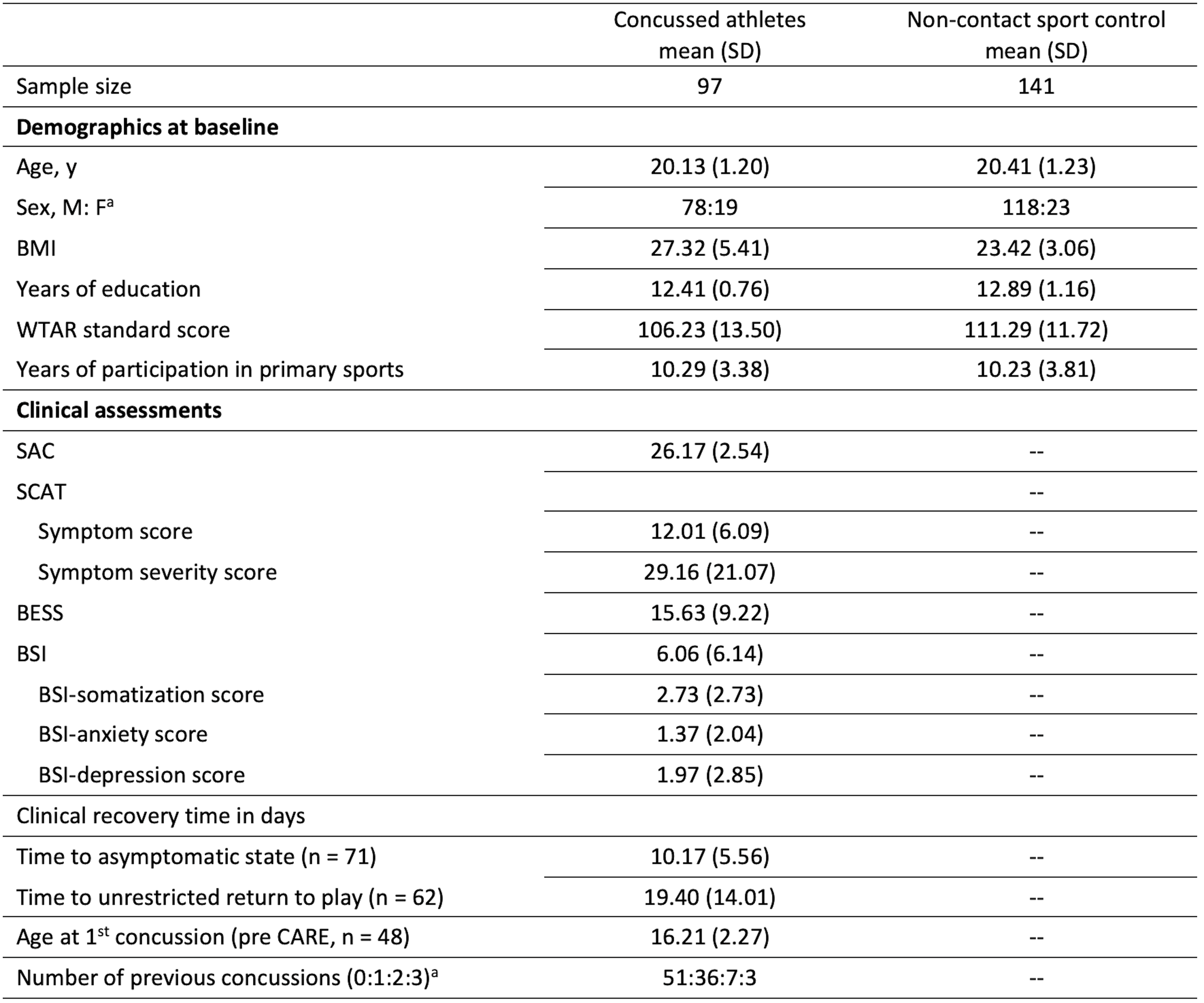
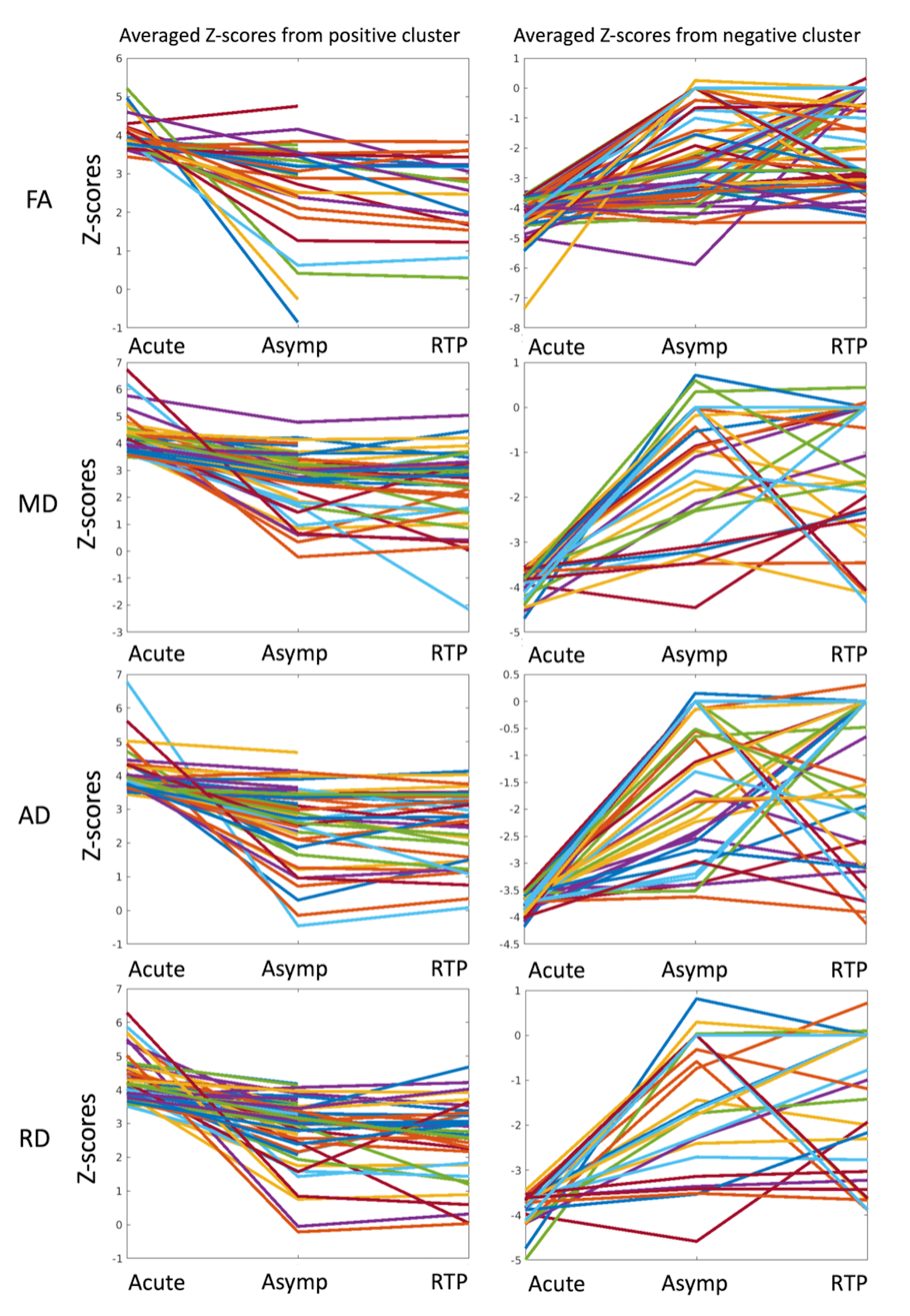
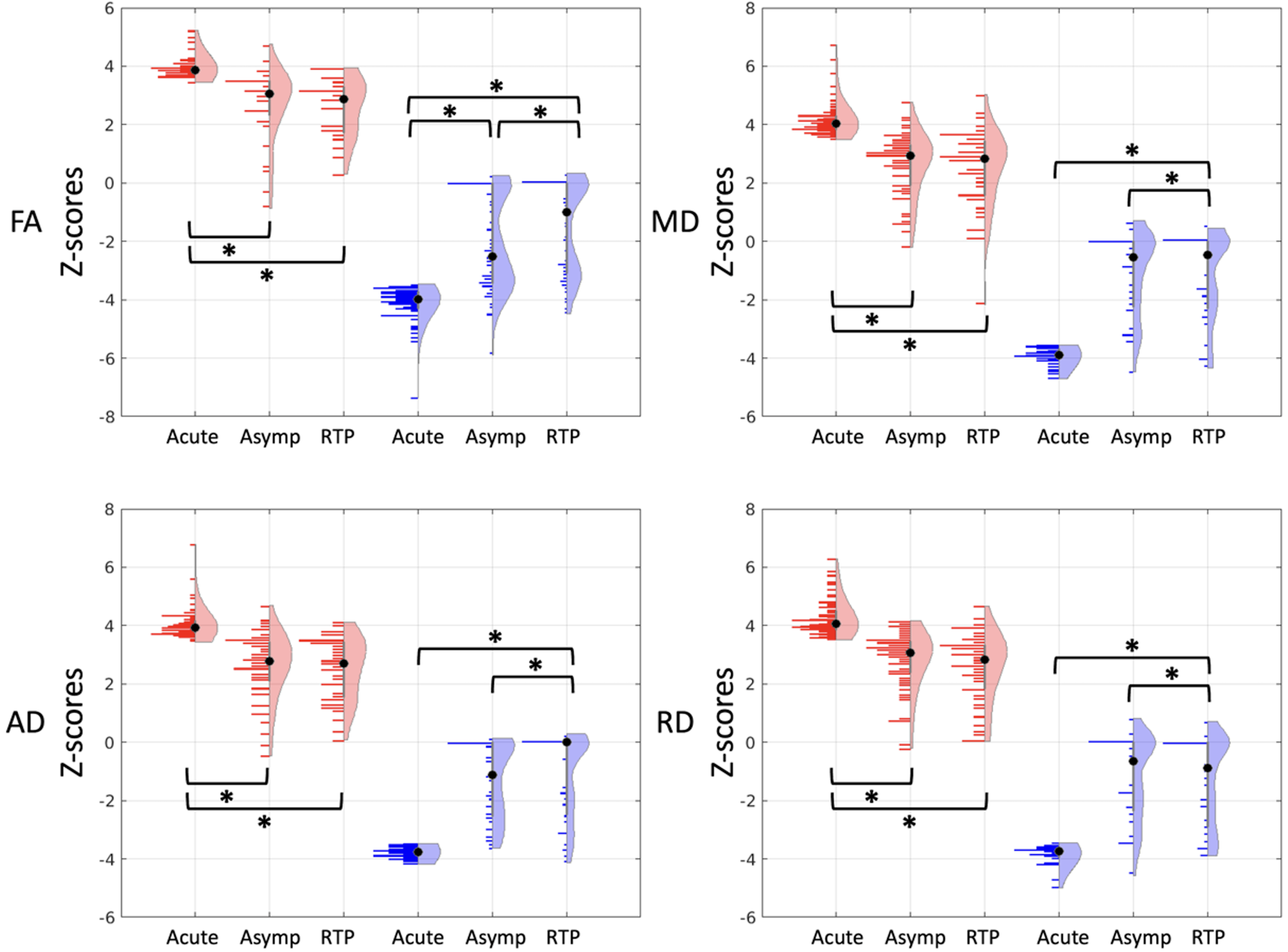
After data QA/QC, 97 concussed athletes and 141 non-contact sport controls with matched demographics had neuroimaging datasets at the acute time point available for the analysis (Table 1). There were 71 and 62 concussed participants with neuroimaging data at Asymp and RTP timepoints, respectively.The existence of heterogeneity in the concussed brains can be appreciated in the projected extreme Z maps (Figure 2), where the exact anatomical locations of extreme Z voxels were distributed and different across the concussed participants, despite some of them being located adjacent to each other in the same white matter tracts. The individualized traces for each DTI metric in Figure 3 illustrate longitudinal trajectory in averaged Z-scores during the acute-to-RTP phase. Figure 4 summarizes the evolving distribution of averaged Z-scores over time. These longitudinal alterations were statistically significant (p’s<0.001) across all DTI metrics and in both positive and negative extreme Z-score masks.
Conclusion
Using the subject-specific analysis, we observed heterogeneity in the post-concussion brain with respect to anatomical locations and recovery trajectories. Despite the individual heterogeneities, some common features exist in certain subgroups. The corpus callosum and internal capsule seem to be more vulnerable in some of the concussed athletes. Over the period between 24 hours postinjury and return to play, some individuals demonstrated persistently high Z-scores, suggesting persistent brain changes, while others showed trends of neutralization of the extreme Z-scores.Acknowledgements
This research was supported by the Grand Alliance Concussion Assessment, Research, and Education (CARE) Consortium, funded in part by the National Collegiate Athletic Association (NCAA) and the Department of Defense (DOD). This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs, through the Combat Casualty Care Research Program, endorsed by the Department of Defense, under Award No. W81XWH1420151. Opinions, interpretations, conclusions and recommendations are those of the author and are not necessarily endorsed by the DOD.References
1. Wu Y-C, Harezlak J, Elsaid NM, et al. Longitudinal white-matter abnormalities in sports-related concussion: A diffusion MRI study. Neurology 2020;95(7):e781-e792.
2. Chamard E, Lassonde M, Henry L, et al. Neurometabolic and microstructural alterations following a sports-related concussion in female athletes. Brain Inj 2013;27(9):1038-1046.
3. Mustafi SM, Harezlak J, Koch KM, et al. Acute White-Matter Abnormalities in Sports-Related Concussion: A Diffusion Tensor Imaging Study from the NCAA-DoD CARE Consortium. Journal of Neurotrauma 2018;35(22):2653-2664.
4. Lancaster MA, Meier TB, Olson DV, McCrea MA, Nelson LD, Muftuler LT. Chronic differences in white matter integrity following sport‐related concussion as measured by diffusion MRI: 6‐Month follow‐up. Human brain mapping 2018;39(11):4276-4289.
5. Wu YC, Mustafi SM, Harezlak J, Kodiweera C, Flashman LA, McAllister TW. Hybrid Diffusion Imaging in Mild Traumatic Brain Injury. J Neurotrauma 2018;35(20):2377-2390.
6. Gardner A, Kay-Lambkin F, Stanwell P, et al. A systematic review of diffusion tensor imaging findings in sports-related concussion. J Neurotrauma 2012;29(16):2521-2538.
7. Wu YC, Harezlak J, Elsaid NMH, et al. Longitudinal white-matter abnormalities in sports-related concussion: A diffusion MRI study. Neurology 2020;95(7):e781-e792.
8. Mustafi SM, Yang HC, Harezlak J, et al. Effects of White-Matter Tract Length in Sport-Related Concussion: A Tractography Study from the NCAA-DoD CARE Consortium. J Neurotrauma 2022.
9. Wu YC, Wen Q, Gill JM, et al. Longitudinal associations between blood biomarkers and white-matter MRI in sport-related concussion: A study of the NCAA-DoD CARE Consortium. Neurology 2023 accepted.
10. Bigler ED. Neuropathology of Mild Traumatic Brain Injury: Correlation to Neurocognitive and Neurobehavioral Findings. In: Kobeissy FH, editor. Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects, Frontiers in Neuroengineering. Boca Raton (FL); 2015.
11. White T, Schmidt M, Karatekin C. White matter 'potholes' in early-onset schizophrenia: a new approach to evaluate white matter microstructure using diffusion tensor imaging. Psychiatry Res 2009;174(2):110-115.
12. Mac Donald CL, Johnson AM, Cooper D, et al. Detection of blast-related traumatic brain injury in US military personnel. New England journal of medicine 2011;364(22):2091-2100.
13. Mayer AR, Bedrick EJ, Ling JM, Toulouse T, Dodd A. Methods for identifying subject‐specific abnormalities in neuroimaging data. Human brain mapping 2014;35(11):5457-5470.
14. Broglio SP, McCrea M, McAllister T, et al. A national study on the effects of concussion in collegiate athletes and US military service academy members: the NCAA–DoD concussion assessment, research and education (CARE) consortium structure and methods. Sports medicine 2017;47(7):1437-1451.
15. Mustafi SM, Harezlak J, Koch KM, et al. Acute white-matter abnormalities in sports-related concussion: a diffusion tensor imaging study from the NCAA-DoD CARE Consortium. Journal of neurotrauma 2018;35(22):2653-2664.
16. Manjon JV, Coupe P, Concha L, Buades A, Collins DL, Robles M. Diffusion weighted image denoising using overcomplete local PCA. PloS one 2013;8(9):e73021.
17. Andersson JL, Sotiropoulos SN. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage 2016;125:1063-1078.
18. Avants BB, Tustison N, Song G. Advanced normalization tools (ANTS). Insight j 2009;2(365):1-35.
19. Fortin J-P, Parker D, Tunç B, et al. Harmonization of multi-site diffusion tensor imaging data. Neuroimage 2017;161:149-170.
Figures