2084
Neurochemistry, microstructure, and perfusion in long-COVID: An interim analysis from a multisite study1Center for Magnetic Resonance Research, Department of Radiology, University of Minnesota, Minneapolis, MN, United States, 2Department of Neurology, University of Minnesota, Minneapolis, MN, United States, 3School of Public Health, Division of Biostatistics, University of Minnesota, Minneapolis, MN, United States, 4Mayo Clinic, Rochester, MN, United States, 5Athinoula A. Martinos Center for Biomedical Imaging, Department of Radiology, Massachusetts General Hospital, Boston, MA, United States, 6Department of Radiology, Harvard Medical School, Boston, MA, United States, 7Johns Hopkins University, Baltimore, MD, United States, 8The Houston Methodist Research Institute, Houston, TX, United States
Synopsis
Keywords: Infectious Disease, COVID-19, Arterial Spin labelling, Brain, Brain Connectivity, Diffusion Tensor Imaging, Microstructure, Multimodal, Spectroscopy, Perfusion
Motivation: There is an urgent need to understand the biological basis of long-COVID.
Goal(s): To elucidate long-term consequences of SARS-CoV-2 infection in the brain using advanced MRI.
Approach: In a multisite study, we collected single-voxel MRS, diffusion MRI, pCASL and T2 FLAIR MRI, to investigate the neurochemistry, microstructure, perfusion, and white matter hyperintensities (WMH) in participants suffering from long-COVID.
Results: Participants with long-COVID have long-lasting effects (that persist years after acute infection) in the neurochemistry, microstructure, and perfusion, primarily in the brainstem, midbrain and diencephalon, and their connecting tracts, without the presence of overt white matter pathology.
Impact: Multi-modal advanced MRI demonstrates long-lasting effects of COVID-19 in the brain, including neurochemical and microstructural abnormalities and perfusion deficits. These insights may facilitate the treatment and care of people suffering from long-COVID.
Introduction
Long-COVID is characterized by long-term health problems persisting or appearing after acute SARS-CoV-2 infection. Neurological and cognitive symptoms are frequently reported by patients with long-COVID. Approximately 10% of patients experience long-COVID after acute infection, with no current treatment1. Defining the biological basis of these symptoms is critical to develop interventions and appropriate care to individuals suffering from long-COVID. In this multisite study, we aim to better understand the long-term consequences of SARS-CoV-2 infection in the brain using advanced MRI.Methods
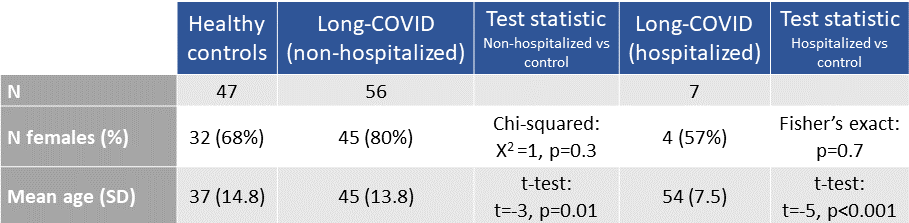
Harmonized methods were used to collect multimodal MR data across 5 sites. Here, we present interim cross-sectional analyses from single-voxel MRS, diffusion MRI, pseudocontinuous arterial spin labeling (pCASL) and T2 FLAIR.Participants with long-COVID were enrolled if they had neurological sequelae in the 6 months after a confirmed SARS-CoV-2 infection and continued to show at least one neurological symptom. Participants were scanned on average 596 (± 298) days post-infection. Control participants were enrolled if they had no prior COVID-19 symptoms and diagnosis (Figure 1).
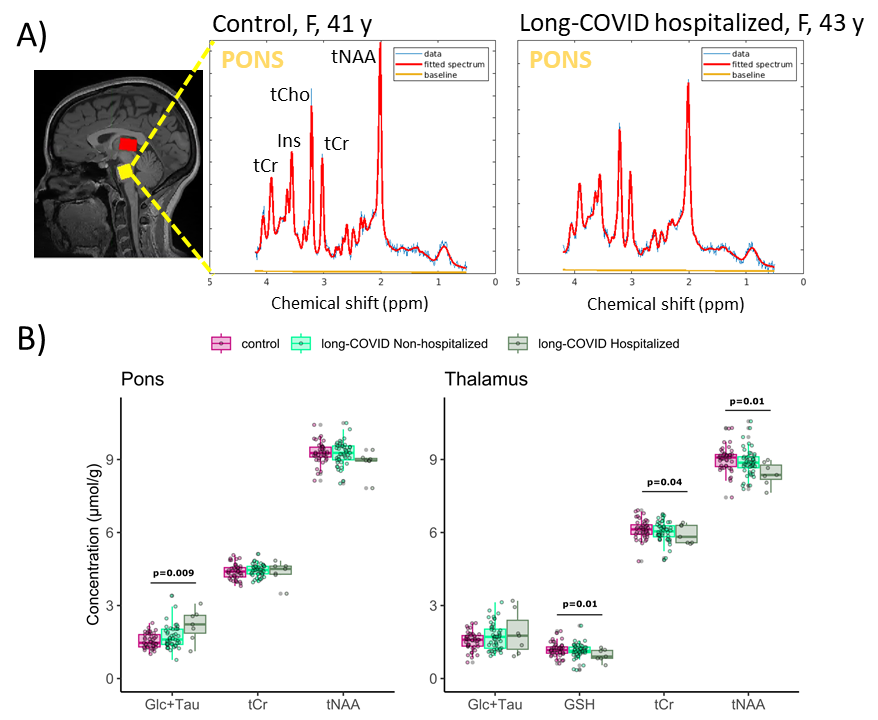
MR data were acquired on SIEMENS Prisma 3T scanners. 1H-MRS data were obtained from the pons (16x16x16 mm3) and bilateral thalamus (21(AP)x36(LR)x14(FH) mm3), using a short-echo semi-LASER protocol2. Spectra were corrected for frequency, phase and eddy-current errors using MRspa3 before quantification in LCModel with simulated basis set. Diffusion and pCASL acquisition parameters and processing were based on the Human Connectome Protocol (HCP)4,5.
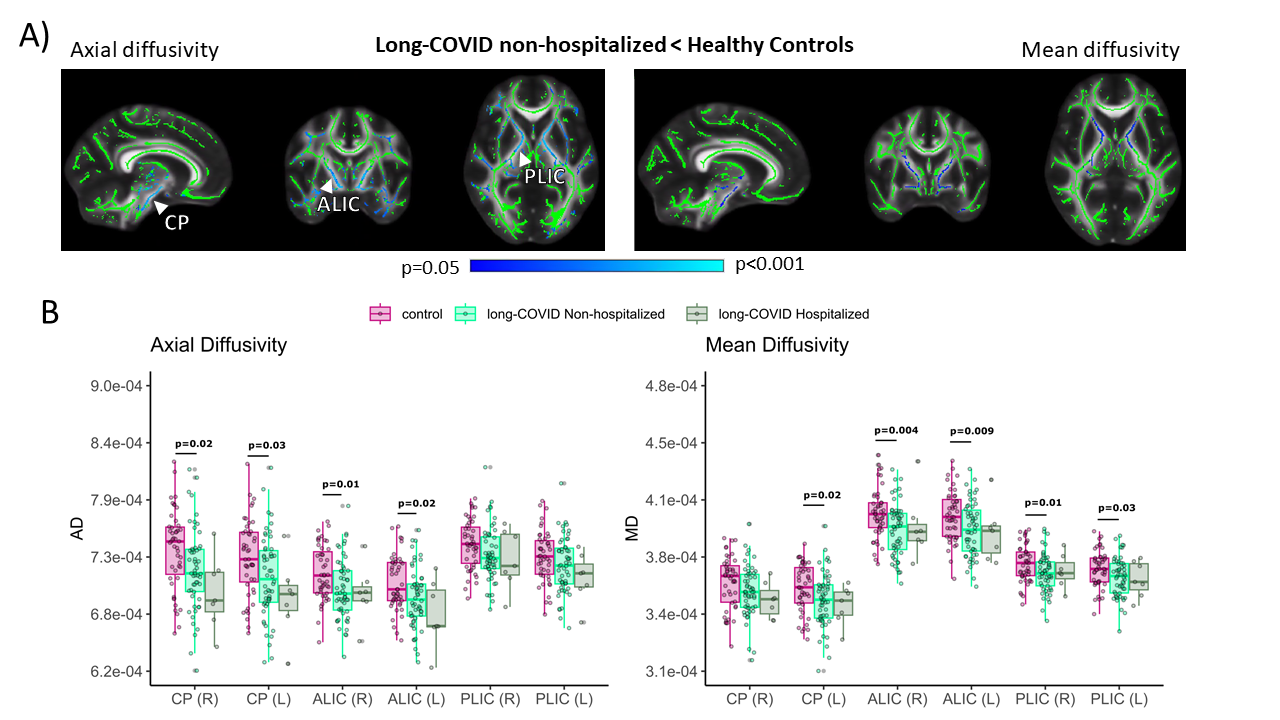
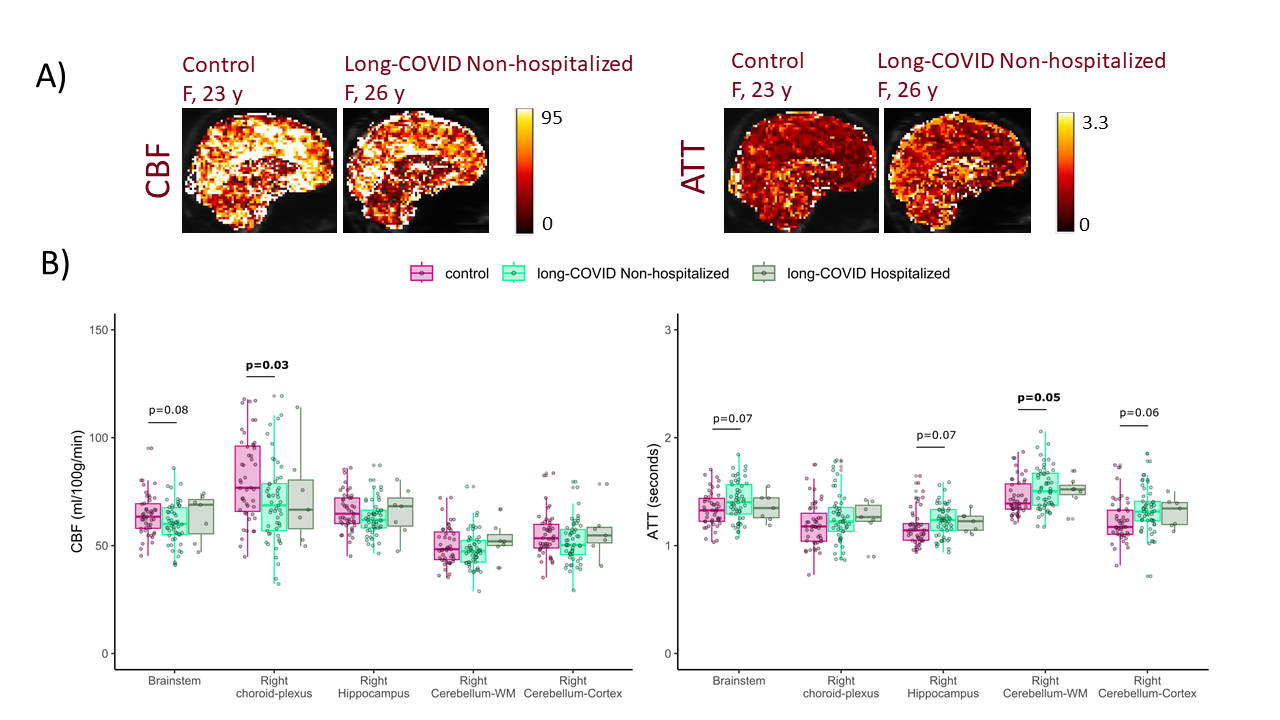
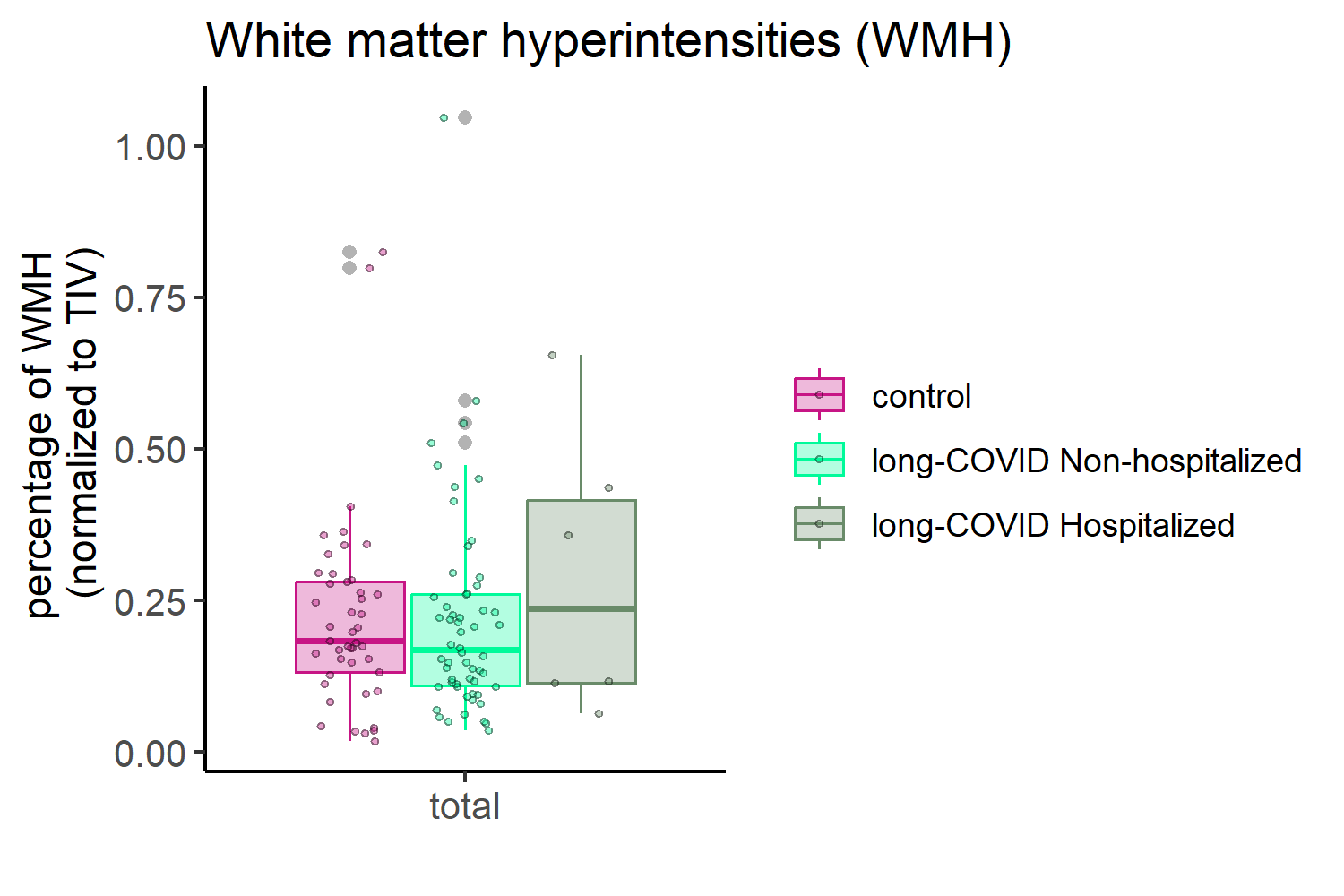
Fractional anisotropy (FA), axial-, radial-, and mean diffusivity (AD, RD, and MD, respectively) values were calculated using DTIFIT (FSL). TBSS (FSL) was used for voxel-wise permutation analysis of DTI maps. The randomize function was used with TFCE6, generating cluster-size statistics based on 5000 permutations. Mean regional FA, AD, RD, and MD values were further extracted in the native space, using an atlas-based segmentation (JHU white matter atlas) as previously described7. Cerebral blood flow (CBF) and arterial transit time (ATT) were calculated from pCASL data5, using tissue masks based on T1-weighted images processed with FreeSurfer. White matter hyperintensity (WMH) volumes were derived from a semi-automated segmentation of FLAIR images8, normalized to intracranial volume.
ANOVA, followed by Tukey’s post-hoc tests, were used to compare each long-COVID group (hospitalized or non-hospitalized during acute infection) to controls, while accounting for age and sex differences.
Results
This report included 110 participants, of which 63 suffered from long-COVID (n=56 non-hospitalized and n=7 hospitalized) and 47 were controls (Figure 1). Participants with long-COVID were older than controls (non-hospitalized p=0.01, hospitalized p<0.001).Hospitalized participants with long-COVID showed neurochemical differences in the pons and thalamus. Specifically, they had higher Glucose+Taurine (Glc+Tau) in the pons and lower glutathione (GSH), total creatine (tCr) and total N-acetylaspartate (tNAA) in the thalamus, than controls (Figure 2).
Non-hospitalized participants with long-COVID had lower AD and MD in the cerebral peduncle and in both the anterior and posterior limbs of the internal capsule (Figure 3).
Non-hospitalized participants with long-COVID had lower CBF in the choroid-plexus and trends for lower CBF in the brainstem, and higher ATT in the cerebellum and trends for higher ATT in the brainstem and hippocampus (Figure 4).
No group differences were found in WMH volumes (Figure 5).
Discussion
These findings suggest that long-COVID is associated with alterations in neurochemistry of the pons and thalamus, microstructural damage in tracts that connect the cerebrum to the brainstem/pons and perfusion deficits primarily in infratentorial structures that persist up to 2 years post-infection.Lower tNAA and GSH in hospitalized cases indicate neuronal dysfunction and oxidative stress in the thalamus. Lower GSH is consistent with a prior long-COVID report from frontal gray matter9. Higher Glc+Tau in the brainstem points to energy deficits, either due to COVID-19-related hyperglycemia10 or lower glucose utilization.
Lower AD and MD have also been previously reported in participants with long-COVID, specifically in the corpus callosum, forceps minor, middle longitudinal fasciculus, uncinate tract and fronto-occipital fasciculus11. These findings in diffusivity could indicate axonal damage, reduced brain perfusion, and/or hypoxia11,12.
Lower CBF and higher ATT in infratentorial structures could be associated with lower AD and MD observed in the cerebral peduncle, a tract that connects the brainstem to the cerebrum. Further analyses will elucidate on how these measures relate.
Conclusion
By combining advanced multi-modal MRI, this study revealed neurochemical, microstructural and perfusion deficits primarily in the brainstem, midbrain, diencephalon, and their connecting tracts in participants with long-COVID. These diffusion (lower diffusivity), perfusion (lower CBF, higher ATT) and functional (lower tNAA, GSH) deficits were observed in the absence of increases in WMH. Future work will focus on age-matching the cohorts and investigating how imaging measures relate to observed clinical phenotypes and symptom severity.Acknowledgements
R01NS124065, R01NS124065-02S1, P41 EB027061, 1S10OD017974-01.References
1. Thaweethai, T. et al. Development of a Definition of Postacute Sequelae of SARS-CoV-2 Infection. JAMA 329, 1934–1946 (2023).
2. Deelchand, D. K. et al. Plug-and-play advanced magnetic resonance spectroscopy. Magn. Reson. Med. 87, 2613–2620 (2022).
3. Deelchand, D. K. MRspa: Magnetic Resonance signal processing and analysis. https://www.cmrr.umn.edu/downloads/mrspa/.
4. Harms, M. P. et al. Extending the Human Connectome Project across ages: Imaging protocols for the Lifespan Development and Aging projects. NeuroImage 183, 972–984 (2018).
5. Juttukonda, M. R. et al. Characterizing cerebral hemodynamics across the adult lifespan with arterial spin labeling MRI data from the Human Connectome Project-Aging. NeuroImage 230, 117807 (2021).
6. Smith, S. M. & Nichols, T. E. Threshold-free cluster enhancement: Addressing problems of smoothing, threshold dependence and localisation in cluster inference. NeuroImage 44, 83–98 (2009).
7. Park, Y. W. et al. Assessment of Cerebral and Cerebellar White Matter Microstructure in Spinocerebellar Ataxias 1, 2, 3, and 6 Using Diffusion MRI. Front. Neurol. 11, (2020).
8. Raz, L. et al. Thrombogenic microvesicles and white matter hyperintensities in postmenopausal women. Neurology 80, 911–918 (2013).
9. Saleh, M. G. et al. Ongoing oxidative stress in individuals with post-acute sequelae of COVID-19. NeuroImmune Pharmacol. Ther. 2, 89–94 (2023).
10. Barreto, E. A. et al. COVID-19-related hyperglycemia is associated with infection of hepatocytes and stimulation of gluconeogenesis. Proc. Natl. Acad. Sci. 120, e2217119120 (2023).
11. Díez-Cirarda, M. et al. Multimodal neuroimaging in post-COVID syndrome and correlation with cognition. Brain J. Neurol. 146, 2142–2152 (2023).
12. Kumar, R. et al. Altered Global and Regional Brain Mean Diffusivity in Patients with Obstructive Sleep Apnea. J. Neurosci. Res. 90, 2043–2052 (2012).
Figures