2108
Nipple detection in breast dynamic contrast-enhanced magnetic resonance imaging using reinforcement learning1Research and Innovation Department, Olea Medical, La Ciotat, France
Synopsis
Keywords: Analysis/Processing, Breast, Nipple, Detection, Landmark
Motivation: As the nipple position knowledge becomes part of standardized report, the automatic detection can ease clinician’s workflow.
Goal(s): The aim of our work is to accurately detect the position of the nipples in a dynamic contrast-enhanced (DCE) MR image.
Approach: A reinforcement learning approach combined with a multi-constructor and multi-centric database enabled to initiate the development of a versatile tool in line with clinical real life. The detection problem was addressed using a Deep Q-Network trained with 248 breast DCE MR images.
Results: The nipple positioning error is less than 10 millimeters in most of the breasts tested, i.e. 95/102 breasts.
Impact: Nipple detection is a tedious task for clinicians and an arduous one for algorithms. Lesion to nipple distance is valuable information when planning surgery. This study explores the landmark detection domain to automate nipple detection using a reinforcement learning approach.
Introduction
The nipple to lesion location is valuable information when planning biopsy1 or resection surgery2 as it helps to decide wheter a nipple-areola sparing mastectomy is feasible. Among automatic tasks that can streamline the radiological interpretation process, such as lesions segmentation, nipple detection is another subject of interest for clinicians. Therefore, including the distance between the nipple and the lesion in a findings report would benefit clinical workflow. This detection is complicated as breasts can differ greatly from one another, resulting in very different nipple shapes and positions, which can be even more deformed by the coil, or by neoplasm incidence. In addition, breast MRIs are performed to highlight internal tissues rather than the skin, and can have a broad range of contrasts, making the nipple detection task challenging. This study explores a new method to detect the nipple on breast MR images thanks to reinforcement learning.Methods
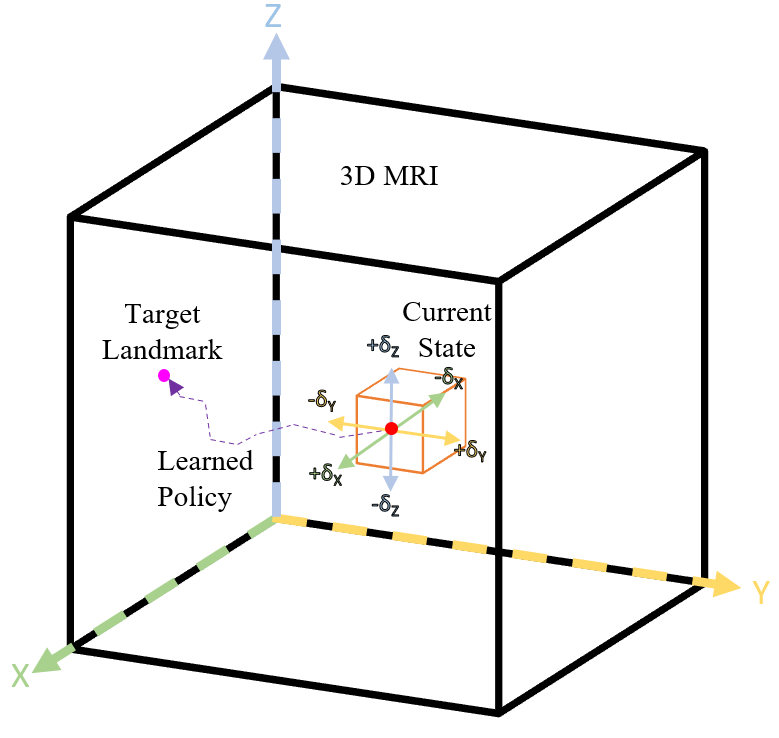
Reinforcement learningReinforcement learning (RL) is a training method based on rewarding desired behaviors and/or penalizing undesired ones3. In general, a reinforcement learning agent perceives and interprets its environment, takes actions, and learns through trial and error. A diagram representing RL agent finding a target landmark4 is represented in Figure 1. The agent is first spawned randomly within the boundaries of the 3D image. Then it iteratively moves toward a nipple position (x,y,z) within an MR volume. Its movement is decided using a Deep Q-Network (DQN): given a current state (e.g., position, surroundings information), the network predicts a movement that should reduce its distance to a nipple. Our implementation is based on the constrained multi-agent reinforcement learning5.
Data preparation
The database consists of 124 studies coming from more than 15 different imaging centers and includes 4 MRI system manufacturers (59% GE, 17% Siemens, 17% Philips, 7% Canon). Studies were acquired following the standard protocol with both 1.5 T (84%) and 3T (16%) magnetic fields. The nipple detection study was performed on T1w dynamic contrast enhanced (DCE) MR series and using the first post-contrast phase. Also, two-thirds of the data is fat saturated, and one-third is non-fat saturated. The database was randomly split into three sets for training (148), evaluation (49), and testing (51) purposes.
The manual annotation was done by three experts, and the nipple area was annotated using 3D sphere brush tool. Unlike segmentation annotation, the knowledge of the nipple spatial extend is not required here. Instead, a point coordinate is needed, and it was obtained as the centroid coordinates of the previous annotation.
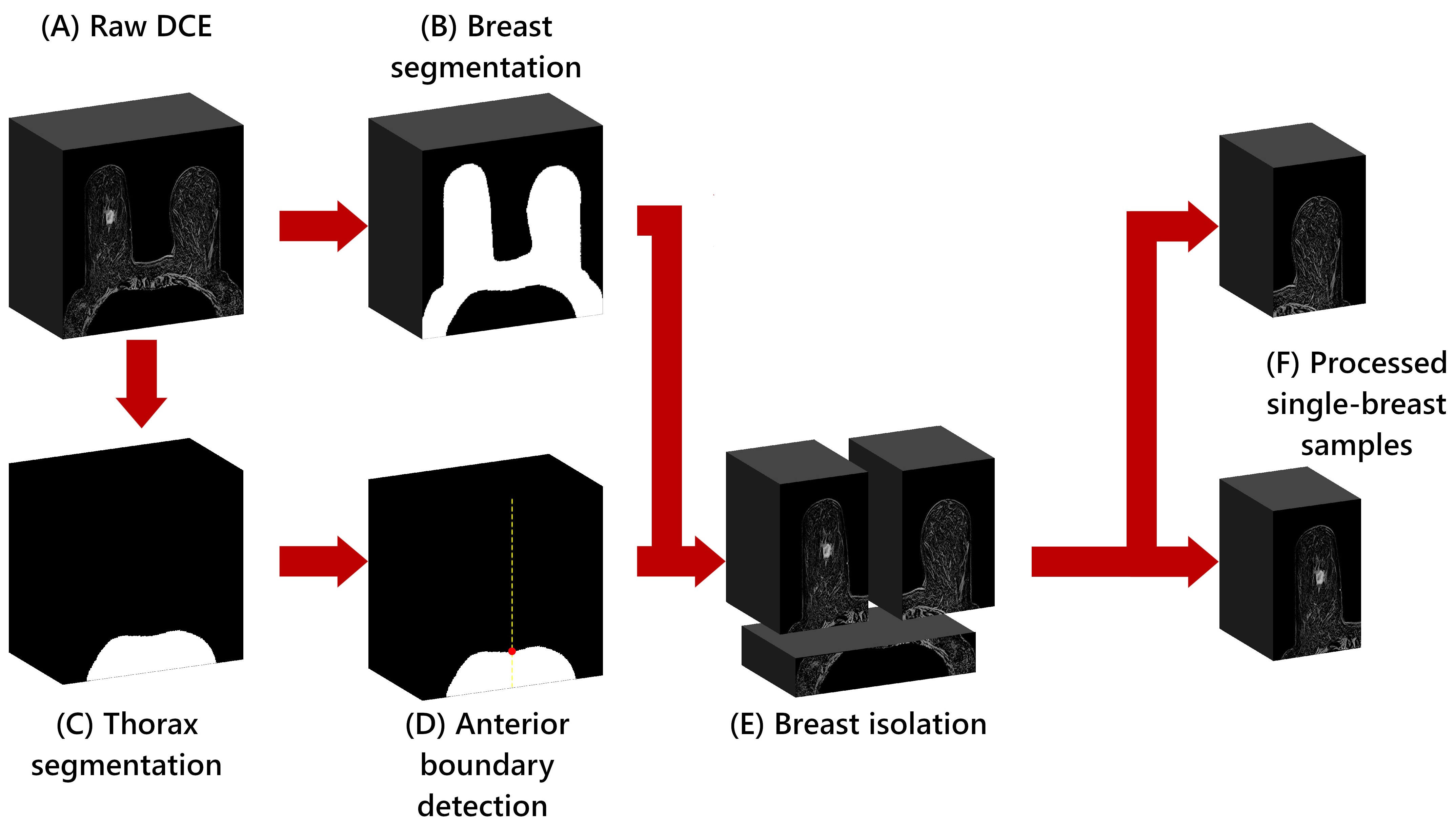
In this study, only one breast is analyzed at a time. A dedicated segmentation model provides the breast and thorax masks that can be used to extract each breast, as detailed in Figure 2.
Results
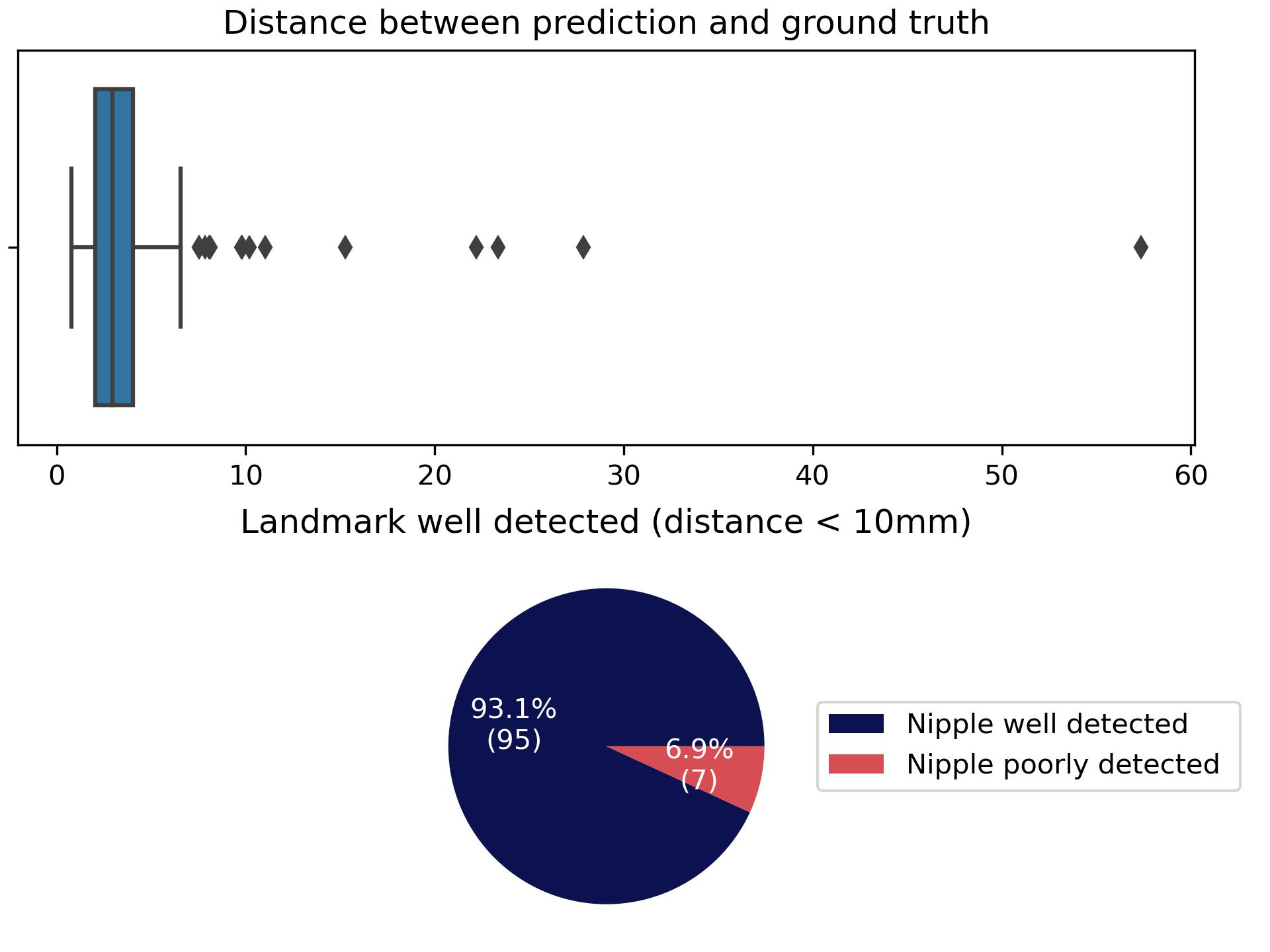
The database is artificially doubled because the breasts are considered separately. This option provides additional diversity compared with the original dataset, since the two breasts are not symmetrical. After the training process, 102 breast volumes were used to test the resulting model. The error quantification was determined by the distance from ground truth to estimation coordinates. The success criterion is established when this distance remains less than 10 mm. Overall, the trained model succeeded in 93% of cases, i.e. 95/102 breasts. Figure 3 presents the statistics obtained with the test dataset. Also, Figure 4 shows some representative examples of prediction compared to the ground truth.Discussion
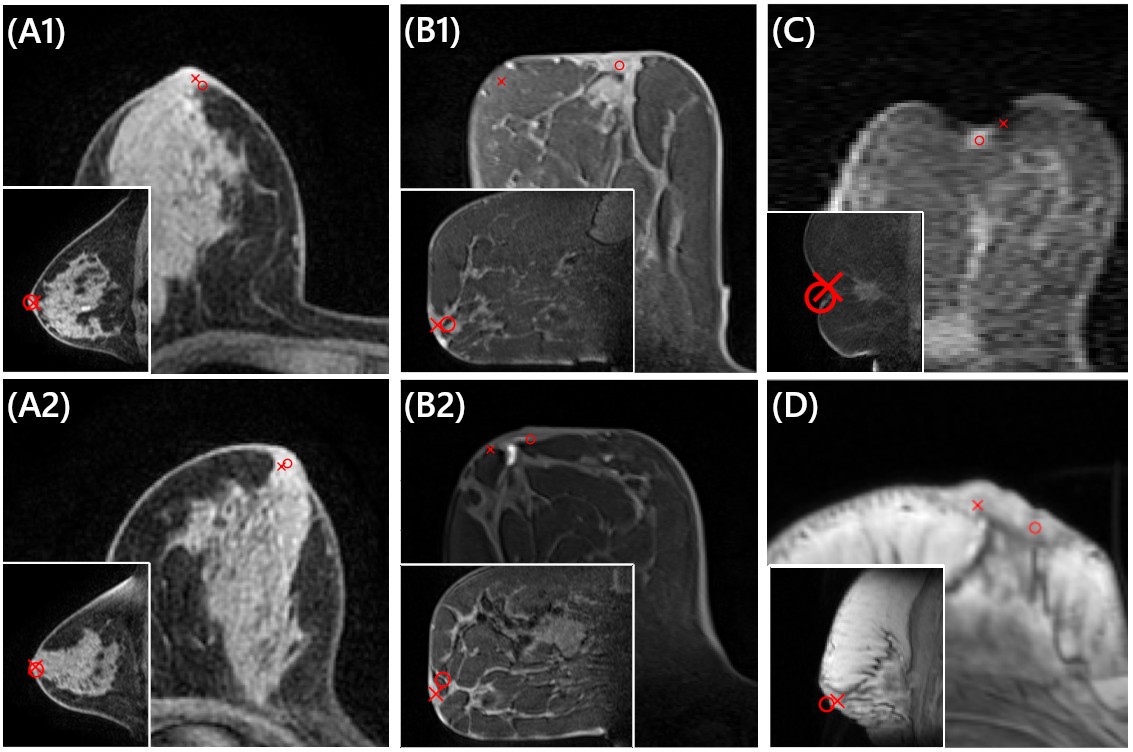
This study assumed that the nipple is anatomically invariant, as breast landmark, even though it differs in shape and size from one patient to another. Results in Figure 4A underline the overall quality of the model prediction using the deep RL strategy. In Figure 4B, a square-shaped breast illustrates the worst prediction with 57 mm off. A nipple depression is presented in Figure 4C, which poses detection challenges. A non-fat saturated acquisition is shown in Figure 4D, where the agent encounters difficulty in nipple detection. While overall performances are satisfactory (93% of sucess), outliers’ results will be further mitigated with database compensation regarding under-represented breast features. Finally, distance to the ground truth might not be enough to decide when the nipple is properly detected, and a visual inspection may be considered to statute. To date, no other study has reported nipple detection performance in this context.Conclusion
Nipple detection is challenging due to anatomical variability of the breast and the nuances observed in MRI protocols. This automated approach based on reinforcement learning demonstrated the feasibility of this task for computer aided diagnosis tool. This work will contribute to flow the MRI exams analysis and standardize report for improved patient care.Acknowledgements
No acknowledgement found.References
1 - Zhang, J. et al., "Hierarchical Convolutional Neural Networks for Segmentation of Breast Tumors in MRI With Application to Radiogenomics," in IEEE Transactions on Medical Imaging, vol. 38, no. 2, pp. 435-447, Feb. 2019.
2 - D’Alonzo, M. et al., “Clinical and radiological predictors of nipple-areola complex involvement in breast cancer patients,” Eur J Cancer, vol. 48, no. 15, pp. 2311–2318, Oct. 2012.
3 - Kevin Zhou, S. et al., "Deep reinforcement learning in medical imaging: A literature review," Medical Image Analysis, Volume 73, 2021.
4 - Alansary, A. et al., “Evaluating reinforcement learning agents for anatomical landmark detection,” Med Image Anal, vol. 53, pp. 156–164, Apr. 2019.
5 - Leroy, G. et al., "Communicative Reinforcement Learning Agents for Landmark Detection in Brain Images." In: Kia, S.M., et al. "Machine Learning in Clinical Neuroimaging and Radiogenomics in Neuro-oncology". MLCN RNO-AI 2020 2020. Lecture Notes in Computer Science(), vol 12449. Springer, Cham., 2020.
Figures