2107
Automatic spine station identification from surface coil sensitivity maps of MR imaging using deep learning1GE HealthCare, Niskayuna, NY, United States, 2GE HealthCare, Waukesha, WI, United States, 3GE HealthCare, Bangalore, India
Synopsis
Keywords: Analysis/Processing, Segmentation, Spine stations; Automatic prescription
Motivation: In spine scanning with MRI, multiple localizer scans are acquired to manually set the stations. 3D surface coil sensitivity maps, with low-resolution but large FOV, which are acquired as part of the prescan can potentially be used to automatically determine the station boundaries.
Goal(s): Utilize the existing information in the MRI scanner to automatically predict the location of spine stations and thereby accelerate the workflow.
Approach: Use a deep learning framework to automatically identify the stations of the spine anatomy from the coil sensitivity maps.
Results: The deep learning model shows good localization of spine stations with mean centroid errors less than 15mm.
Impact: Spine stations can be identified from large FOV, low-resolution surface coil sensitivity maps in MRIs using our deep learning framework, which can be used for fast and automatic spine anatomical planning and imaging.
Introduction
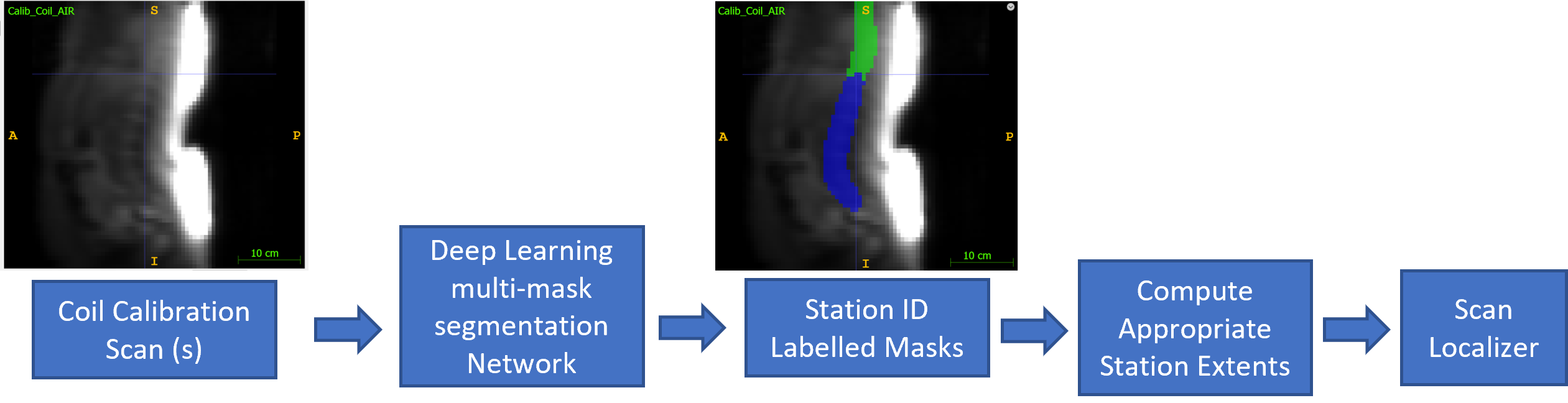
Spine scanning with MRI is cumbersome because it involves multiple stations, including cervical, thoracic and lumbar stations. The technologist has to acquire multiple localizers and then work across the multiple set of localizers to determine the boundaries across stations and scan higher resolution images accordingly. This might also involve additional processing in terms of image pasting etc. Previously, a methodology for automatic prescription of correctly oriented FOV and coverage for spine localizer imaging using large FOV, low-resolution 3D surface coil sensitivity maps (calibration data) has been demonstrated1. We extended this concept to determine the extent of three spine stations automatically and accordingly generate correctly positioned station wise localizer data with relevant orientation, FOV and coverage. This whole setup runs from the prescan data itself and provides ready to use, station-based localizer data for further spine MR scan planning. Figure 1 shows the proposed workflow for automatic prescription of spine exams based on calibration data.Methods
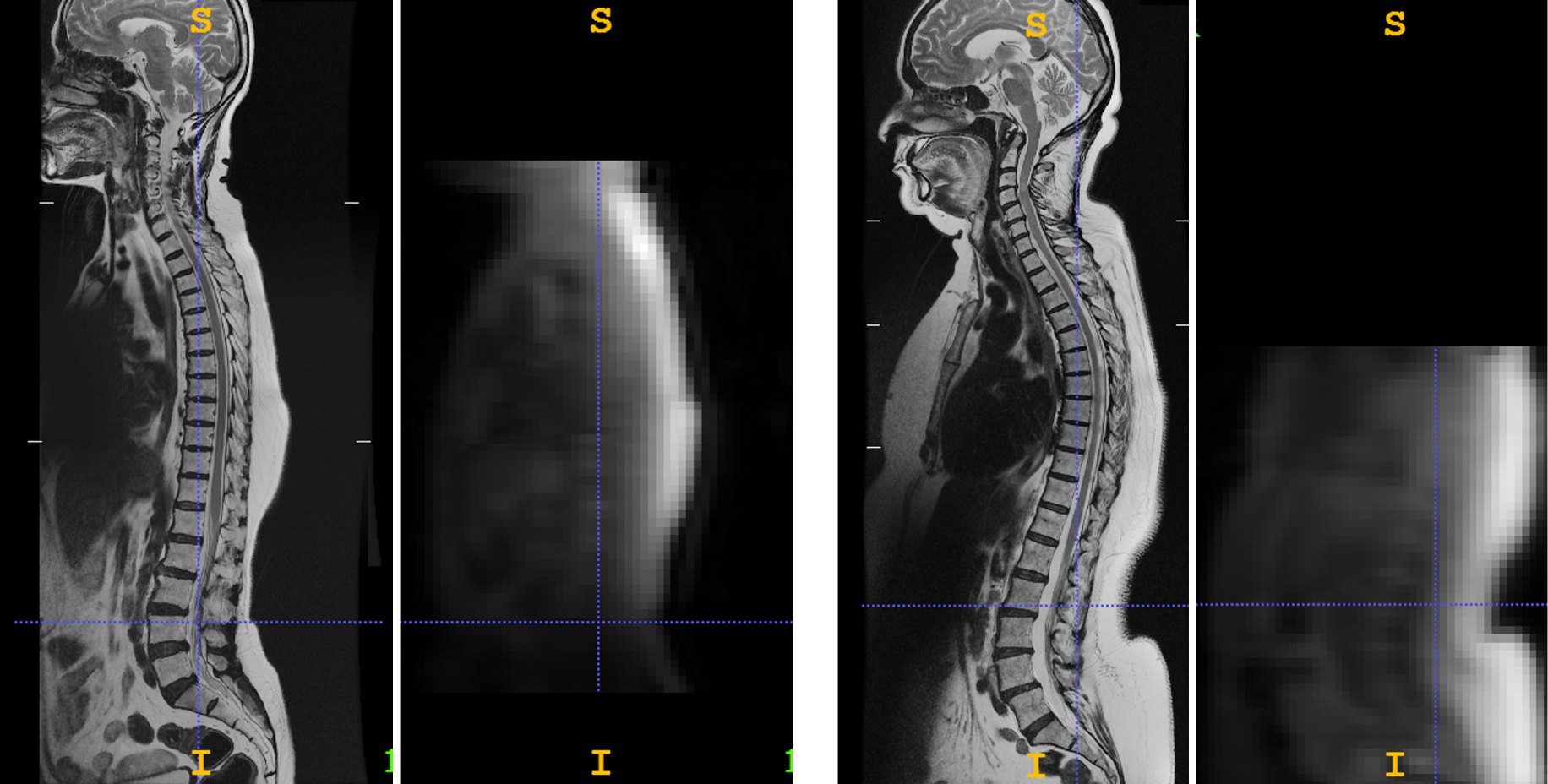
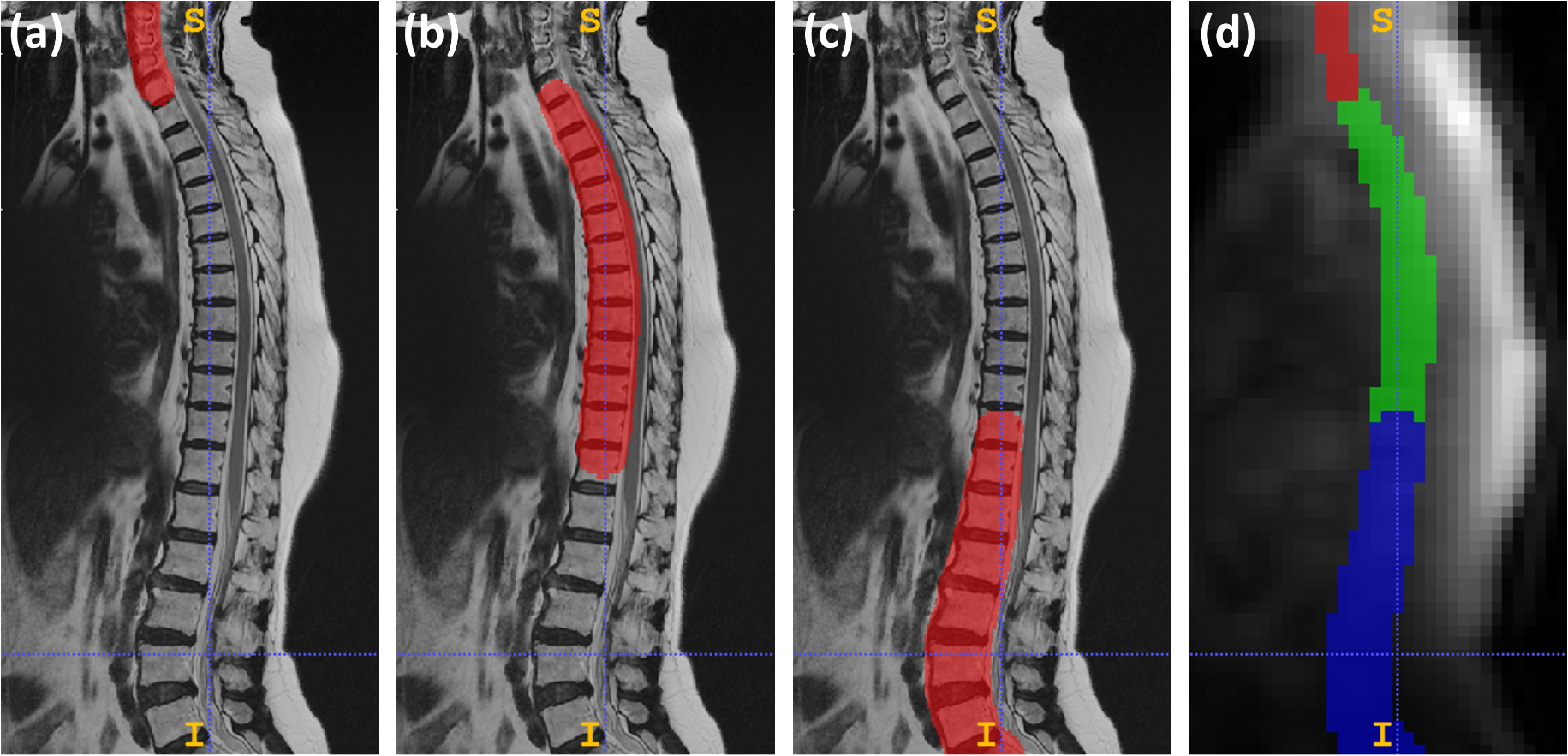
Data: A total of 90 patients spine MRI data with coil sensitivity maps and high-resolution T2 scans were collected on 1.5T MRI scanner. Data were acquired with the following protocol: Coil sensitivity maps: TE/TR=1.5ms/200ms, flip angle=70°, in-plane resolution of 6.25x6.25mm and slice thickness of 7mm. High-resolution 2D sagittal T2: TE/TR=115ms/2200ms, flip angle=90°, in-plane resolution of 0.53x0.53mm and slice thickness of 4.5mm. High-resolution images were acquired for three stations of spine with an overlapping FOV in the original acquisition by 15%. From the Image browser, the pasting session application was used to combine the stations and created a series labeled as PASTED. See Figure 2 for examples of pasted series and calibration images.Ground-truth (GT) generation: High-resolution sagittal pasted series data was used to generate vertebral column mask, and cervical and lumbar station labels using existing DL frameworks2. The vertebral column mask and the cervical and lumbar labels were used to get the segregation of the three stations in the high-resolution pasted images. These segregation masks were processed to obtain smooth concave masks enclosing each station, which were resampled to calibration data space and generated the final GT multi-station masks for training the DL model. All the calibration images were resampled to 64x64x64 image size before training. See Figure 3 for an example of GT generation.
DL architecture and training: We used a 3D U-Net3 architecture with three downsample and upsample levels. The initial filter number is 16 and convolutional kernel size is 3x3x3. The whole dataset was split into train (191 with augmentation), validation (20 with augmentation), and test-set (32 images) such that all data from each patient appeared only in one split. The DL model was trained for 100 epochs with multi-label DICE as loss function.
Evaluation: We use the following metrics to evaluate the performance of the spine station localization: Euclidean distance between the centroid points of GT and predicted masks, and distance between the boundaries of GT and predicted masks in AP/SI directions.
Results and Discussion
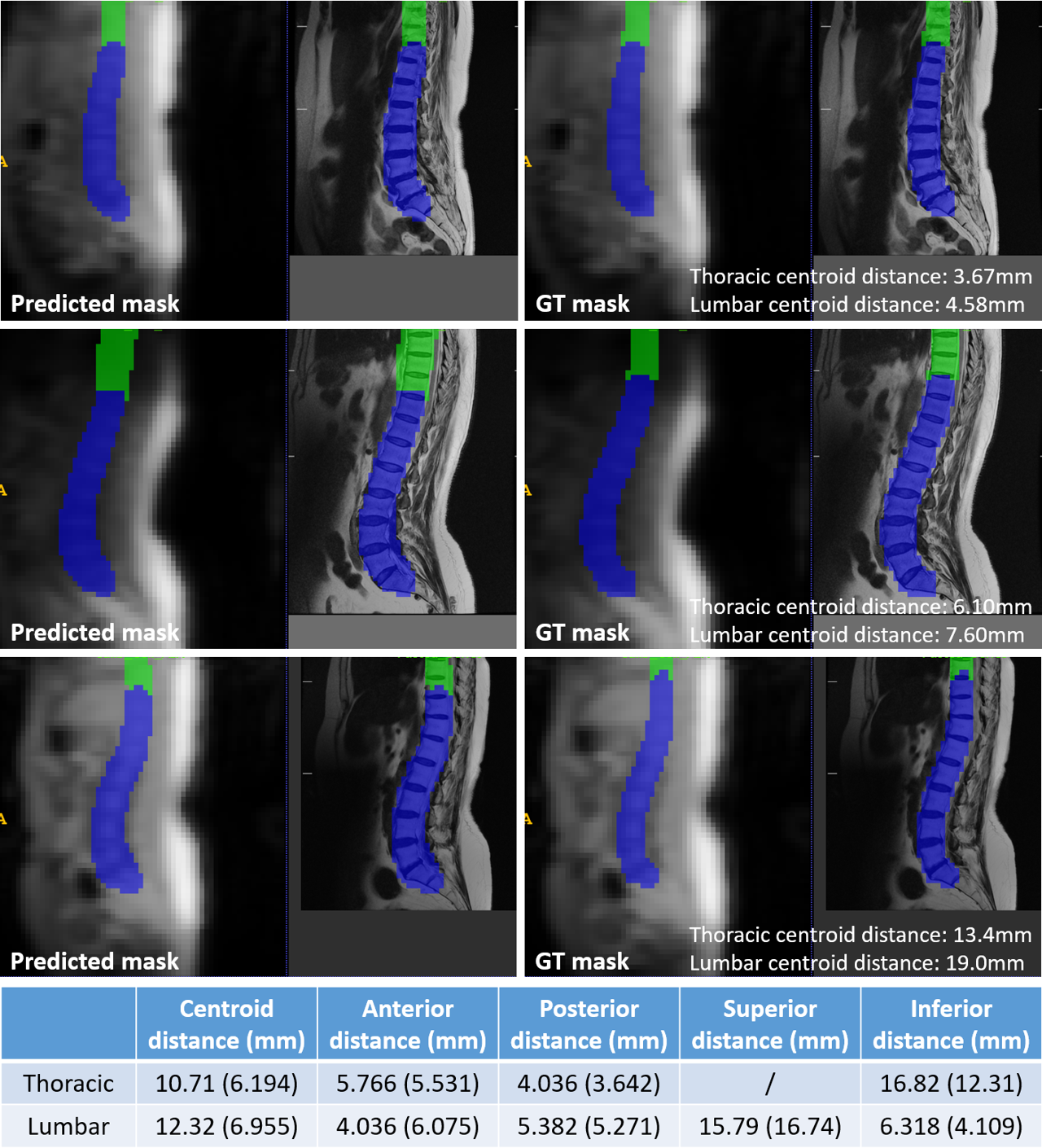
Figure 4 shows examples of DL model predictions on testing images from different subjects. The DL model produces consistent results compared to GT masks, indicating its capability of identifying spine stations from calibration images. The centroid distance between predicted and GT masks has mean of 10.71mm for thoracic and 12.32mm for lumbar station among the testing data, with maximum distance less than 25mm, which is within acceptable limits for localization of spine stations (a single spine vertebrae is ~20-24 mm along SI direction). The distance errors in the A/P directions are mostly less than 10mm. Shift in SI direction is less than 30mm in most cases, which should be acceptable to automatically identify the spine stations as part of the prescan to reduce repeated localizer scans.The current approach is limited by a small training set. Not all of the coil sensitivity maps were saved after scanning, resulting in a limited number of calibration data for cervical station in our dataset. Therefore, results on cervical station and the distance along superior direction of the thoracic station are not presented. In the future, we will expand our data pool to include more subjects with all stations from different sites, which will make the model more robust to different FOVs and scanning parameters.
Conclusion
We have demonstrated that the large FOV, low-resolution calibration data can be used by a DL framework to identify the spine stations for spine exam, which can reduce the repeated scans of localizers in clinical practice. The concept of our DL framework is generic and can be extended to other anatomies which need station identification.Acknowledgements
No acknowledgement found.References
[1] Manickam, Kavitha, et al. Intelligent automatic slice prescription of scout scans of MSK MRI imaging using surface coil sensitivities. International Society for Magnetic Resonance in Medicine (ISMRM) 2023, Toronto, Canada, June 3-8, 2023 (p.1445).
[2] Shanbhag, Dattesh D, et al. Deep Learning based spine labeling with three-plane 2D localizers without vertebrae segmentation. International Society for Magnetic Resonance in Medicine (ISMRM) 2021, May 15-20, 2021 (p.3812).
[3] Çiçek, Özgün, et al. 3D U-Net: learning dense volumetric segmentation from sparse annotation. Medical Image Computing and Computer-Assisted Intervention–MICCAI 2016: 19th International Conference, Athens, Greece, October 17-21, 2016, Proceedings, Part II 19. Springer International Publishing, 2016.
Figures