2092
Scalable and Transferable U-Net for Accurate Simultaneous 3D MRI Segmentation of Gestational Sac and Decidual Tissue in Cesarean Scar Pregnancy1GE Healthcare, Shanghai, China, 2Shanghai AI Laboratory, Shanghai, China, 3Shanghai first maternity and infant hospital, Shanghai, China
Synopsis
Keywords: Analysis/Processing, Uterus, Large-scale Deep Learning, Cesarean scar pregnancy, gestational sac
Motivation: Cesarean scar pregnancies (CSP) pose significant risks and complications. Accurate segmentation of the gestational sac (GS) and decidual tissue (DEC) in CSP through MRI is crucial for diagnosis, but current methods are limited in effectiveness.
Goal(s): Introduce a large-scale and pre-trained model, Scalable and Transferable U-Net (STU-Net), to accurately segment GS and DEC simultaneously.
Approach: 151 CSP females with structural MRI were enrolled. STU-Net was trained and evaluated.
Results: The proposed STU-Net achieved promising segmentation performance.
Impact: The proposed STU-Net enables precise segmentations of GS and DEC, potentially enhancing the diagnostic accuracy of CSP.
Introduction
Cesarean scar pregnancy (CSP) refers to a unique form of ectopic pregnancy where a gestational sac (GS) implants on a scar from a previous cesarean section incision [1]. The rising cesarean section rate has contributed to an increase in the incidence of CSP, which can lead to serious life-threatening complications[2-3]. MRI is vital in diagnosing CSP promptly, but accurate segmentation of the GS and surrounding decidual tissue (DEC) is time-consuming for radiologists, impeding further quantitative assessment and analysis [4].Several deep learning networks (DL) have shown promising results in segmenting the uterus in volumetric MR images [5-6]. However, accurate segmentation of the GS and DEC in CSP cases poses additional challenges due to their more complex anatomical structures. Currently, there are limited automatic segmentation models specifically designed for this task. Furthermore, existing networks often require extensive fine-tuning to accommodate different tasks and datasets, thereby limiting their applicability and transferability.
Recently, a large-scale supervised pre-trained deep learning model for medical image segmentation, called Scalable and Transferable U-Net (STU-Net), has been introduced [7]. Previous research demonstrated that STU-Net can automatically configure task-specific hyperparameters and has shown promising results in multiple segmentation tasks [7]. Building upon this potential, our study aimed to apply STU-Net to perform 3D MRI segmentation in CSP cases, evaluating its ability to accurately segment both the GS and the DEC simultaneously.
Methods and Materials
Patients151 CSP females (mean age: 34.67±4.86) were enrolled. The datasets were randomly divided into training and test sets at a ratio of 7:3. All patients underwent MRI examinations using a 1.5T MR scanner (OPTIMA MR360, GE HealthCare) with an 8-channel phased-array coil. The three-dimensional CUBE sequence was selected. The acquisition parameters were as follows: TR/TE, 2000 ms/91-95 ms; slice thickness, 1.6 mm; intersection gap, 0; matrix size, 228 ×228; FOV, 24x24cm2.
Model Construction
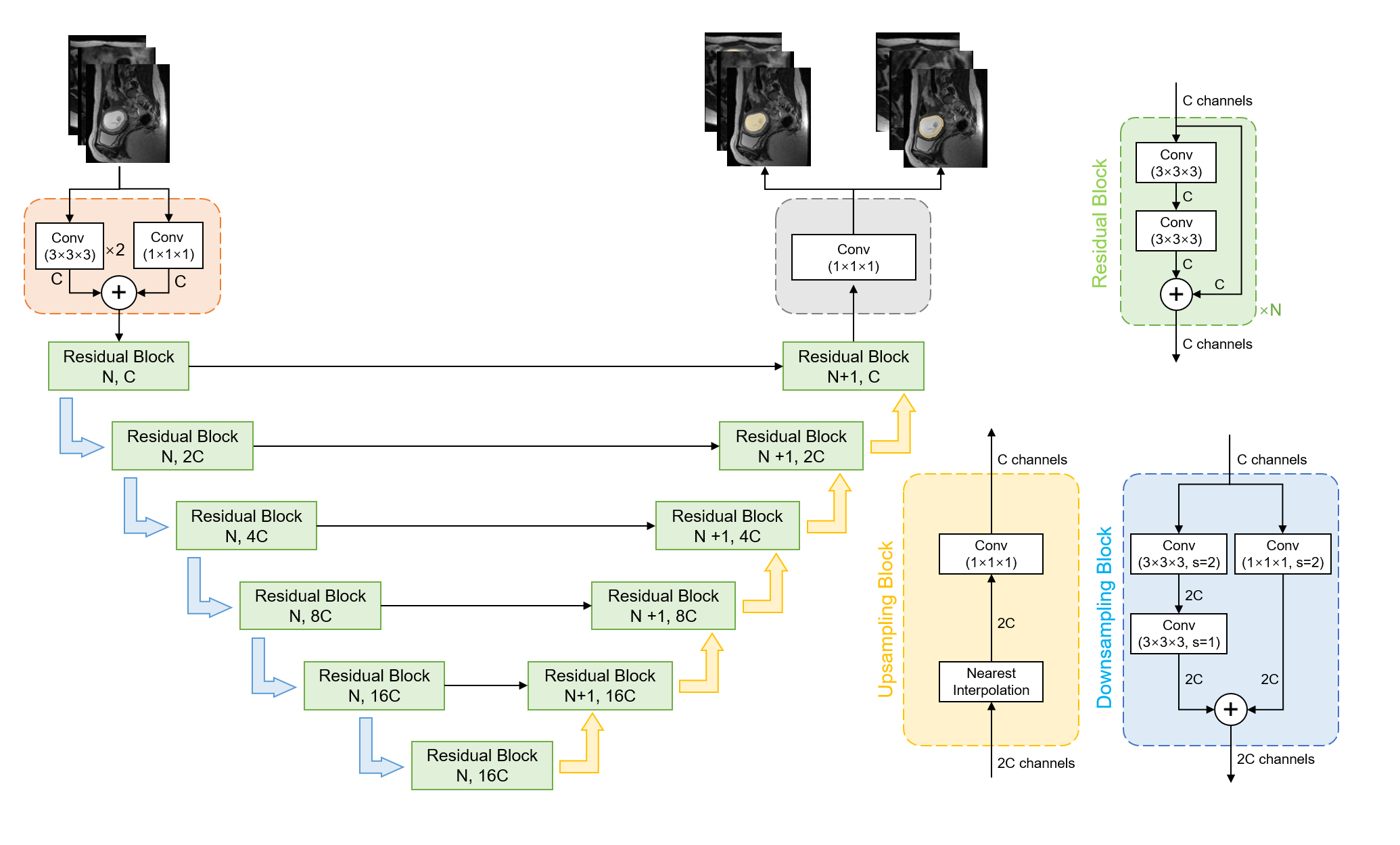
The general architecture of STU-Net is illustrated in Fig.1. The architecture of STU-Net was built upon the traditional U-Net with three primary modifications. Firstly, a residual block was introduced in each stage, replacing the plain convolution block used in the traditional U-Net. Secondly, the downsampling block in encoder had two branches. The left branch consisted of two 3×3×3 convolutions with different strides: a stride of 1 for the former and a stride of 2 for the latter. The right branch used a kernel size of 1×1×1 with a stride of 2 to match the output shape of the left branch. Lastly, for the upsampling block in the decoder, STU-Net employed nearest interpolation followed by a 1×1×1 convolution with a stride of 1 as a replacement for the traditional transpose convolution. This weight-free interpolation alleviated the weight shape issues.
Training Process
The dataset was normalized using a target spacing of (1.600, 0.7227, 0.7227). During the training stage, we fine-tuned STU-Net using the official pre-trained models from (https://github.com/uni-medical/STU-Net), which were initially trained on the TotalSegmentator dataset [8]. The learning rate was set as 0.001 for both the encoder and decoder and as 0.01 for the segment head. The input size was (40, 224, 224) and a batch size of 2 was used. The training comprised 250,000 iterations. The performance of STU-Net was evaluated using dice coefficient (Dice) and 95% Hausdorff Distance (HD95).
Results
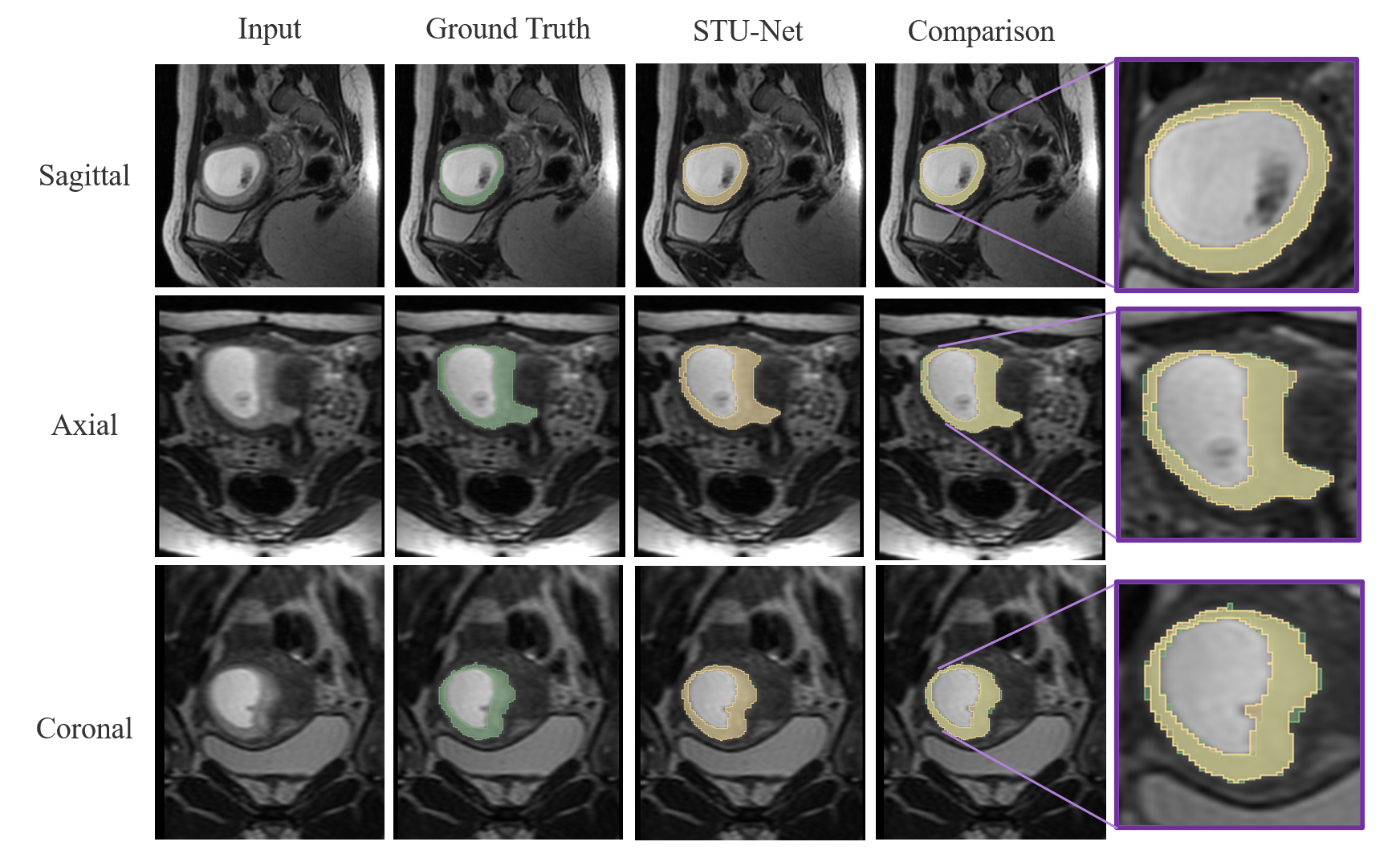
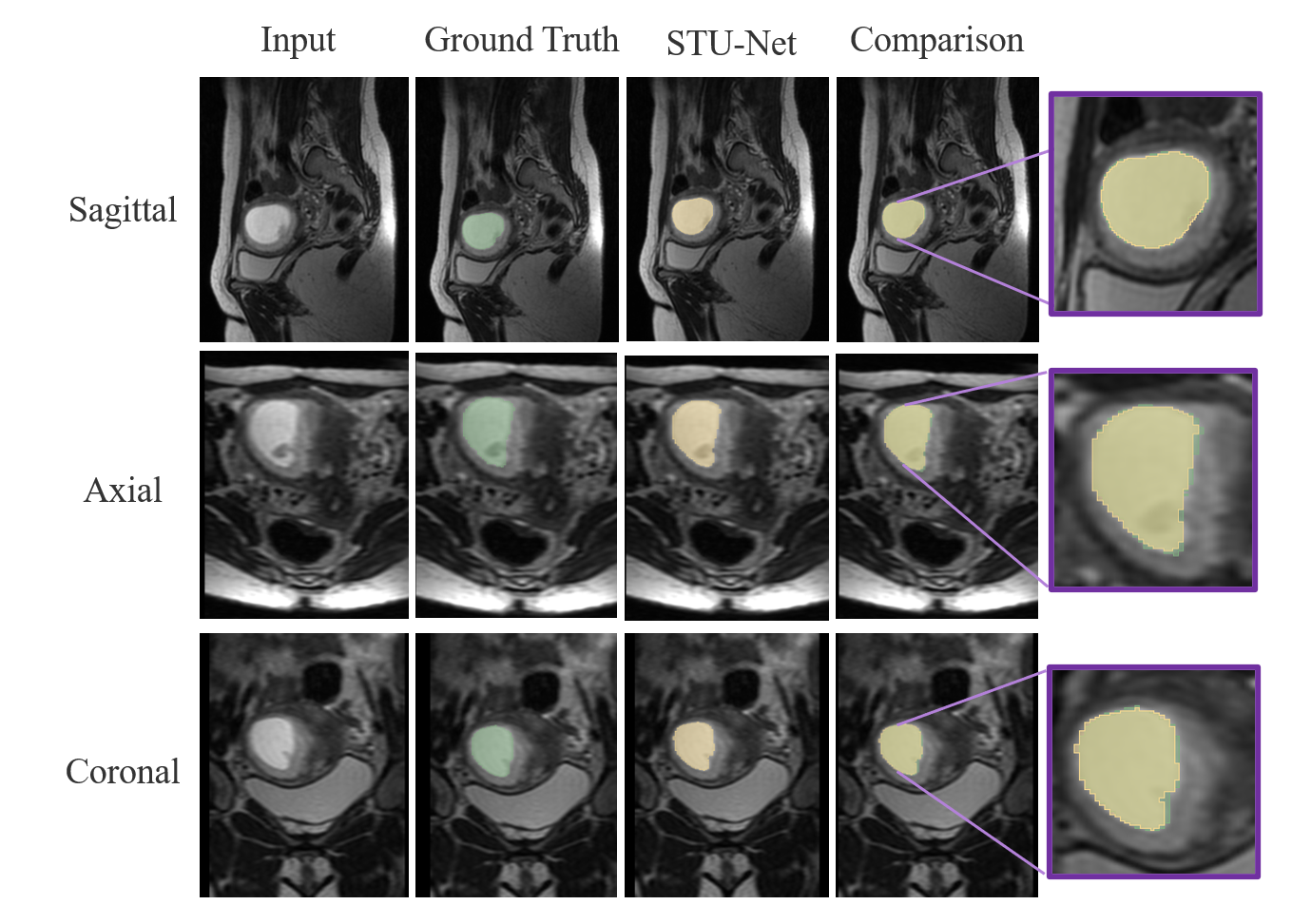
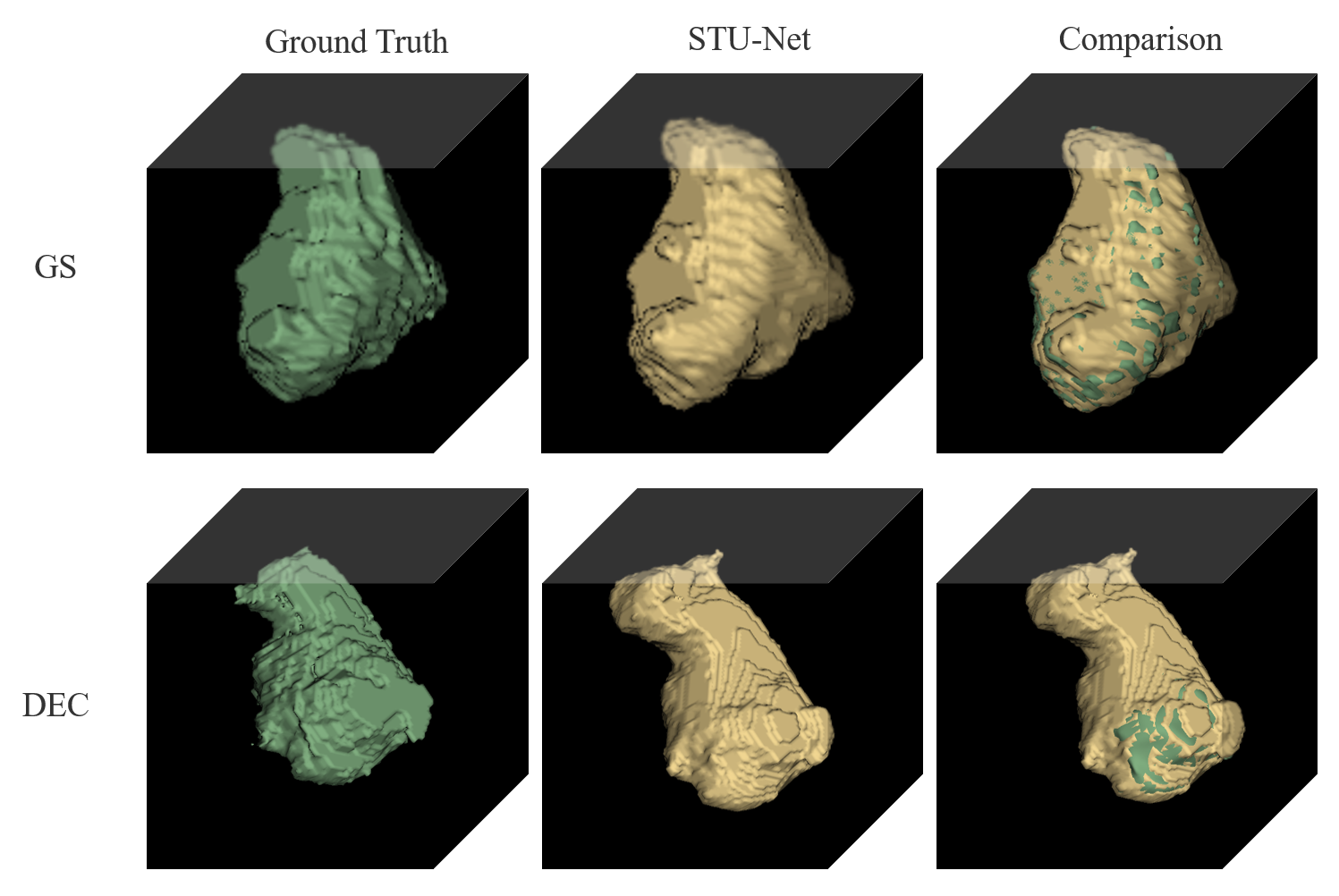
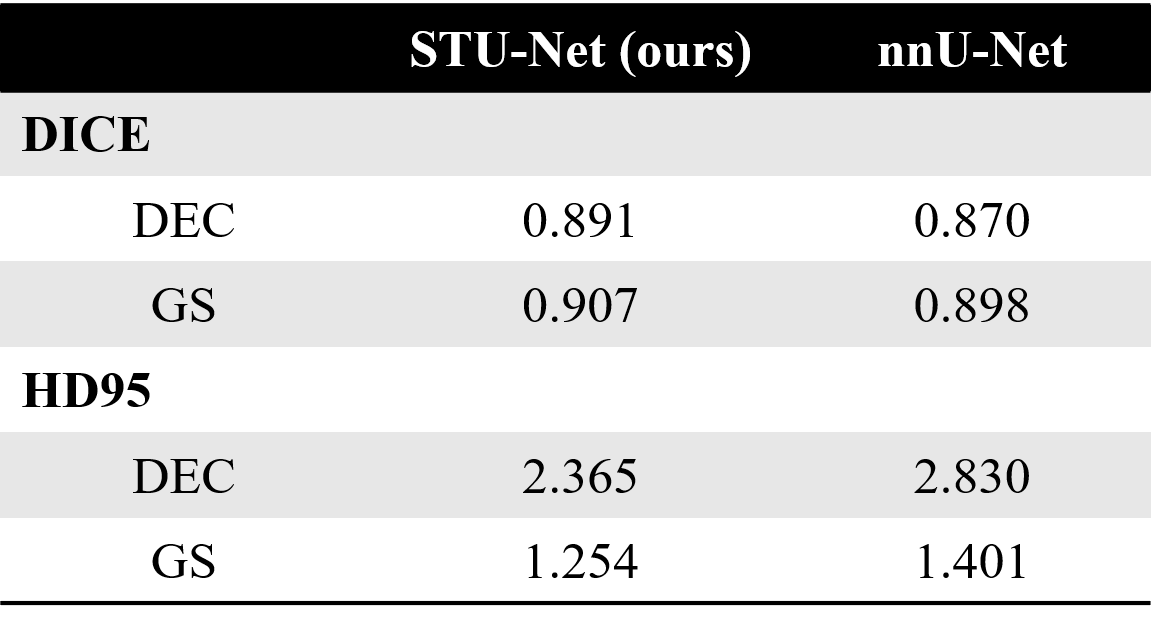
Tab.1 presents the model performance of STU-Net compared to the referenced nnU-Net for segmenting the GS and DEC in the test dataset. STU-Net outperformed nnU-Net with higher Dice and lower HD95 for both GS (0.907 vs 0.898, 1.254 vs 1.401) and DEC (0.891 vs 0.870, 2.365 vs 2.830). Fig.2 and Fig.3 provide more detailed segmentation results for DEC and GS, respectively. Fig.4 presents another example of a CSP female illustrating the segmentation results of DEC and GS in a three-dimensional pattern.Discussion and Conclusion
In this study, we utilized the Scalable and Transferable U-Net (STU-Net), a large-scale pre-trained model, to perform segmentation of gestational sac (GS) and surrounding decidual tissue (DEC) in females with cesarean scar pregnancy (CSP). The results demonstrated the effectiveness of STU-Net in precise segmentation.In conclusion, the effective transferability of STU-Net in segmenting the GS and DEC provided potential assistance in diagnosing and managing CSP cases. By automating the segmentation process and delivering reliable results, the application of STU-Net held promise in improving patient outcomes and enhancing efficiency in CSP diagnosis and management.
Acknowledgements
none.References
[1] Allerkamp HH, Clark AR, et al. Something old, something new: digital quantification of uterine vascular remodelling and trophoblast plugging in historical collections provides new insight into adaptation of the utero-placental circulation. Hum Reprod 2021, 36(3):571-586.
[2] Tang Y, Zhang Y, et al. A Comparison of Ultrasound Guided Curettage With and Without Uterine Artery Embolization on Controlling Intraoperative Blood Loss for a Cesarean Scar Pregnancy Treatment: Study Protocol for a Randomized Clinical Trial. Front Endocrinol (Lausanne) 2021, 12:651273.
[3] Timor-Tritsch IE, Monteagudo A, Cali G et al. Easy sonographic differential diagnosis between intrauterine pregnancy and cesarean delivery scar pregnancy in the early first trimester. Am J Obstet Gynecol 2016; 215: 225 e1-7.
[4] Xiao X, Ding R, et al. Diagnostic performance of magnetic resonance imaging and ultrasonography on the detection of cesarean scar pregnancy: A meta-analysis. Medicine (Baltimore) 2021, 100(48):e27532.
[5] Shahedi, Maysam et al. “Deep learning-based segmentation of the placenta and uterus on MR images.” Journal of medical imaging (Bellingham, Wash.) vol. 8,5 (2021): 054001.
[6] Kurata, Yasuhisa et al. “Automatic segmentation of the uterus on MRI using a convolutional neural network.” Computers in biology and medicine vol. 114 (2019): 103438.
[7] Ziyan H, Haoyu W, et al. “STU-Net: Scalable and Transferable Medical Image Segmentation Models Empowered by Large-Scale Supervised Pre-training” arXiv:2304.06716, 2023.
[8] Jakob Wasserthal, Manfred Meyer, et al. Totalsegmentator: robust segmentation of 104 anatomical structures in ct images. arXiv preprint arXiv:2208.05868, 2022. 2, 5, 6
Figures