2119
Causal discovery of morphological changes in thoracic aorta: Investigation on a large epidemiological non-contrast-enhanced MRI cohort1Medical Image and Data Analysis (MIDAS.lab), Department of Diagnostic and Interventional Radiology, University Hospital of Tuebingen, Tuebingen, Germany, 2Institute of Signal Processing and System Theory, University of Stuttgart, Stuttgart, Germany, 3Stanford Medicine, Department of Radiology, Palo Alto, CA, United States
Synopsis
Keywords: Analysis/Processing, Vessels, Thoracic Aorta, Segmentation, Landmark Detection, Causal Discovery
Motivation: The thoracic aorta is often affected by life-threatening, undetected morphological changes. Prior works primarily focused on factors correlating with aortic aneurysms but lack the investigation of causal influences related to morphological changes.
Goal(s): Our goal is to perform automatic aortic shape analysis inline on the scanner. We investigate causal dependencies between metadata and thoracic aortic diameter in approx. 30,000 non-contrast-enhanced MRA.
Approach: We apply a deep learning framework for shape analysis and Peter-Clark-algorithm to investigate causal influences on the thoracic aorta.
Results: We found that sex, age, height, BMI, hypertension, and vascular-stiffness causally impact the aorta’s diameter, whereas diabetes lacks a causal relationship.
Impact: This study reveals causal influences on morphological changes of the thoracic aorta using a large epidemiological dataset (~30,000 non-contrast-enhanced-MRA). A deep-learning-based framework supports the identification of causal factors impacting the aortic diameter and thereby, enabling early detection of life-threatening risks.
Introduction
MRI allows due to its high soft tissue contrast a reliable detection of life-threatening pathological changes in the thoracic aorta. Pathological changes like the expansion of the aortic diameter can lead to aneurysms. The dilation is influenced by multiple factors [1]. Previous studies [2-4] explored such factors correlating with aortic aneurysms but lack the investigation of real causal influences. However, the occurrence of confounding factors in datasets conceals the causal relationship and creates spurious-correlations which can lead to wrong conclusions and diagnoses.For instance, if daily alcohol consumers exhibit larger aortic diameters than nondrinkers, a correlation exists between alcohol consumption and diameter size. However, suppose daily drinkers are significantly older than nondrinkers. In this case, age might create a spurious-correlation between the alcohol and the diameter size as age influences both factors. Hence, in the presence of the variable age, alcohol consumption and diameter size are independent (Common Cause Principle [5]).
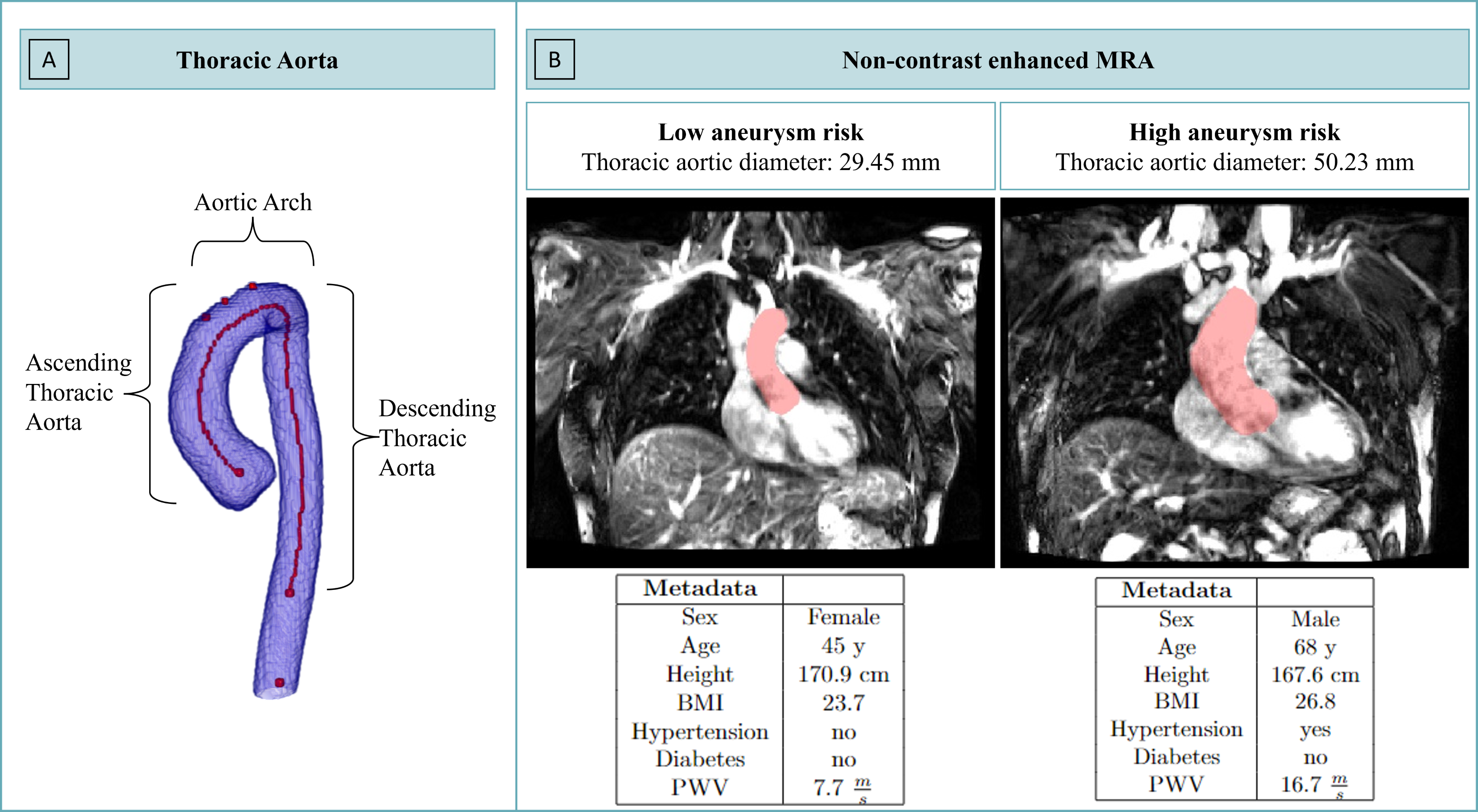
In this study, we investigate causal influences for changes in the thoracic aorta's diameter (Fig.1A). Previous studies lack access to large epidemiological databases with metadata (e.g., age, anthropometric measures, hypertension, diabetes), hindering both causal discovery and comprehensive analysis. Our method is investigated on 30,000 non-contrast-enhanced MRA of the German National Cohort (GNC) which includes ~250 metadata per subject (Fig.1B) allowing an extensive causal discovery.
Therefore, (1) an automatic deep learning (DL)-based segmentation and landmark point detection of the thoracic aorta including an automated shape analysis is developed; (2) causal relationships between the MRI and non-imaging metadata are investigated. The trained network is subsequently deployed in the inline scanner reconstruction for automatic shape analysis and abnormality detection.
Methods
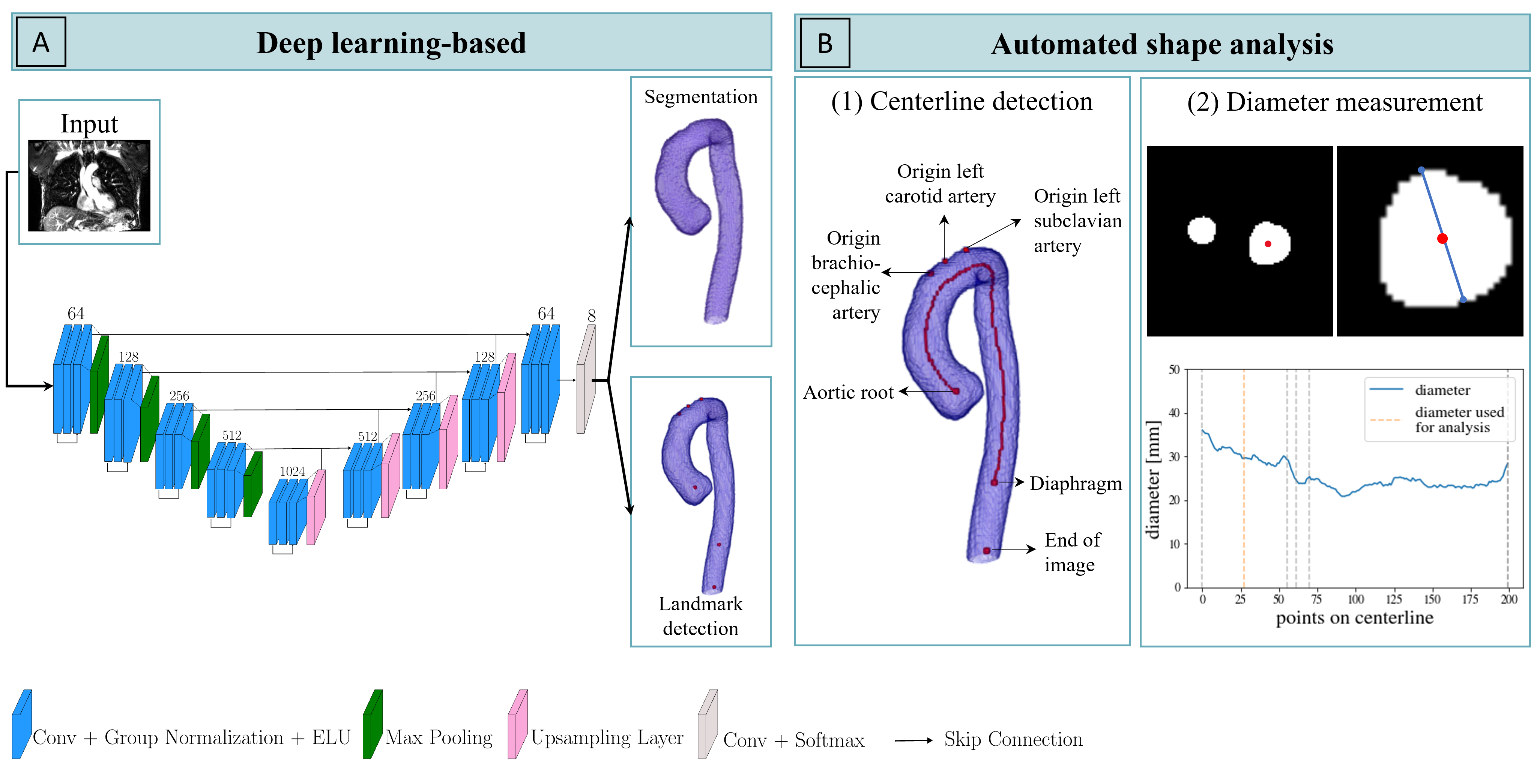
Segmentation: We developed a DL-based residual-UNET to segment the thoracic aorta from non-contrast-enhanced MRA. Extending our prior model [6], this novel approach predicts the segmentation mask and six landmark points to separate the thoracic aorta into the aortic arch, ascending, and descending part (Fig.2A).Shape analysis: To automatically measure the diameter of the aorta, we compute the centerline with the fast-marching-method (FMM)[7] (Fig.2B-1). With the centerline, the diameter is automatically measured along 200 equally-distributed points of the thoracic aorta (Fig.2B-top). For the following analysis, we use the diameter measured in the middle of the ascending aorta(Fig.1A/Fig.2B-2 orange).
Statistical and causal analysis:
Causal dependence between the aortic diameter and the respective metadata is discovered with the Peter-Clark-algorithm (PC)[8] which bases on the Common Cause Principle [5]. Additionally, various statistical tests, including Mann-Whitney-U-Test and Pearson's correlation, are used to quantify correlations.
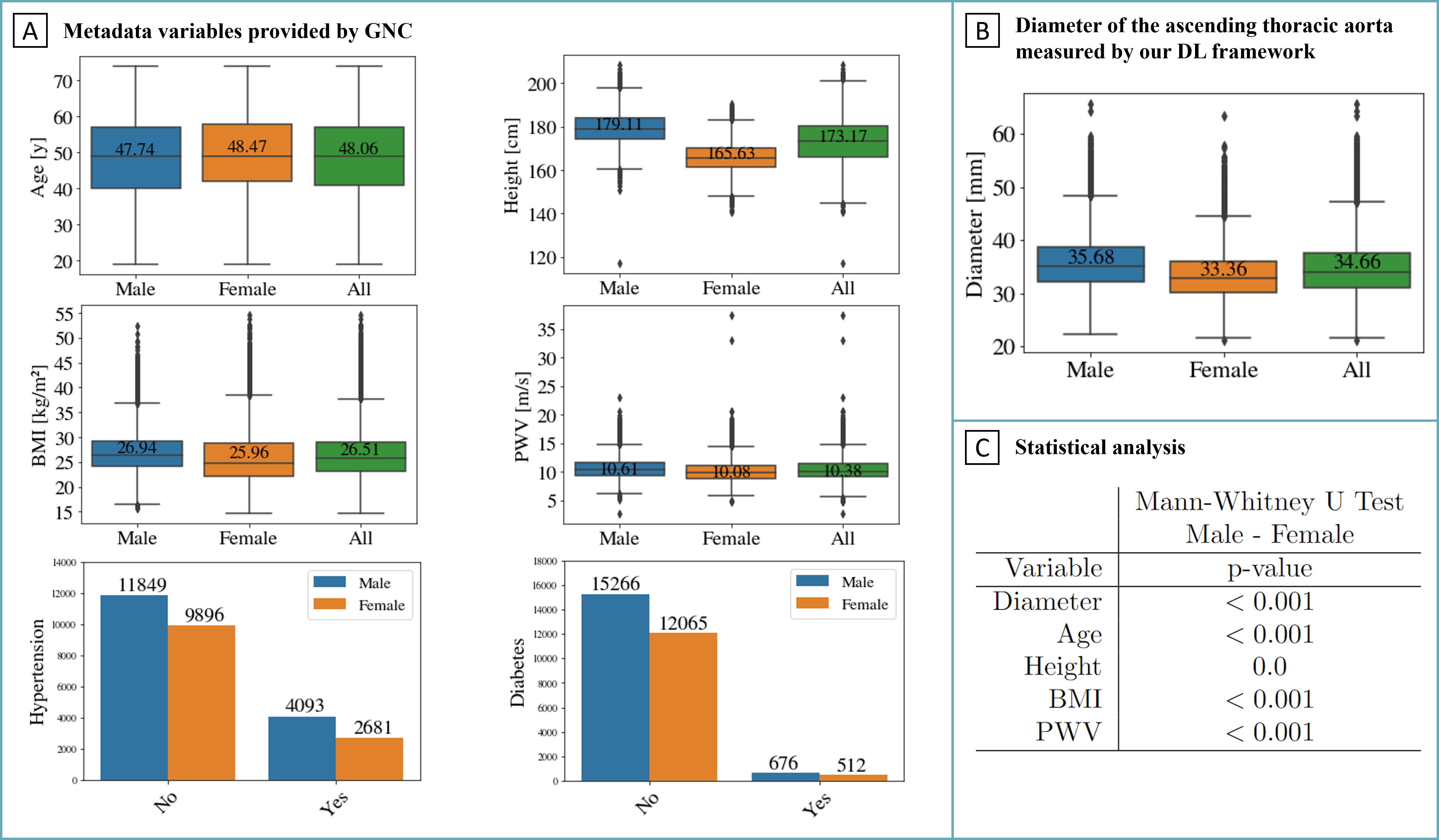
Data: Analysis is performed on ~30,000 non-contrast-enhanced T2-weighted MRI of the thoracic aorta of the German National Cohort (GNC) (female:11679, male:15147, age:48.06±12.26 [19y to 74y]) acquired at 3T Siemens Skyra with spatial resolution: 1.2x1.2x2.5mm3, matrix size: 240x320x104, TE=102ms, TR=5951ms, flip angle=150°, pixel bandwidth=650Hz/pixel, and acquisition time 4:20min:s. From the ~250 metadata, we used: sex, age, height, BMI, hypertension, diabetes, and vascular stiffness (Fig.3A).
Results and Discussion
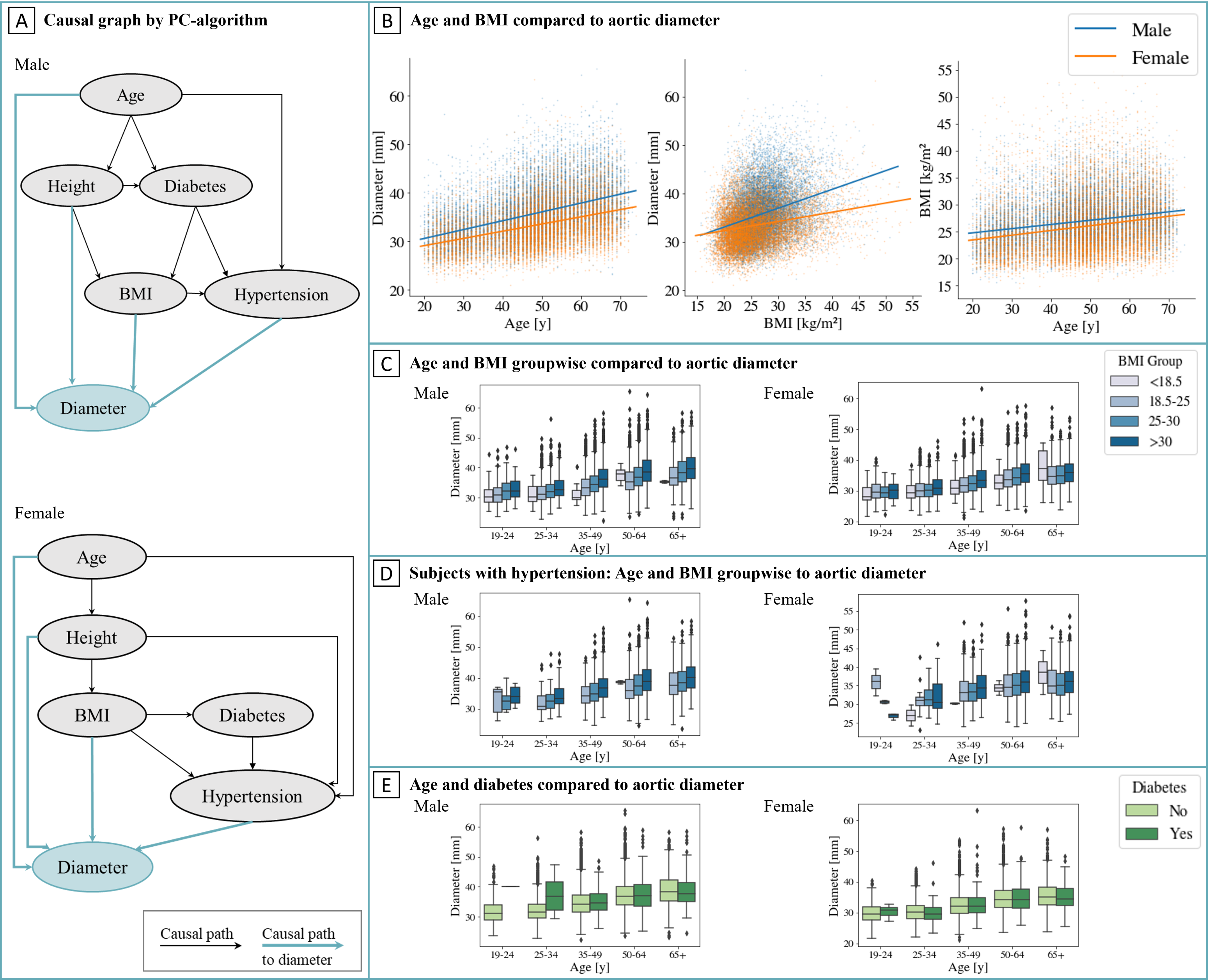
Fig.3B shows the resulting diameter distribution of all subjects. Since male and female subjects show statistical independence (Fig.3C) for all our observed variables, investigations are performed sex-individual.Experiment-1: Causal Discovery of Age-Height-BMI-Hypertension-Diabetes-Diameter
Age, height, BMI, hypertension, and diabetes are presumed to correlate with aortic aneurysms [9,10], and all but diabetes exhibit causal relationships with aortic diameter (Fig.4A). Since diameter increases with age and BMI (Fig.4B), we split age and BMI into groups to demonstrate that these relationships are not spurious. Within each age group for all subjects and for the subgroup with hypertension, diameter size rises with increasing BMI, validating the causal relationships established by PC (Fig.4C-D). Diabetes, however, only influences hypertension causally; no direct association with diameter size is observed (Fig.4E).
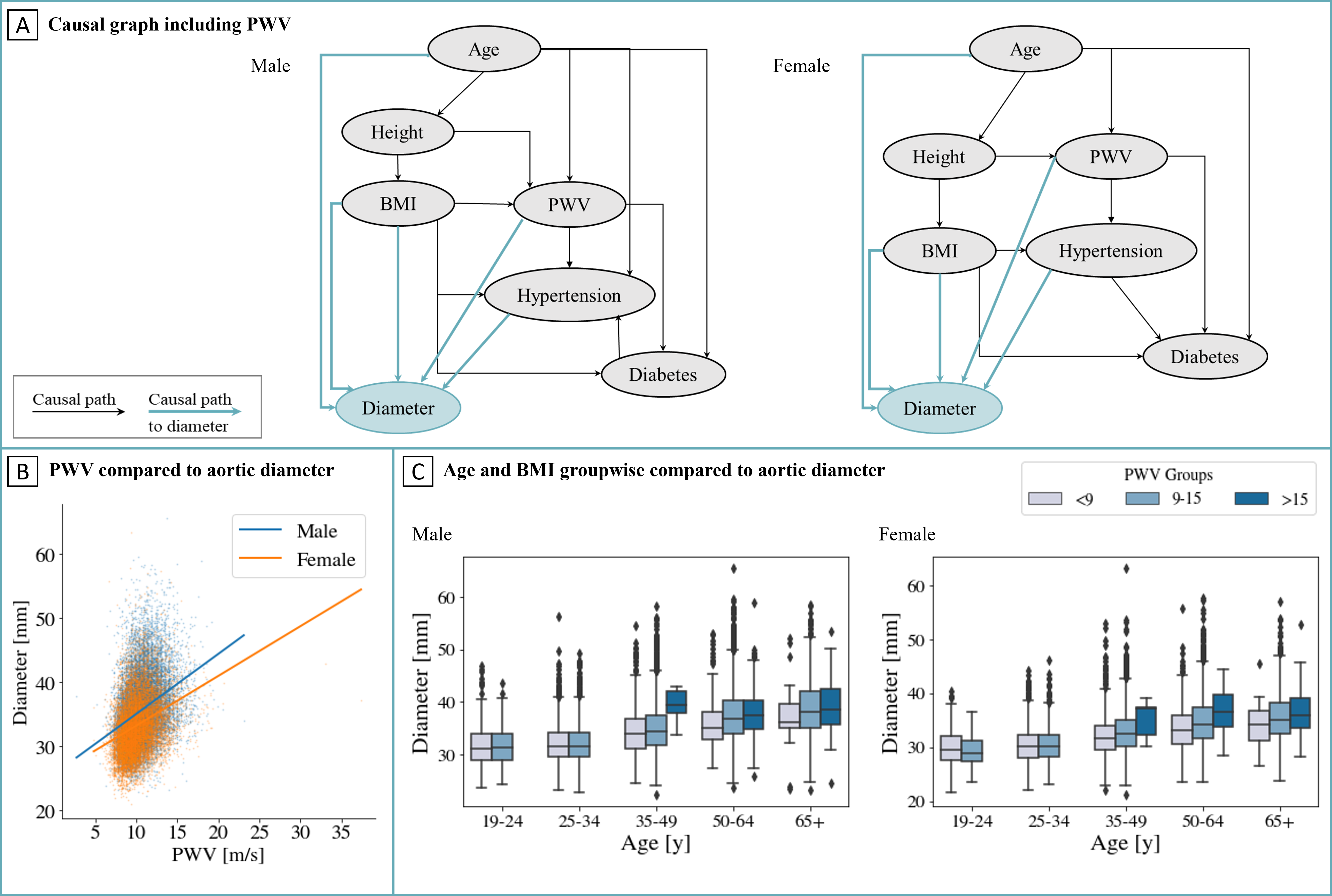
Experiment-2: Extended Causal Discovery including Vascular Stiffness
In this follow-up experiment, brachial-ankle pulse wave velocity (PWV), known as vascular stiffness, is additionally incorporated into the causal model (Fig.5A). PWV causally influences the aortic diameter. An increasing PWV exhibits an increased diameter size (Fig.5B). Since vascular stiffness is known to correlate with age [11], Fig.5C demonstrates that the aortic diameter increases with rising PWV age-independent.
We acknowledge some limitations. This work confines to the above-described metadata. However, it is infeasible to examine all metadata, so crucial factors affecting aortic diameter are potentially omitted.
Conclusion and Outlook
In conclusion, we confirmed causal relationships between the thoracic aorta's diameter and age, height, BMI, hypertension, and vascular stiffness (Fig.5A). These findings enhance the comprehension of thoracic aortic pathology, including aortic aneurysm development, providing valuable insights for prognostic diagnosis. Our trained network is translated to the MRA workflow, by performing DL-based segmentation and shape derivation inline on the scanner which allows automated analysis and abnormality checks.Acknowledgements
S.G. and T.K. contributed equally.This project was conducted with data from the German National Cohort (GNC) (www.nako.de). The GNC is funded by the Federal Ministry of Education and Research (BMBF) (project funding reference no. 01ER1301A/ B/C and 01ER1511D), federal states, and the Helmholtz Association, with additional financial support from the participating universities and institutes of the Leibniz Association. We thank all participants who took part in the GNC study and the staff in this research program.
References
- Elefteriades JA. Natural history of thoracic aortic aneurysms: indications for surgery, and surgical versus nonsurgical risks. The Annals of thoracic surgery. 2002;74(5):S1877‐S1880.
- Chen T, Yang X, Fang X et al. Potential influencing factors of aortic diameter at specific segments in population with cardiovascular risk. BMC Cardiovascular Disorders. 2022;22(1):32.
- Mancusi C, Manzi MV, Lembo M et al. Normalization of ascending aorta dimension for body size influences pathophysiologic correlation in hypertensive patients: the Campania Salute Network. European Journal of Preventive Cardiology. 2023:zwad224.
- Mensel B, Heßelbarth L, Wenzel M, et al. Thoracic and abdominal aortic diameters in a general population: MRI-based reference values and association with age and cardiovascular risk factors. European radiology. 2016;26:969–978.
- Reichenbach H. The direction of time: Univ of California Press; 1991. (vol. 65).
- Hepp T, Fischer M, Winkelmann MT et al. Fully automated segmentation and shape analysis of the thoracic aorta in non‐contrast-enhanced magnetic resonance images of the German National Cohort Study. Journal of Thoracic Imaging. 2020;35(6):389–398.
- Sethian JA. Fast marching methods. SIAM review. 1999;41(2):199–235.
- Spirtes P, Glymour C, Scheines R. Causation, Prediction, and Search. Causation, Prediction, and Search [Internet]. 1993;81 doi: 10.1007/978-1-4612-2748-9
 .
. - Huang Z, Su H, Zhang T et al. Double-edged sword of diabetes mellitus for abdominal aortic aneurysm. Frontiers in Endocrinology. 2022;13:1095608.
- Rooprai J, Boodhwani M, Beauchesne L et al. Central hypertension in patients with thoracic aortic aneurysms: prevalence and association with aneurysm size and growth. American Journal of Hypertension. 2022;35(1):79–86.
- Vatner SF, Zhang J, Vyzas C et al. Vascular stiffness in aging and disease. Frontiers in Physiology. 2021;12:762437.
Figures