2106
Feasibility of predicting MRI tissue heating (MRSaiFE) using experimental training data1Radiology, Weill Cornell Medicine, New York, NY, United States, 2GE Healthcare, Aurora, OH, United States
Synopsis
Keywords: Analysis/Processing, Safety, SAR, MRSaiFE
Motivation: MRI poses safety risks due to tissue damage via SAR hotspots. We have previously developed MRSaiFE, an AI-based SAR prediction tool.
Goal(s): This study expands MRSaiFE with experimental, in vivo, training data.
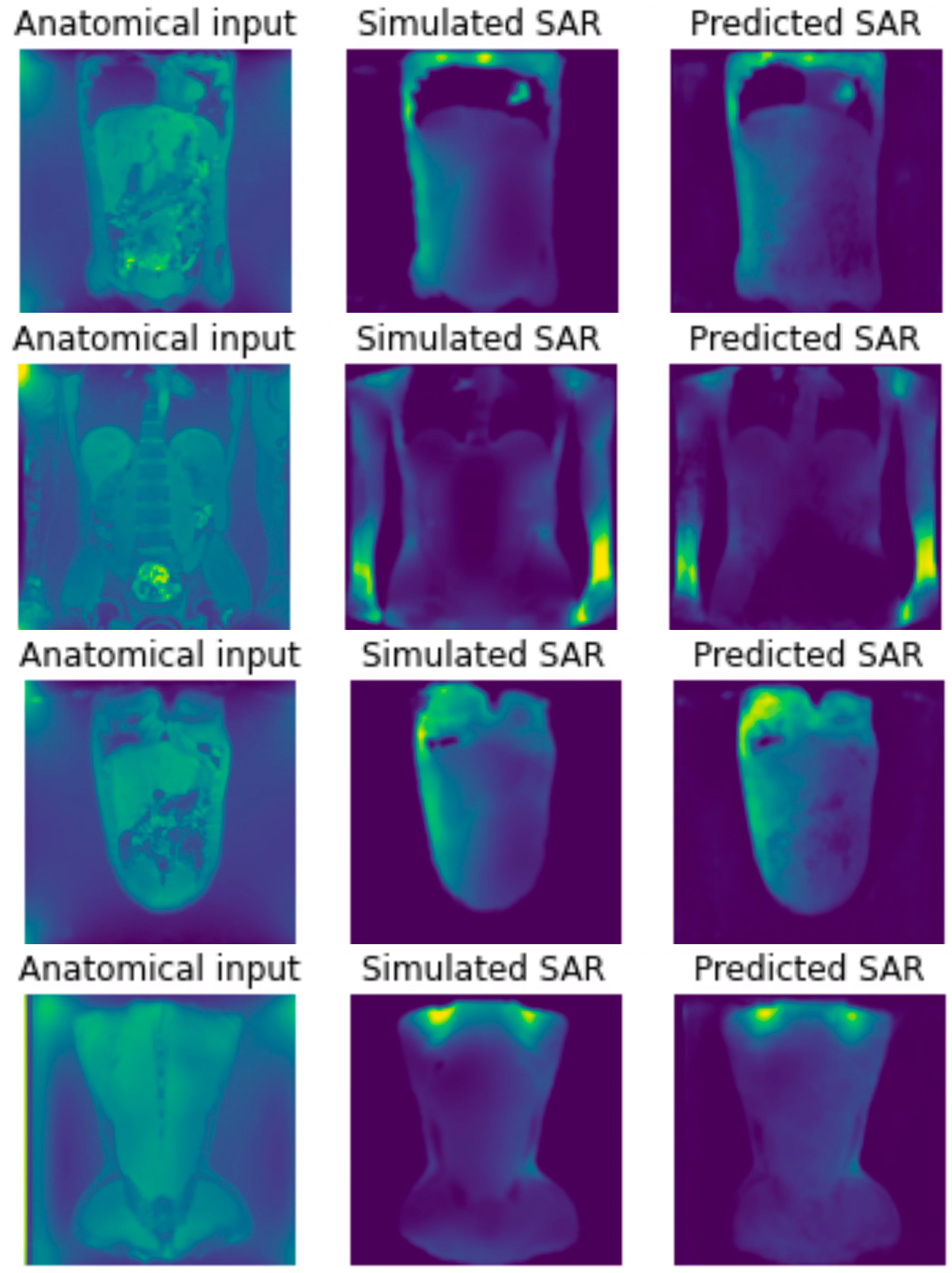
Approach: Images from a subject are segmented into a numerical model that is simulated to obtain SAR. The MRSaiFE input is the scanned image, and the predicted output SAR is obtained from training on the simulated SAR.
Results: Good agreement (0.4% MSE, 6% RMSE, and 81% SSIM) demonstrates feasibility of using 1) experimental training data and 2) scanned input images, enabling future prediction from in vivo localizers.
Impact: By replacing conservative SAR margins with patient-specific values, MRSaiFE offers potential for enhanced sensitivity, resolution, or reduced scan time. Additionally, it could notably enhance safety in patients with medical implants, hyperthermia treatments, and in MRI procedures at ultra-high fields.
Introduction
Localized tissue heating in MRI, measured as the specific absorption rate (SAR), results in “hot spots” in regions of excessive radiofrequency (RF) energy absorption. Local SAR cannot be measured, and current monitoring methods do not reflect individual patient anatomy, often leading to conservative estimates that limit MRI power and performance1,2.Local SAR varies widely and is strongly influenced by patient anatomy, positioning, and coil specifics. Consequently, there is a growing need for a real-time monitoring system7,8. We have previously introduced MRSaiFE9-13, an AI-driven strategy devised to predict local SAR.
Here, we expand MRSaiFE by introducing experimental data. The original algorithm was trained on numerical body models, using mockup input images and a simulated SAR output.
In this study, abdominal data from a 22-year-old male subject was used. The MRSaiFE algorithm now uses a scanned input image. SAR cannot be measured in vivo and was obtained from segmenting the image data into a numerical model that was then simulated.
Methods
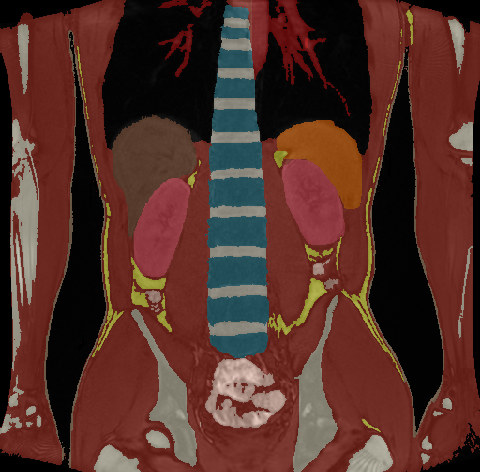
A. Data AcquisitionSegmentation: Abdominal 3D LAVA Flex images of a 22-year-old male were obtained on a GE MR750 system (Fig.1). The DICOM data were segmented with iSEG (Zurich MedTech, Zurich, Switzerland) to form a numerical body model. A threshold mask of the whole body was obtained. This threshold level was then manipulated to segment each tissue individually. 13 different tissues were obtained (muscle, skin, fat, internal air, blood vessels, bone, intestines, liver, muscle, spinal cord, spleen, vertebrae, kidneys, and heart). The brush tool was used to refine the edges of each tissue. An example of segmented human body is shown in Fig.2.
Simulation: Sim4Life was used for a full-wave simulation of the segmented body model within a standard 60cm-bore 3T body-sized birdcage coil. Each tissue was assigned dielectric tissue properties (IT’IS, Switzerland). To account for SAR variations due to patient positioning, we simulated the model at positions of ±x=40cm and ±y=40cm from the isocenter. The simulated B1+-field (normalized to 1W input power) and 1g-averaged SAR were extracted for further processing.
B. Post-processing:
Matlab was used to postprocess the measured in vivo data, simulated SAR and B1 fields. The acquired 3D image (input) and simulated SAR (output) data were co-registered. Coronal image slices were multiplied with the simulated B1+-field of the empty birdcage coil to encode the location of the model. AI-training data were exported as 224x224 images, resulting in 8,184 image input and SAR output images, split into 75%/15%/10% training/validation/testing datasets.
C. AI Network:
A 2D U-Net architecture was implemented using a cascade of convolutional filters with nonlinear reLU activation functions9-15. Training was performed using stochastic gradient descent (SGD) as well as Keras and Tensorflow (Google, Mountain View, California). Hyperparameters were maintained from the original MRSaiFE implementation with optional optimization as needed. Training was performed over 30 epochs SGD using a GeForce RTX 2080 Ti Graphics Processing Unit (GPU) (NVIDIA, Santa Clara, USA). Layers were randomly initialized using the He initialization.
D. Testing:
Quantitative image quality comparisons were performed between simulated and predicted SAR and quantified using mean squared error (MSE), root mean squared error (RMSE), and structural similarity (SSIM).
Results
Predicted images align well with the expected SAR (Table 1). We obtained an MSE of 0.4%±0.3% with an RMSE of 6%±2% over all slices in the test dataset. A structural similarity index (SSIM) of 81%±9% was observed.Discussion and Conclusion
This study introduces experimental data into our real-time local SAR-monitoring tool.Future work includes introducing experimental output data in addition to the experimental input data used here. SAR cannot be measured in vivo, but data in the form of B1 and/or temperature maps can be incorporated. In the course of this work, we performed preliminary scans of B1 and temperature maps and found agreement with the simulated data, to be analyzed in detail in future work.
We will also use segmented full-length body scans to expand the proof-of-concept abdominal study presented here. We plan to incorporate a number of such segmented models in the final tool instead of or in addition to the simulated dataset published previously.
This specific study focuses on body MRI at 3T, which comes with similar spatial SAR variation as 7T brain imaging. We are still in the process of installing our 7T scanner and will report on the higher field strength when available.
Beyond SAR monitoring in routine scans, MRSaiFE could notably enhance safety in patients with medical implants, hyperthermia treatments, and in MRI procedures at even higher fields like 9.4T and 10.5T.
Acknowledgements
This research work was supported by the National Institutes of Health (R01EB031820).References
- Collins, C.M., et al. (2005). Temperature and SAR calculations for a human head within volume and surface coils at 64 and 300 MHz. Journal of Magnetic Resonance Imaging, 19(5), 650-656.
- Hand, J.W. (2008). Modelling the interaction of electromagnetic fields (10 MHz–10 GHz) with the human body: methods and applications. Physics in Medicine & Biology, 53(16), R243.
- C. M. Collins and M. B. Smith, "Calculations of B1 distribution, SNR, and SAR for a surface coil adjacent to an anatomically-accurate human body model," Magn. Reson. Med., vol. 45, no. 4, pp. 692-699, Apr. 2001.
- M. Thornton, P. Picot, B. Rutt, and S. Winkler, "Method and system for estimating the specific absorption rate of a tissue region prior to a magnetic resonance imaging scan," US20150316626A1, Nov. 5, 2015.
- S. A. Winkler, P. A. Picot, M. M. Thornton, and B. K. Rutt, "Direct SA mapping by thermoacoustic imaging: A feasibility study," Magn. Reson. Med., vol.78, no. 4, p. 1599-1606, 2017.
- S. A. Winkler and B. K. Rutt, "Practical Methods for Improving B1+ Homogeneity in 3 Tesla Breast Imaging," J. Magn. Reson. Imaging JMRI, vol. 41, no. 4, pp. 992-999, Apr. 2015.
- Zanche, N.D., et al. (2008). Real-time RF power monitoring in MRI. Magnetic Resonance in Medicine, 59(2), 315-321.
- Katscher, U., et al. (2003). Transmitter B1 field inhomogeneities and SAR calculations for MRI with fast multichannel transmit arrays. Journal of Magnetic Resonance Imaging, 17(5), 546-556.
- Gokyar, S., Zhao, C., Ma, S. J., & Wang, D. J. J. (2023). Deep learning-based local SAR prediction using B1 maps and structural MRI of the head for parallel transmission at 7 T. Magnetic resonance in medicine, 90(6), 2524–2538. https://doi.org/10.1002/mrm.29797
- Winkler, S. A., Saniour, I., Chaudhari, A., Robb, F., & Vaughan, J. T. (2020, December). MRSaiFE: tissue heating prediction for MRI: a feasibility study. In 2020 IEEE MTT-S International Microwave Biomedical Conference (IMBioC) (pp. 1-3). IEEE.
- Gokyar, S., Saniour, I., Robb, F., Nghiem, A., Kainz, W., Chaudhari, A. S., & Winkler, S. MRSaiFE: towards the real-time prediction of SAR in 3T and 7T MR RF coils-a feasibility study with 10 body models.
- Gokyar, S., Robb, F. J., Kainz, W., Chaudhari, A., & Winkler, S. A. (2021). MRSaiFE: an AI-based approach towards the real-time prediction of specific absorption rate. IEEE Access, 9, 140824-140834.
- Moghadam MC, Panjwani N, Motovilova E, Zhang M, Robb F, Hoang A, Afrin T, Winkler S.A. (2023). Optimized model architecture and generalization for deep learning-based SAR prediction (MRSaiFE). ISMRM 2023
- Meliadò, E. F., Raaijmakers, A. J. E., Sbrizzi, A., Steensma, B. R., Maspero, M., Savenije, M. H. F., ... & van den Berg, C. A. T. (2020). A deep learning method for image‐based subject‐specific local SAR assessment. Magnetic resonance in medicine, 83(2), 695-711.
- Brink, W. M., Yousefi, S., Bhatnagar, P., Remis, R. F., Staring, M., & Webb, A. G. (2022). Personalized local SAR prediction for parallel transmit neuroimaging at 7T from a single T1‐weighted dataset. Magnetic resonance in medicine, 88(1), 464-475.
Figures