2093
Contrastive Learning with Multi-Contrast Constraints for Segmentation in Renal Magnetic Resonance Imaging1Medical Image And Data Analysis (MIDAS.lab), Department of Diagnostic and Interventional Radiology, University Hospital of Tuebingen, Tuebingen, Germany, 2Department of Radiology, Center for Advanced Imaging Innovation and Research (CAI2R), New York University Grossman School of Medicine, New York, NY, United States, 3Department of Diagnostic and Interventional Radiology, University Hospital of Tuebingen, Tuebingen, Germany, 4Department of Radiology, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Analysis/Processing, Segmentation, Reproducibility challenge, multi-parametric renal MRI, AI/ML Image segmentation, Kidney
Motivation: Supervised deep learning provides state-of-the-art medical image segmentation when large labeled images are accessible. However, manual segmentation suffers from prolonged delineation.
Goal(s): In response to the 2024 ISMRM Challenge “Repeat it With Me: Reproducibility Team Challenge”, we aim to show the effectiveness of contrastive learning to find suitable initialization for segmentation with limited annotation.
Approach: We use a multi-contrast contrastive loss guided by representational constraints to learn discriminating features within multi-parametric renal MR images and fine-tune the pretrained model on segmentation tasks.
Results: Our findings validate that pretraining diminishes the needed annotation effort by 60% for different imaging sequences and enhances segmentation performance.
Impact: Multi-contrast contrastive learning reduces annotation effort to train deep-learning segmentation models, confirming prior findings in a new cohort, within the 2024 ISMRM Challenge “Repeat it With Me: Reproducibility Team Challenge” and indicating its potential to improve multi-parametric imaging workflows.
Introduction
Multi-parametric renal MRI is a promising tool for the assessment and monitoring of structural and hemodynamic changes associated with kidney diseases1,2. Generalizable image segmentation frameworks are required to assist clinical diagnostics and establish standardized data analysis workflows in the clinical routine. Deep learning methods have proved effective in handling multi-parametric datasets3–5 and have been applied for the segmentation of kidneys6–8. Nevertheless, collecting large annotated datasets to train such models remains a considerable challenge due to prolonged delineation and reproducibility issues. Self-supervised pretraining has been proposed to overcome the scarcity of labeled data and improve accuracy without direct knowledge of the subsequent downstream task9,10. In this study, we apply a contrastive loss with multi-contrast constraints for pretraining on multi-parametric renal MRI to reproduce previously published findings11 in a new cohort as part of the 2024 ISMRM Challenge “Repeat it With Me: Reproducibility Team Challenge”. By leveraging representational constraints derived from multi-parametric MR images, the model learns discriminative local representations with similar underlying tissue characteristics. We demonstrate the applicability of the method to reduce the annotation effort and improve segmentation performance. We also assessed the method’s generalizability for different contrast images.Methods
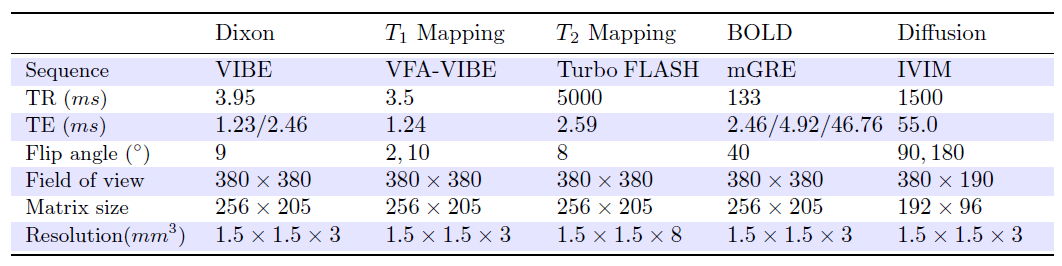
The multi-contrast contrastive loss: The used contrastive loss11,12 assumes that local regions within an MR image with similar tissue-specific parameters generate similar features in the learned representational space. First, a pixel-wise principal component (PC) analysis is performed, followed by K-means clustering to generate the constraint maps. These maps identify similar local regions that will be later used as a surrogate for tissue-specific information. During training, each patch within the image is pulled closer with concurrently similar patches in the learned feature space and in the constraint maps based on l2-normalized cosine similarity measures, whereas dissimilar samples are pushed apart.Data: We used 79 multi-parametric (Dixon, T1 Mapping, T2 Mapping, BOLD and diffusion) renal MR scans (59 patients with prostate cancer or neuroendocrine tumors and 20 healthy subjects), acquired in-house on a 3T scanner, as stated in Table 1. For training and testing, subjects were split into separate training/validation/test subsets of 58/6/15 subjects. Images were intensity normalized to values between 0 and 1. Clinicians manually annotated all data for quantitative evaluation.
Pretraining: A 2D encoder-decoder architecture is used11,12. Initially, the encoder undergoes training using a conventional contrastive strategy13 for 10 epochs. Then, the model is trained using the multi-contrast contrastive loss11,12. Training is conducted on an NVIDIA V100 GPU with an Adam optimizer (batch size=16, learning rate=1e−4, epochs=150) with the learning rate reducing by half if the contrastive loss on the validation dataset plateaus for 10 epochs. We pretrained the model on all available training subjects (N=58) using the studied contrast images. At this stage, learned representations embed relevant contrast information that can be used as an initialization for a subsequent segmentation task.
Downstream Segmentation Task: We fine-tuned the model on a limited amount of training subjects (N) ranging from 2 to 20 to investigate the performance in case of limited labeled data. As comparison, we fine-tuned on the entire training subset to study the effect of pretraining. We compared two models, trained with weights initialized using a random initialization (RI) and the investigated contrastive loss with multi-contrast constraints (CLC) on the multi-parametric data. Fine-tuning is conducted with the focal Tversky loss14 with an alpha weighting on each class on an NVIDIA V100 GPU with an Adam optimizer (batch size=20, learning rate=1e−3, epochs=200) with the learning rate reducing by half if the Tversky loss applied on the validation dataset plateaus for 10 epochs.
Results and Discussion
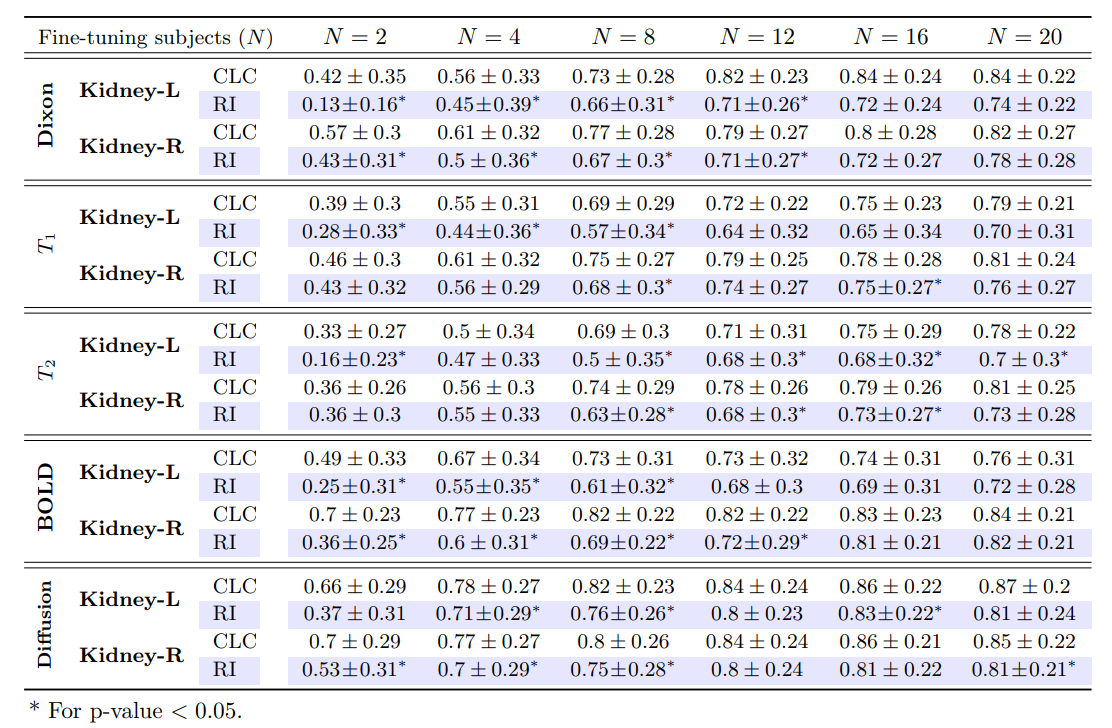
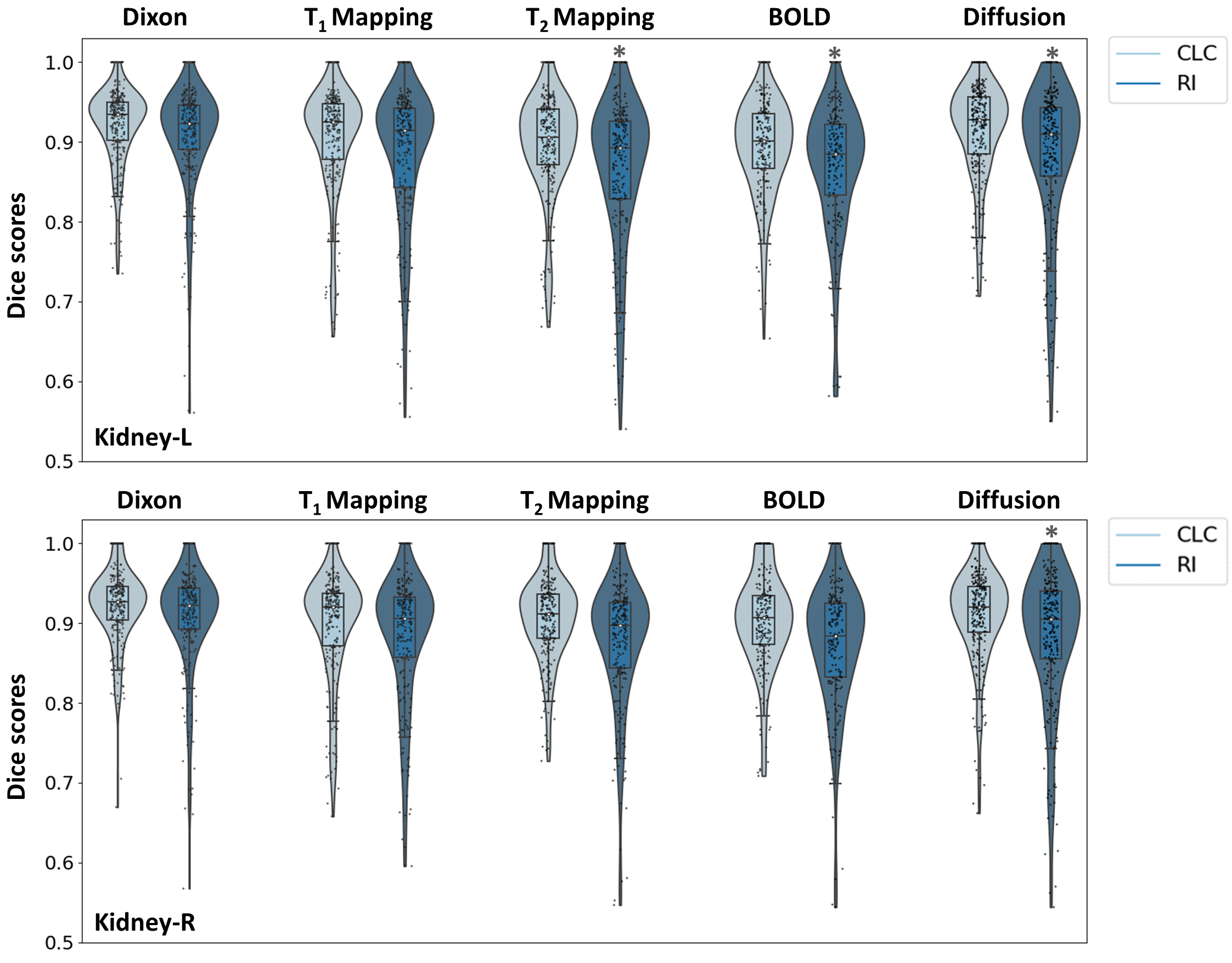
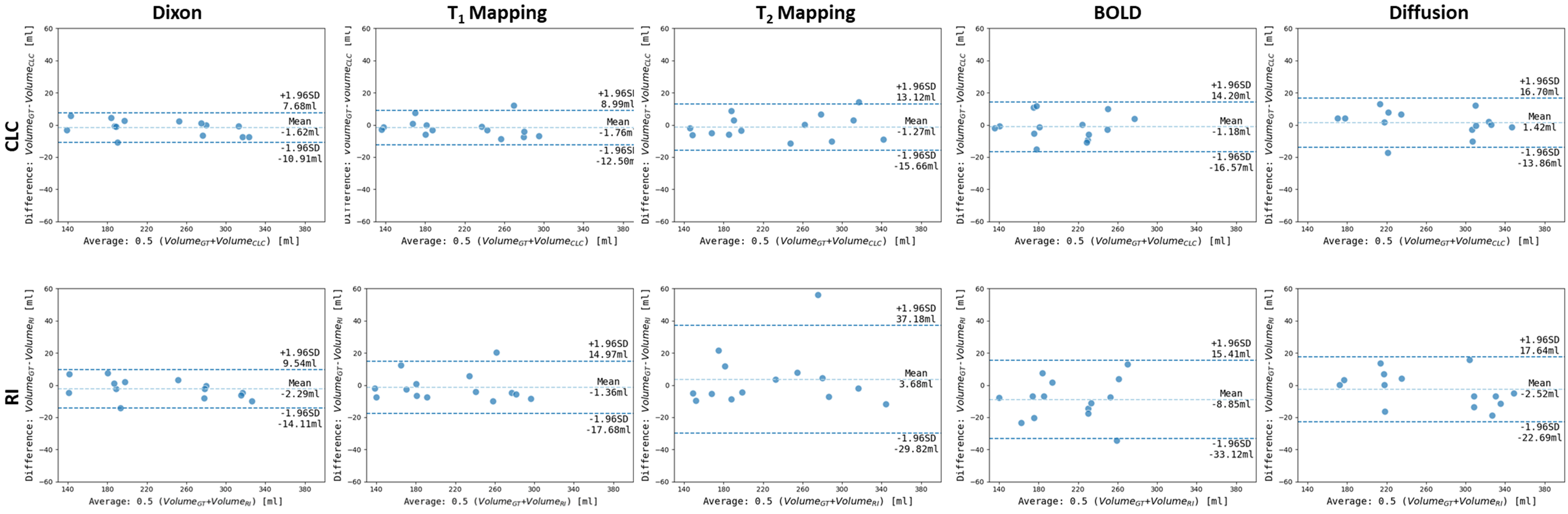
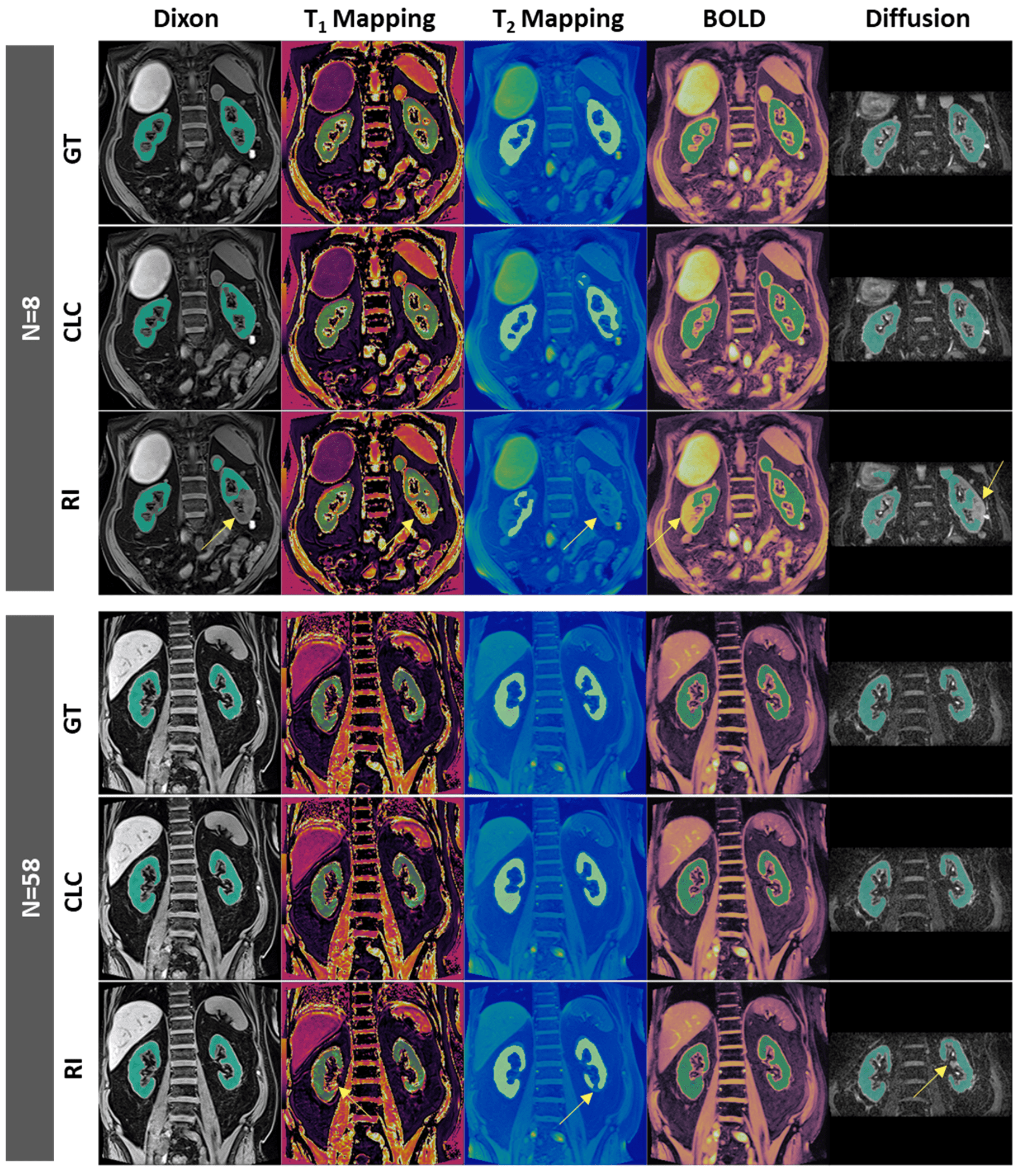
The CLC model yields higher Dice scores compared to random initialization on the segmentation task with limited data (N∈[2, 20]). A CLC-trained model on just N=8 subjects performs similarly to the RI-trained model on a larger dataset of N=20 labeled instances. This underscores a 60% reduction in annotation efforts required on our dataset for all the studied contrast images, as indicated in Table 2. CLC-trained models outperform RI-trained models when fine-tuned on N=58 labeled images, quantitatively, in terms of Dice scores of the left and right kidneys (Fig.1), and kidney volumes (Fig.2) and qualitatively (Fig.3).The superior performance of CLC-trained models across various contrasts demonstrates the capacity of the studied pretraining strategy for broad applicability. We were able to confirm the findings from the initial publication11 in a new cohort.
Conclusion
Pretraining with the multi-contrast contrastive loss reduced annotation ef-fort compared to random initialization for downstream segmentation on multi-parametric renal MRI. Additional improvements in segmentation performance were also demonstrated when a larger cohort of labeled data was used.Acknowledgements
No acknowledgement found.References
1. A. Caroli et al., “Functional magnetic resonance imaging of the kidneys: where do we stand? the perspective of the European cost action parenchima,” Nephrology Dialysis Transplantation, 2018.
2. S. Copur et al., “Future of kidney imaging: functional magnetic resonance imaging and kidney disease progression,” European Journal of Clinical Investigation, vol. 52, no. 5, p. e13765, 2022.
3. F. G. Zöllner et al., “Kidney segmentation in renal magnetic resonance imaging-current status and prospects,” IEEE Access, vol. 9, pp. 71577–71605, 2021.
4. M. Arif et al., “Clinically significant prostate cancer detection and segmentation in low-risk patients using a convolutional neural network on multi-parametric MRI,” Eur. Radiol., vol. 30, pp. 6582–6592, 2020.
5. K. R. Laukamp et al., “Fully automated detection and segmentation of meningiomas using deep learning on routine multipara-metric mri,” Eur. Radiol., vol. 29, pp. 124–132, 2019.
6. M. F. Bobo et al., “Fully convolutional neural networks improve abdominal organ segmentation,” in Medical Imaging 2018: Image Processing, vol. 10574, pp. 750–757, SPIE, 2018.
7. V. Bevilacqua et al., “A comparison between two semantic deep learning frameworks for the autosomal dominant polycystic kidney disease segmentation based on magnetic resonance images,” BMC Medical Informatics and Decision Making, vol. 19, no. 9, pp. 1–12, 2019.
8. M. Haghighi et al., “Automatic renal segmentation in dce-mri using convolutional neural networks,” ISBI 2018, pp. 1534–1537, IEEE, 2018.
9. W. Bai et al., “Self-supervised learning for cardiac MR image segmentation by anatomical position prediction,” MICCAI, Part II 22, pp. 541–549, Springer, 2019.
10. T. Chen et al., “A simple framework for contrastive learning of visual representations,” in ICML, pp. 1597–1607, PMLR, 2020.
11. L. Umapathy et al., “Reducing annotation burden in mr segmentation: A novel contrastive learning loss with multi-contrast constraints on local representations,” ISMRM, 2023.
12. L. Umapathy et al., "Reducing annotation burden in MR: A novel MR-contrast guided contrastive learning approach for image segmentation," Med Phys. 2023;1-14.
13. K. Chaitanya et al., “Contrastive learning of global and local features for medical image segmentation with limited annotations,” Adv. neural inf. process. syst, vol. 33, pp. 12546–12558, 2020.
14. N. Abraham and N. M. Khan, “A novel focal tversky loss function with improved attention u-net for lesion segmentation,” ISBI, pp. 683–687, IEEE, 2019;5
Figures