2117
Advancing Neoadjuvant Chemotherapy Response Prediction through Deep Learning-Enabled Retrospective Quanfication of Pharmacokinetics1Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2Department of Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States, 3Radiology Department, Stanford University, Stanford, CA, United States, 4Karsh Division of Gastroenterology and Hepatology, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 5Department of Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States
Synopsis
Keywords: Analysis/Processing, Machine Learning/Artificial Intelligence
Motivation: While multiphasic contrast-enhanced MRI has propelled noninvasive pCR prediction in breast cancer, its limited temporal resolution restricts quantitative analysis, affecting generalizability and interpretability.
Goal(s): To enhance pCR prediction, we integrated retrospective pharmacokinetic quantification by addressing the temporal resolution limit using deep learning.
Approach: We incorporated a novel retrospective pharmacokinetic quantification approach into our pCR prediction model to better capture the tumor microenvironment's pharmacokinetic indicators.
Results: Our approach improved predictive accuracy in external test datasets, demonstrating the method's superior performance and broader applicability.
Impact: Deep-learning pharmacokinetic quantification enhances the accuracy and applicability of pCR prediction using multiphasic DCE-MRI, offering the potential for precise pre-treatment evaluation that could streamline NAC targeting and minimize initiation delays for breast cancer patients unlikely to respond to standard treatments.
Purpose
Neoadjuvant chemotherapy (NAC) is a primary treatment modality for locally advanced breast cancer1, with the success benchmark being pathological complete response (pCR), which significantly enhances prognosis. Given the variation in pCR rates (10–50%), precise pre-treatment predictors of pCR are crucial for customizing treatment plans and averting delays in cases unresponsive to NAC2. Previous studies3-7 leveraging dynamic contrast-enhanced MRI (DCE-MRI) for imaging predictors have predominantly focused on spatial features, resulting in limited generalizability and reproducibility5 due to protocol variations across sites.Pharmacokinetic parameters, however, are recognized as consistent predictors of pCR8 and are reproducible in breast tissue9,10. Yet, their quantitative analysis in clinical DCE-MRI is impeded by inadequate temporal resolution and a limited number of phases.
Addressing this issue, we employed a novel deep learning-based retrospective quantification (RoQ) technique11,12 to derive quantitative pharmacokinetic parameters from standard multi-phasic DCE-MRI scans. We trained a deep learning model using these retrospectively quantified pharmacokinetics for pCR prediction. The model's predictive capability for pCR was validated on datasets from both the training site and an external site. Our findings suggest that the RoQ-enhanced model exhibits improved predictive performance and better generalizability, withstanding variations in imaging protocols.
Materials and Methods
Data Description:Our study involved two clinical DCE-MRI datasets: the Duke Breast Cancer MRI dataset13 and the Cedars-Sinai Breast Cancer dataset. The Duke dataset comprised pre-treatment DCE-MRI scans of 300 breast cancer patients treated with neoadjuvant chemotherapy between 2000 and 2014, with 64 patients achieving pCR. The Cedars-Sinai dataset included 32 patients, with 13 exhibiting pCR. We used the Duke dataset for training (split 80:20 for training and validation) and the Cedars-Sinai dataset for external testing.
Image Preprocessing:
The preprocessing workflow is depicted in Figure 1. We centralized the tumor region in images from both datasets, aligned them to the first post-contrast phase14, and normalized their intensities. An experienced radiologist delineated the tumor ROI. We then applied retrospective pharmacokinetic quantification12 to obtain both semi-quantitative (i.e. time-to-peak, maximum signal intensity, wash-in rate, wash-out rate) and quantitative parameters (i.e. $$$K^{trans}$$$, $$$k_{ep}$$$, $$$v_e$$$), as illustrated in Figure 2.
Network Architecture:
Our model's architecture is presented in Figure 3. It processes batched 3D volumes with variable channels, standardizing to three channels via a Conv3D layer before input to a finetune-able ResNet-50 equipped with pre-trained weights. A linear classifier with softmax activation was employed, with binary focal cross-entropy loss to address class imbalance, using an empirically determined alpha of 0.1. We developed the network in TensorFlow, training with an Adam optimizer starting at a learning rate of 10-4, decreasing by tenfold after validation loss plateaued for five epochs. Training concluded after 50 epochs.
Experiment Settings:
We assessed performance across three configurations: (A) using only three subtracted post-contrast phases, (B) only seven RoQ-derived maps, and (C) a combination of both. Each model underwent independent training and was evaluated on both validation and test datasets.
Results
Representative DCE-MRI scans and RoQ maps for one patient with pCR and one without are displayed in Figure 4. Figure 5 presents the receiver operating characteristic (ROC) curves for the three experimental setups, alongside the respective area under the curve (AUC) values for both the validation and test datasets. In the validation set, models based on image features, RoQ maps, and combined image-RoQ input achieved ROC-AUC scores of 0.421, 0.725, and 0.652, respectively. Corresponding scores in the test dataset were 0.628, 0.672, and 0.381. Across both datasets, the RoQ-based model not only outperformed the image-based and combined input models in terms of ROC-AUC but also exhibited more consistent results between the datasets, underscoring its superior generalizability.Discussion and Conclusion
Our study has established that incorporating RoQ into the prediction models markedly enhances the noninvasive prediction of pathological complete response (pCR) to neoadjuvant chemotherapy (NAC) in breast cancer patients.The use of RoQ maps independently demonstrated superior predictive performance and stability across multiple datasets when compared to traditional image-based approaches. This advancement indicates a significant step forward in the generalizability and reliability of pCR prediction models, paving the way for more individualized and effective pre-treatment planning. There was relatively less improving in the external dataset, which could be due to limited size of test dataset. Still, the stability of RoQ across different datasets highlights its potential as a standardizable biomarker in breast cancer treatment protocols, promising a reduction in treatment initiation delays for patients unlikely to respond to conventional chemotherapy regimens. Moving forward, the integration of RoQ into clinical practice has the potential to better assist the clinical-decision making of NAC, leading to improved patient outcomes and optimized healthcare resources.
Acknowledgements
No acknowledgement found.References
1. Thompson A, Moulder-Thompson S. Neoadjuvant treatment of breast cancer. Annals of oncology. 2012;23:x231-x236.
2. Earl H, Provenzano E, Abraham J, et al. Neoadjuvant trials in early breast cancer: pathological response at surgery and correlation to longer term outcomes–what does it all mean? BMC medicine. 2015;13:1-11.
3. Adoui ME, Drisis S, Benjelloun M. Predict breast tumor response to chemotherapy using a 3D deep learning architecture applied to DCE-MRI data. Paper presented at: International work-conference on bioinformatics and biomedical engineering2019.
4. Braman NM, Etesami M, Prasanna P, et al. Intratumoral and peritumoral radiomics for the pretreatment prediction of pathological complete response to neoadjuvant chemotherapy based on breast DCE-MRI. Breast Cancer Research. 2017;19:1-14.
5. Khan N, Adam R, Huang P, Maldjian T, Duong TQ. Deep learning prediction of pathologic complete response in breast cancer using MRI and other clinical data: a systematic review. Tomography. 2022;8(6):2784-2795.
6. Li Y, Fan Y, Xu D, et al. Deep learning radiomic analysis of DCE-MRI combined with clinical characteristics predicts pathological complete response to neoadjuvant chemotherapy in breast cancer. Frontiers in Oncology. 2023;12:1041142.
7. Liu T, Wang H, Yu S, Feng F, Zhao J. A Soft-Attention Guidance Stacked neural Network for neoadjuvant chemotherapy’s pathological response diagnosis using breast dynamic contrast-enhanced MRI. Biomedical Signal Processing and Control. 2023;86:105145.
8. Lee J, Kim SH, Kang BJ. Pretreatment prediction of pathologic complete response to neoadjuvant chemotherapy in breast cancer: perfusion metrics of dynamic contrast enhanced MRI. Scientific Reports. 2018;8(1):1-8.
9. Galbraith SM, Lodge MA, Taylor NJ, et al. Reproducibility of dynamic contrast‐enhanced MRI in human muscle and tumours: comparison of quantitative and semi‐quantitative analysis. NMR in Biomedicine: An International Journal Devoted to the Development and Application of Magnetic Resonance In Vivo. 2002;15(2):132-142.
10. Yang C, Karczmar GS, Medved M, Oto A, Zamora M, Stadler WM. Reproducibility assessment of a multiple reference tissue method for quantitative dynamic contrast enhanced–MRI analysis. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2009;61(4):851-859.
11. Wu C, Wang N, Gaddam S, et al. Retrospective quantification of clinical abdominal DCE-MRI using pharmacokinetics-informed deep learning: a proof-of-concept study. Frontiers in Radiology. 2023;3.
12. Wu C, Wang L, Wang N, et al. Retrospective Quantification Pharmacokinetics Of Clinical Breast DCE-MRI Using Deep Learning. ISMRM 2023. 2023;3071.
13. Saha A, Harowicz MR, Grimm LJ, et al. A machine learning approach to radiogenomics of breast cancer: a study of 922 subjects and 529 DCE-MRI features. British journal of cancer. 2018;119(4):508-516.
14. Avants BB, Tustison NJ, Song G, Cook PA, Klein A, Gee JC. A reproducible evaluation of ANTs similarity metric performance in brain image registration. Neuroimage. 2011;54(3):2033-2044.
Figures
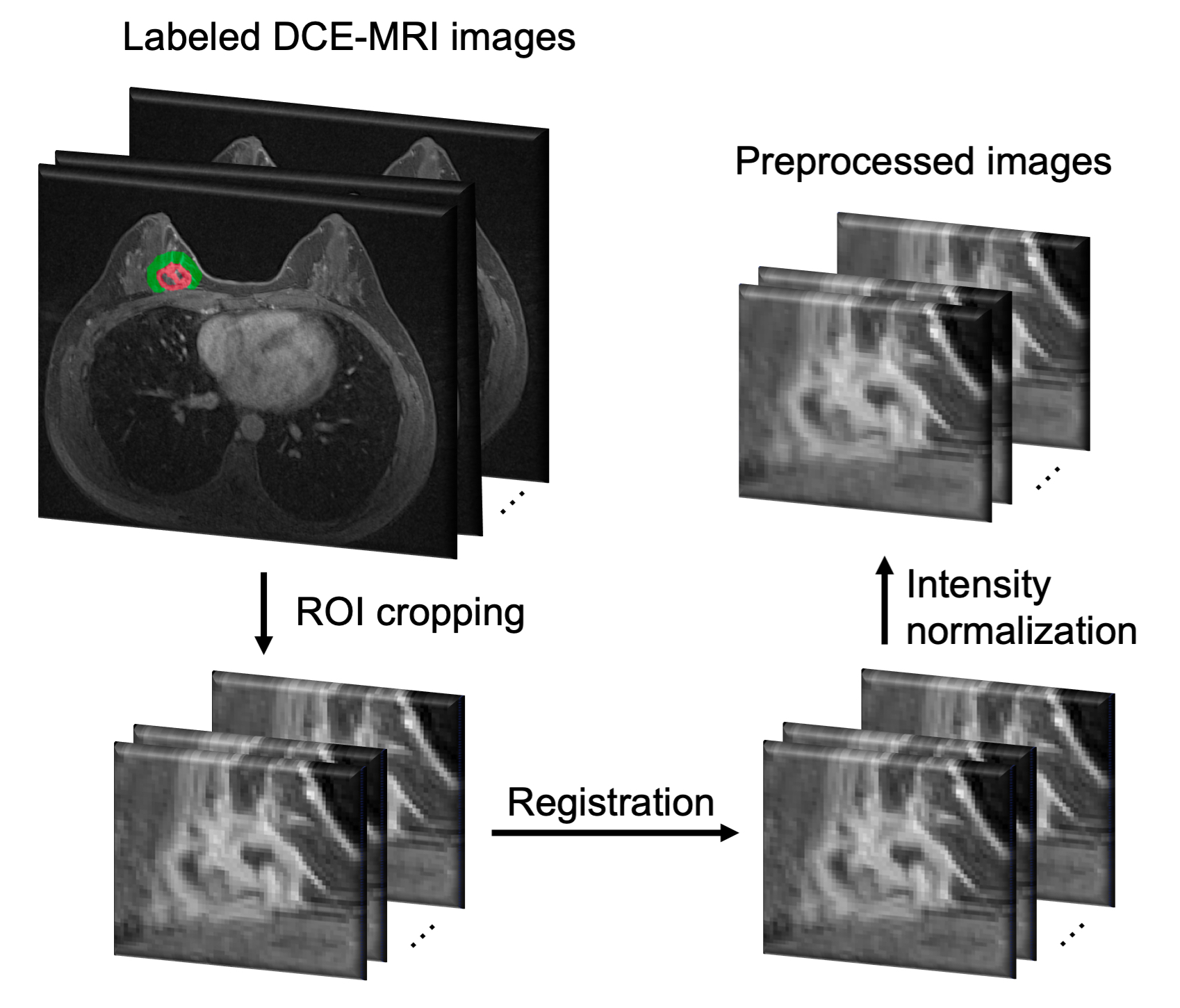
Figure 1 Image preprocessing pipeline. The DCE-MRI images labeled by an experienced radiologist was first cropped to centralize tumor, then performed ANTs registration, and intensity normalized.

Figure 2 Retrospective pharmacokinetic quantification pipeline. The multi-phasic data was temporally super-resolved, then curve analysis was performed to get semi-quantitative maps, and pre-trained transformer block was used to generated quantitative maps.
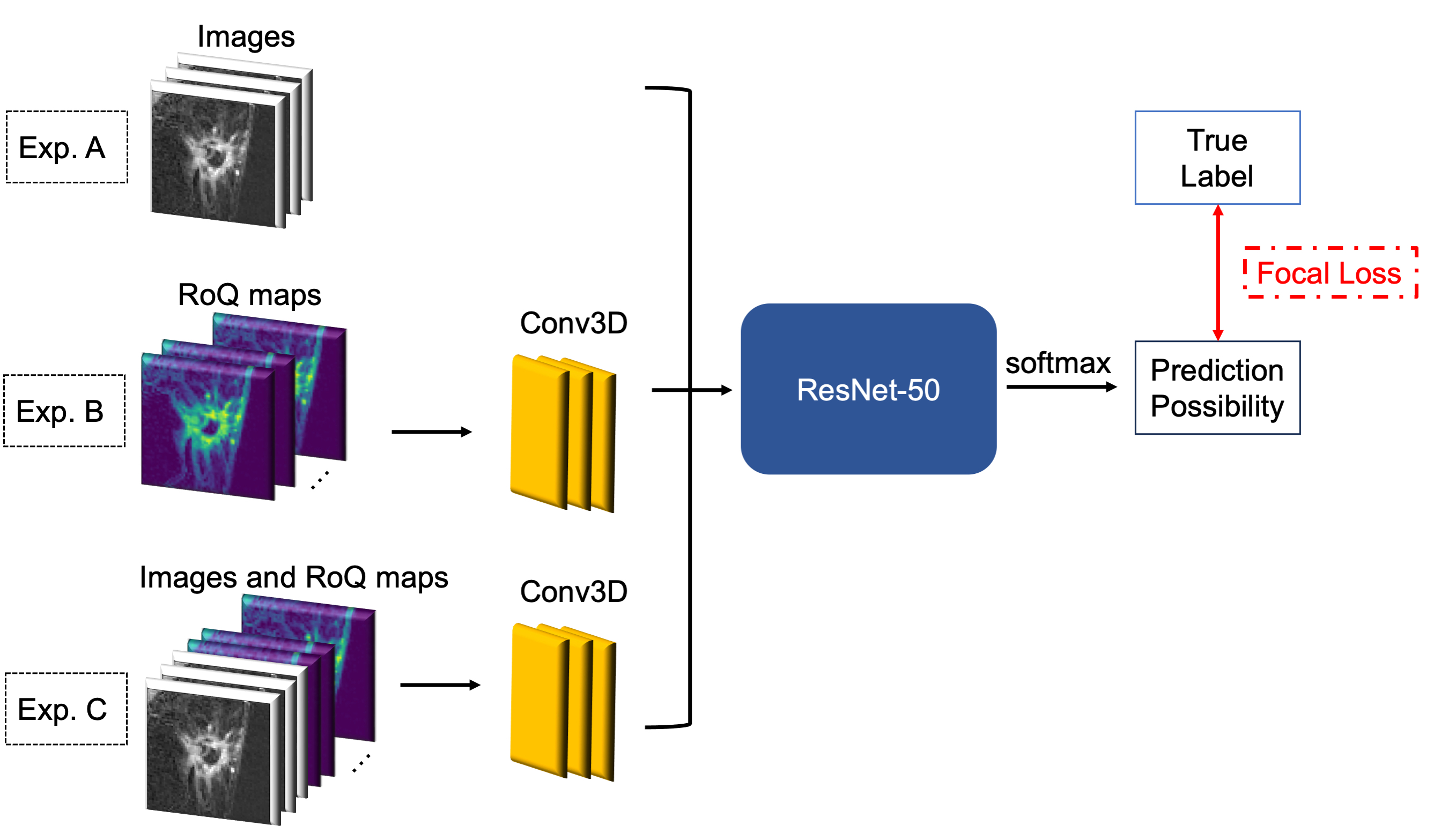
Figure 3 Network and experiment settings of proposed method. The ResNet-50 takes images (experiment A), RoQ maps (experiment B),or the concatenation of images and RoQ maps (experiment C) as input, and outputs a prediction probability, with which focal loss will be calculated.
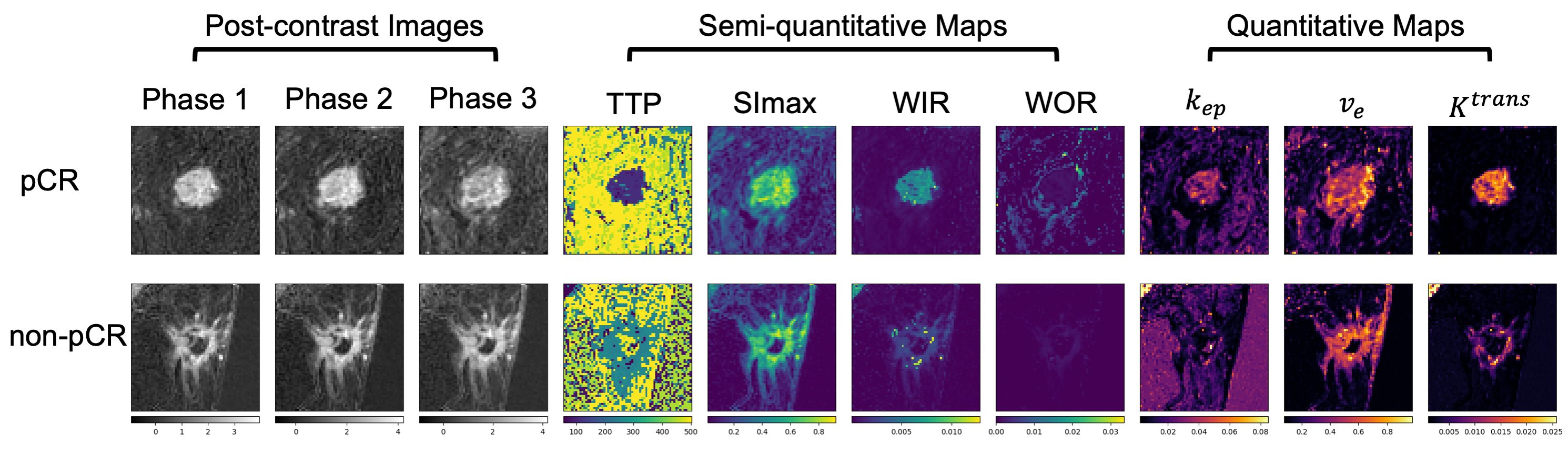
Figure 4 Example of images and retrospective pharmacokinetic maps from a pCR patient and a non-pCR patient.
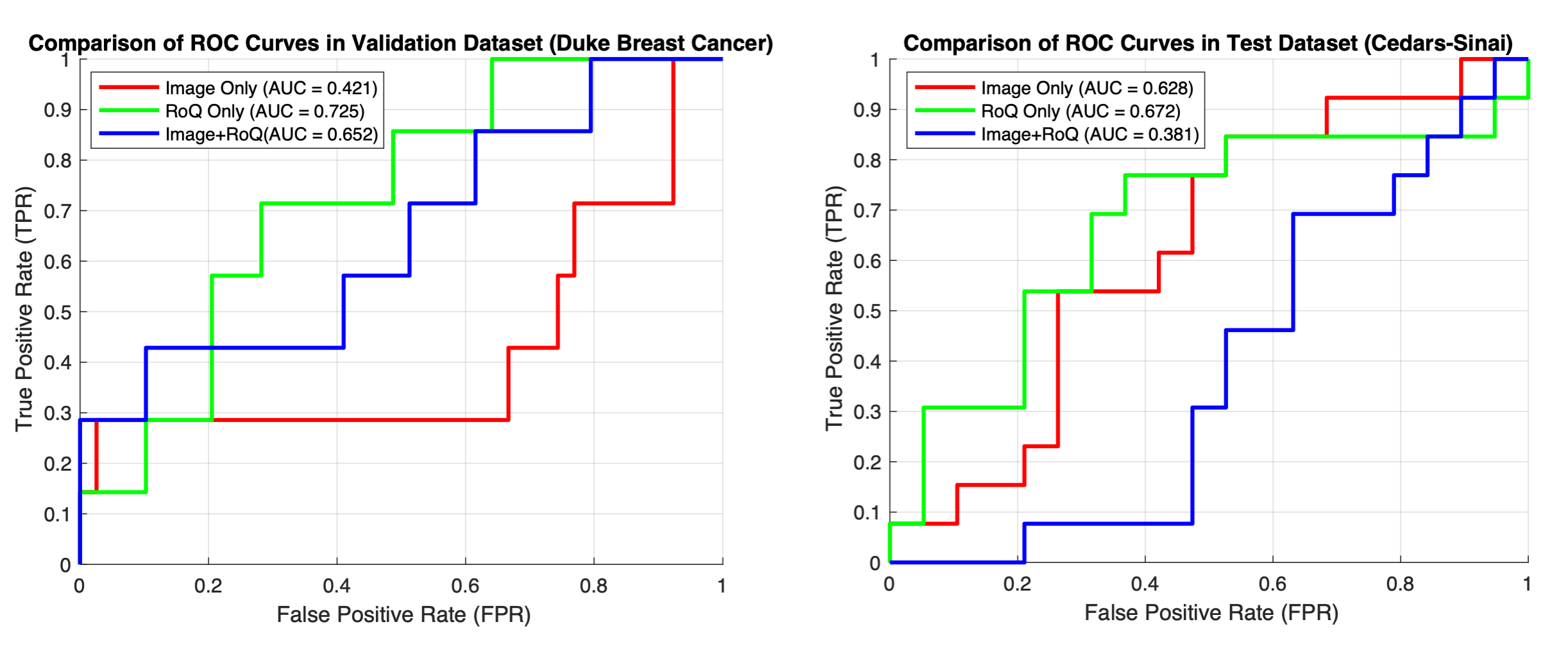
Figure 5 ROC curves in the validation dataset (left) and in the external test dataset (right).