2141
Low-rank based motion correction followed by automatic frame selection in diffusion tensor CMR1Bioengineering Department and Imperial-X, Imperial College London, London, United Kingdom, 2Cardiovascular Magnetic Resonance Unit, Royal Brompton Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom, 3National Heart and Lung Institute, Imperial College London, London, United Kingdom, 4School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom
Synopsis
Keywords: Diffusion Analysis & Visualization, Motion Correction
Motivation: Post-processing of in-vivo diffusion tensor CMR (DT-CMR) is challenging due to the low SNR and variation in contrast between frames which makes image registration difficult, and the need to manually reject frames corrupted by motion.
Goal(s): To develop a semi-automatic post-processing pipeline for robust DT-CMR registration and automatic frame selection.
Approach: We used low intrinsic rank averaged frames as the reference to register other low-ranked frames. A myocardium-guided frame selection rejected the frames with signal loss, through-plane motion and poor registration.
Results: The proposed method outperformed our previous noise-robust rigid registration on helix angle data quality and reduced negative eigenvalues in healthy volunteers.
Impact: This improved image registration and frame selection algorithm may enable groupwise deformable registration on DT-CMR, paving the way towards clinical translation.
Introduction
Diffusion tensor CMR (DT-CMR) depicts myocardial microstructure non-invasively. Repeated breath-holding and cardiac triggering are used to mitigate motion during in-vivo acquisitions, which include multiple diffusion encoding directions and averages. Nevertheless, DT-CMR is still susceptible to cardiac and respiratory motion artifacts. Conventionally, pairwise rigid/affine image registrations are employed to correct in-plane motion in STEAM/SE data, and frames exhibiting either cardiac and respiratory motion induced signal loss or through-plane motion are manually excluded during post-processing. However, the selection of an appropriate reference image for registration is challenging due to the diverse contrasts and cardiac and respiratory motion, which influences the successive pairwise registration. The subjective nature of excluding images with poor registration, through-plane motion, or bulk motion induced signal loss presents a further challenge. Here, we adopted the use of low-rank images to facilitate quicker registration, coupled with an automatic frame selection process to enhance the robustness of the DT-CMR post-processing workflow.Methods
12 healthy volunteers were scanned at both 3T and 1.5T, with both STEAM and SE-EPI with resolution 2.8x2.8x8 mm3, b0 data and 6 encoding directions at b = 150 and 600 s/mm2 with 10.0 [10.0 12.0] averages in short-axis view at systole/diastole. Zonal excitation led to rectangular field-of-view (FOV) with 256x96px. The central 96x96px region was automatically cropped. Four SE-diastole cases were discarded due to poor image quality.We conducted a comparative analysis between the proposed method (Fig. 1) and our in-house developed method chracterized by manual circular cropping aimed at diminishing the high-intensity signal from adjacent organs, a rapid rigid registration1, and a manual selection of frames. We represented all the images $$$Α = N_x\times N_y\times N_{ave}\times N_{DWI}$$$ in the Tucker form2:
$$Α = \phi_{xy} \cdot \phi_{dyn}$$
where $$$\phi^{N_x\times N_y \times L_1}$$$ is the image basis matrix and $$$\phi^{L_1\times N_{ave} \times N_{DWI}}_{dyn}$$$ is the dynamic factor tensor. $$$L_i$$$ is the $$$i^{th}$$$ rank for a given basis matrix. After automatic central cropping, the geometric average $$$A^{L_1=1}$$$ images were taken as the reference since they disentangled the respiratory and local shape deformations (Fig. 2). Derived from a PCA denoised method3, we set $$$A^{L_1=6}$$$ as moving frames. Affine/rigid transformation parameters, derived from the registration between the averaged and denoised frames, were applied to the original diffusion-encoded frames.
The ROI was determined to be a donut-shaped area centred on the manually annotated blood pool for automatic frame selection. The inner radius was set at 95% of the shortest distance from the labelled myocardium boundary, while the outer radius extended to 105% of the maximum distance, ensuring precise delineation of the myocardium. We employed a Pearson correlation to exclude outliers situated more than three scaled median absolute deviations below the median value4.The RMSE, R-square of the fitting of helix angle (HA) line profiles, number of negative eigenvalues in the myocardium, and horizontal and vertical visualization were chosen as evaluations5.
Affine/rigid registrations for SE/STEAM were implemented using itk-elastix6 in python, with 150 iterations and a single-resolution. The previous rigid registration used dft-registration1 in MATLAB.
Results
Denoised images $$$A^{L_1=6}$$$ were less susceptible to the high-intensity signal from surrounding organs, hence the automatic square cropping replaced manual circular cropping with enhanced registration robustness and expediting convergence (Fig. 2).The dft-registration1 processed 63 frames in approximately 0.2 seconds, while both rigid/affine registrations in elastix took around 20 seconds. Although with a high computational efficiency, dft-registration failed if suboptimal manual cropping has included the high intensity regions of the surrounding chest wall (Fig. 3).
It is noteworthy that the frame selection previously utilized for STEAM-EPI4 has also been effectively adapted for SE data. Thanks to the improved registration, less frames were discarded using the proposed approach.
When fitting DT-CMR parameters, the proposed registration outperformed the previous in-house workflow which just relied on the original images. It showed HA line profiles with higher R-square, lower RMSE, less percentage of negative eigenvalues in the myocardium in both SE/STEAM and comparable visualization with less manual post-processing burden (Fig. 4, Table 1).
Conclusion and Discussion
We proposed a method using low-rank decomposition as pre-processing to enable a robust rigid/affine registration of in-vivo DT-CMR data. Automatic frame selection was guided by Pearson correlation within the myocardium-segmentation guided part. Instead of choosing the reference image with brightest frame, the proposed method averaged the low-rank frames which discarded the local deformation, respiratory motion and noise as the reference to boost the registration. Our method encountered limitations, including increased computational time and less accurate cropping for off-center hearts. This improved registration and frame selection algorithm may enable groupwise deformable registration on DT-CMR, paving the way towards clinical translation.Acknowledgements
This study was supported in part by the BHF programme grant RG/19/1/34160, ERC IMI (101005122), the H2020 (952172), the MRC (MC/PC/21013), the Royal Society (IEC\NSFC\211235), the NVIDIA Academic Hardware Grant Program, the SABER project supported by Boehringer Ingelheim Ltd, and the UKRI Future Leaders Fellowship (MR/V023799/1).
References
[1] Guizar-Sicairos M, Thurman ST, Fienup JR. Efficient subpixel image registration algorithms. Opt Lett 2008;33(2):156-158. doi: 10.1364/OL.33.0001562.
[2] Nguyen CT, Christodoulou AG, Coll-Font J, Ma S, Xie Y, Reese TG, Mekkaoui C, Lewis GD, Bi X, Sosnovik DE, Li D. Free-breathing diffusion tensor MRI of the whole left ventricle using second-order motion compensation and multitasking respiratory motion correction. Magn Reson Med 2021;85(5):2634-2648. doi: 10.1002/mrm.286113.
[3] Gurney-Champion OJ, Collins DJ, Wetscherek A, Rata M, Klaassen R, Laarhoven HWMv, Harrington KJ, Oelfke U, Orton MR. Principal component analysis for fast and model-free denoising of multi b-value diffusion-weighted MR images. Physics in Medicine & Biology 2019;64(10):105015. doi: 10.1088/1361-6560/ab17864.
[4] Ferreira PF, Martin RR, Scott AD, Khalique Z, Yang G, Nielles-Vallespin S, Pennell DJ, Firmin DN. Automating in vivo cardiac diffusion tensor postprocessing with deep learning-based segmentation. Magn Reson Med 2020;84(5):2801-2814. doi: 10.1002/mrm.282945.
[5] Ferreira PF, Kilner PJ, McGill L-A, Nielles-Vallespin S, Scott AD, Ho SY, McCarthy KP, Haba MM, Ismail TF, Gatehouse PD, de Silva R, Lyon AR, Prasad SK, Firmin DN, Pennell DJ. In vivo cardiovascular magnetic resonance diffusion tensor imaging shows evidence of abnormal myocardial laminar orientations and mobility in hypertrophic cardiomyopathy. Journal of Cardiovascular Magnetic Resonance 2014;16(1):87. doi: 10.1186/s12968-014-0087-86.
[6] Klein S, Staring M, Murphy K, Viergever MA, Pluim JPW. elastix: A Toolbox for Intensity-Based Medical Image Registration. IEEE Transactions on Medical Imaging 2010;29(1):196-205. doi: 10.1109/TMI.2009.2035616
Figures
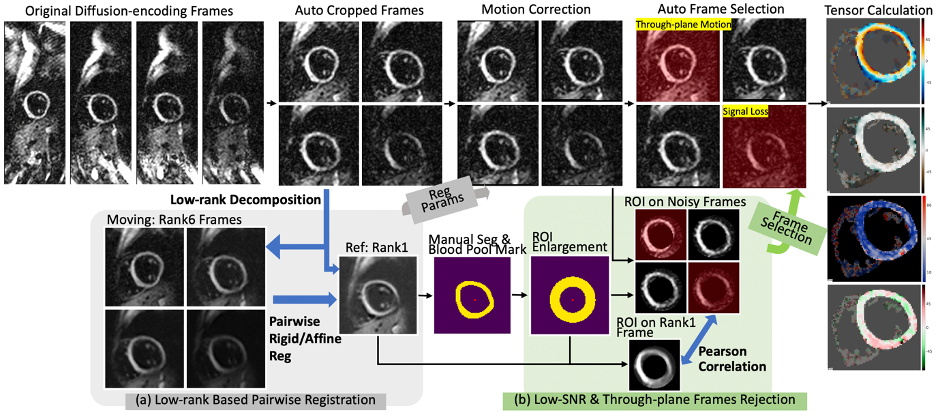
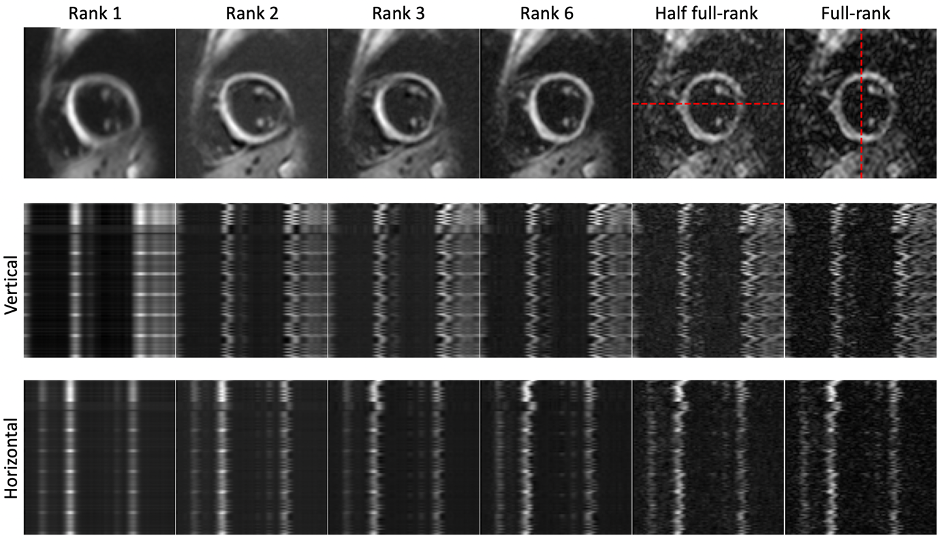
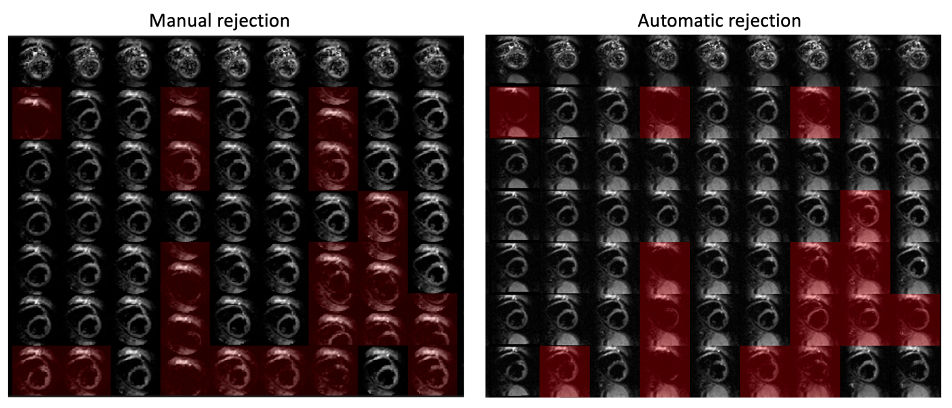
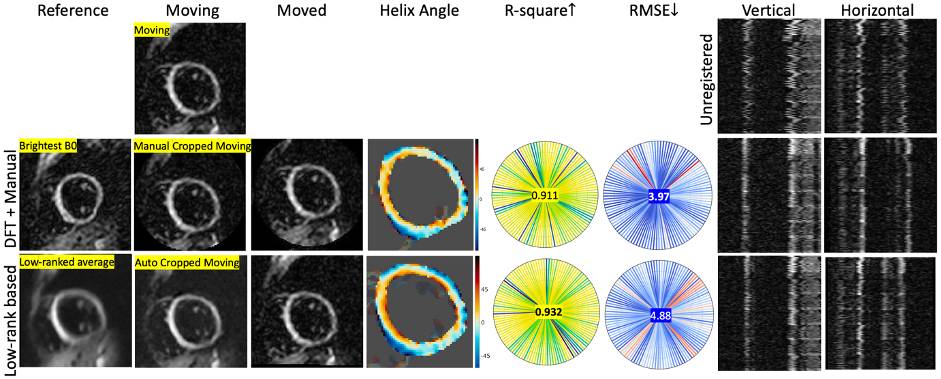
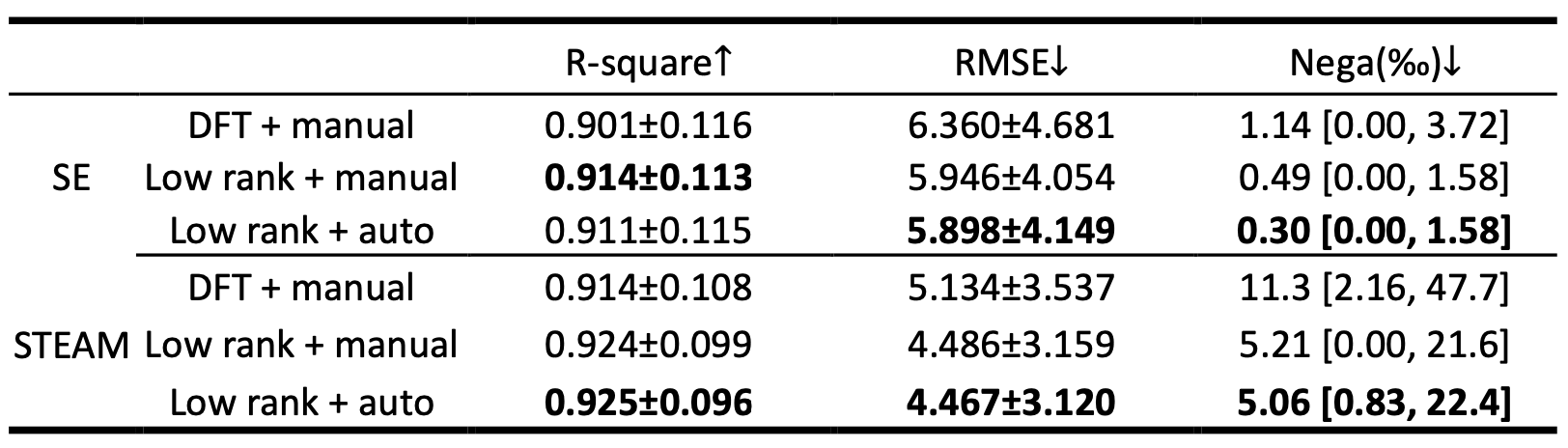
Table 1. Statistical metrics of the proposed method. DFT and low-rank denote the rigid registration and the proposed method. The R-square and RMSE are shown in mean ± std. The term "Nega" refers to the proportion, expressed per thousand, of pixels within the myocardial tissue that has negative eigenvalues . They are shown in median [percentile25 percentile75]. Manual and auto stand for the manual and automatic frame selection respectively.