2083
Brain long distance functional connectivity mediates the relationship between fatigue and PTSD after COVID-19 infection.1Department of Medical Imaging, First Affiliated Hospital of Xi’an Jiaotong University, Xi'an City, China, 2GE HealthCare MR Research, Beijing City, China
Synopsis
Keywords: Infectious Disease, COVID-19
Motivation: Brain network alterations in acute phase of coronavirus disease 2019 patients (acute-COVID) with fatigue has not yet been elucidated.
Goal(s): Our goal was to determine the characteristics of alterations in brain network and the neurobiological mechanisms in acute-COVID patients with fatigue.
Approach: We utilized graph theory analysis to assess brain network alterations in COVID-19 patients.
Results: Results demonstrated the abnormalities in brain network in acute-COVID patients with fatigue, involing left insular gyrus and right inferior frontal gyrus. Morever, the normalized characteristic path length of global brain in acute phase of COVID-19 could predict the development of chronic symptoms.
Impact: Our functional MRI findings highlight abnormal brain network metrics in acute phase COVID-19 patients with fatigue, offering valuable neuroimaging marker for early clinical intervention in long-COVID patients.
Introduction
Fatigue and post-traumatic stress disorder (PTSD) frequently manifest in cases of long-coronavirus disease 2019 (long-COVID) and substantially contribute to the overall burden associated with this condition[1]. Prior research has primarily concentrated on the chronic phase (beyond three months) post-infection[2, 3]. Changes in brain functional networks during the acute-phase (within four weeks) remain unknown. This study aims to explore the impact of COVID on fatigue and associated alterations in functional brain networks during the acute phase. Additionally, we will evaluate the relationship between acute-phase network metrics and fatigue and PTSD three months after infection.Methods
This study was approved by Ethics Committee of our hospital (No. XJTU1AF2023LSK-013). From January to February 2022, 153 individuals in the acute phase of COVID-19 (acute-COVID) who met Diagnosis and Treatment of Novel Coronavirus Pneumonia (Trial version 9) criteria were enrolled and divided to non-fatigue (COVID-N, n = 74) and fatigue (COVID-F, n = 79) groups. Meanwhile, 34 matched healthy controls (HC) were also recruited. All subjects underwent neuropsychological test and MRI examinations on a 3.0-Tesla MRI scanner (Discovery MR750w, GE Healthcare), and were followed up for three months. Resting-state functional MRI (rs-fMRI) data was acquired with below parameters: TR/TE 2000/30 ms, flip angle 90°, matrix size 64 × 64, field of view 25.6 × 25.6 cm2, voxel size 4 × 4 × 4 mm3, 40 axial slices, and 180 volumes. Pre-processing was performed using Data Processing Assistant for Brain Imaging (DPABI)[4]. Graph theoretical network analysis (GRETNA) was used for functional connectivity network analysis. We utilized the automated anatomical labeling (AAL) atlas to define network nodes into 246 regions of interest (ROIs)[5]. Demographic and neuropsychological data, as well as AUC values of network metrics, were compared using t-tests and ANCOVA in two and three groups. Post hoc comparisons were corrected for false discovery rate (FDR). Partial correlation analysis explored parameter correlations.Results
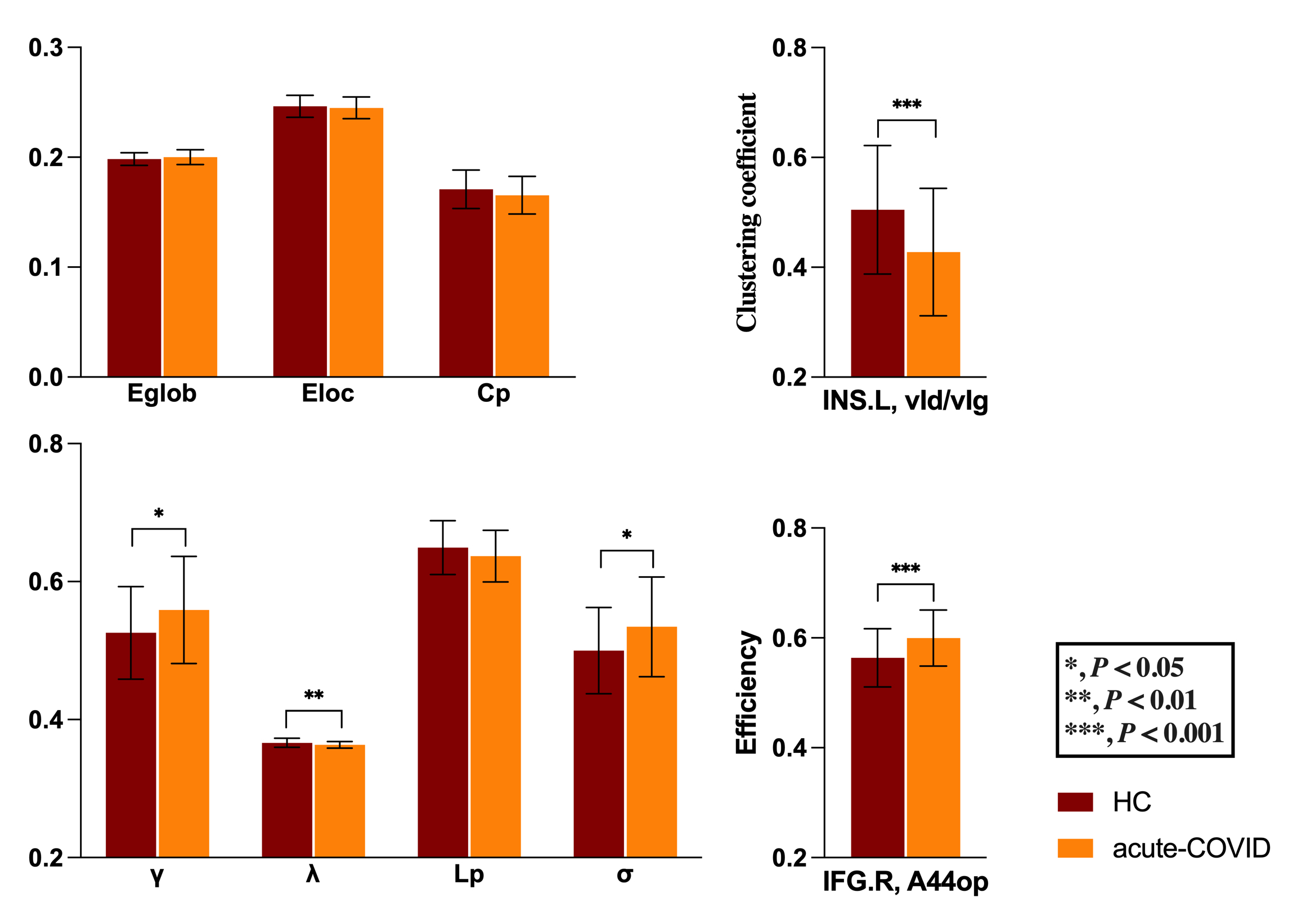
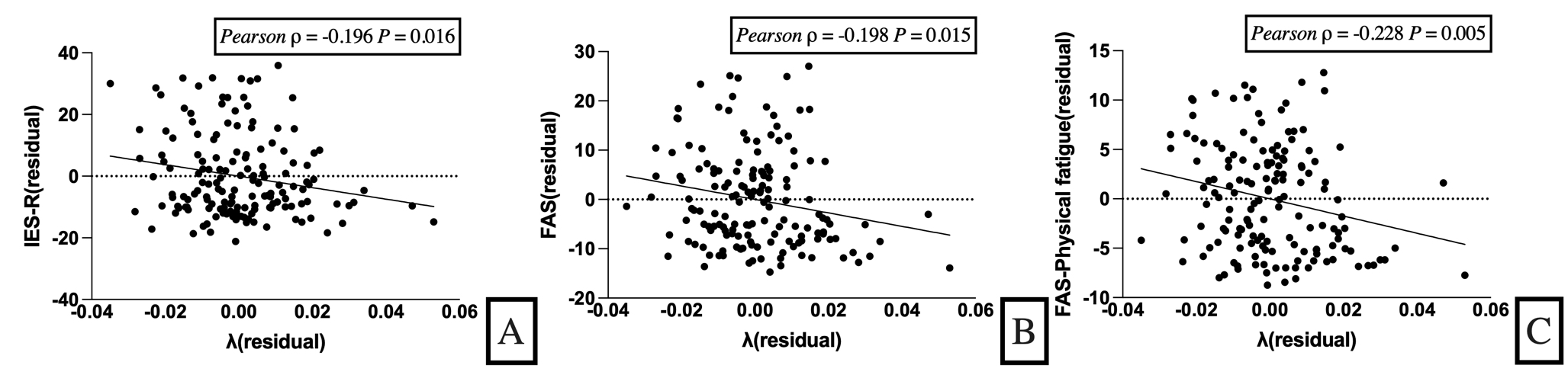
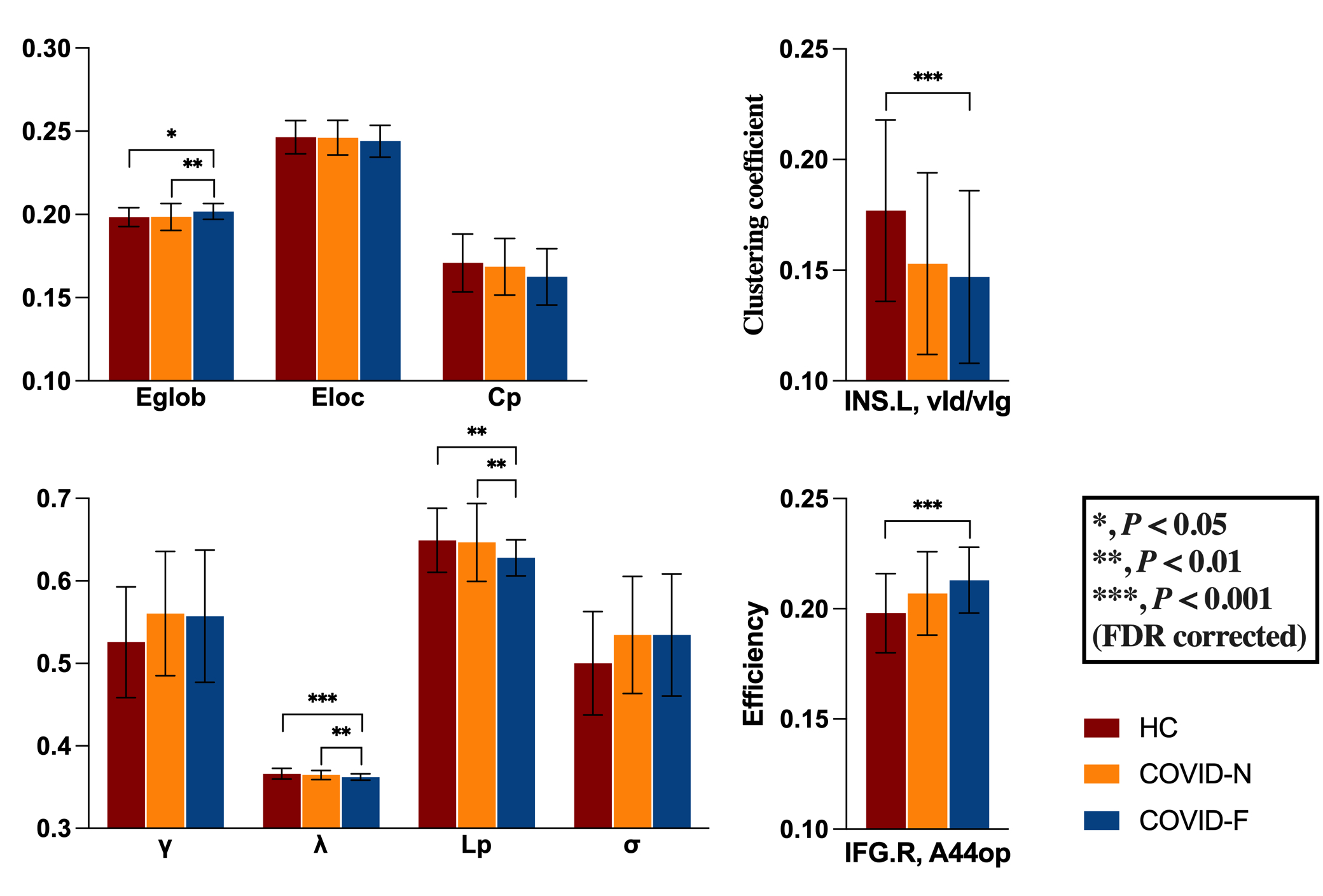
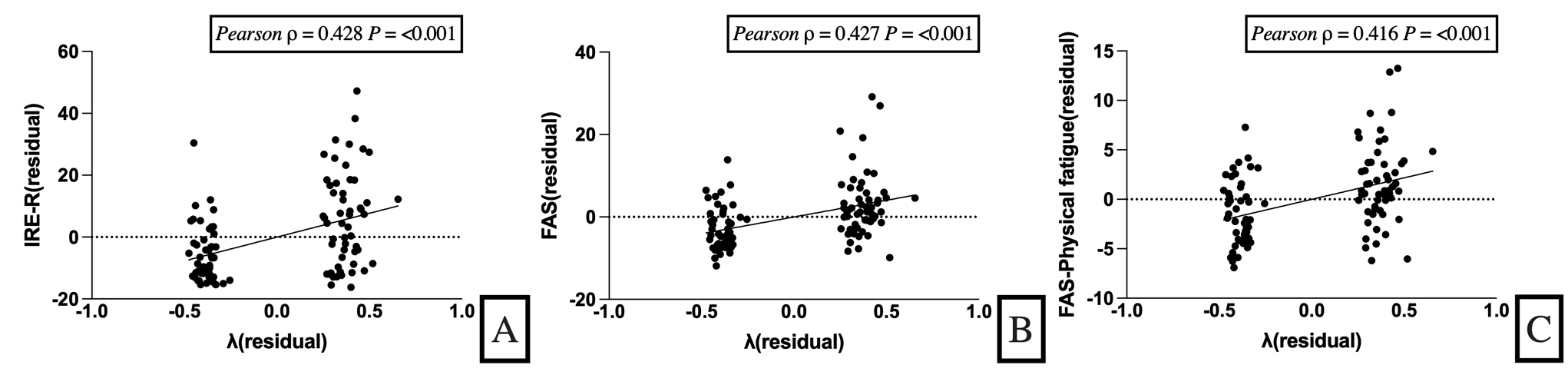
The inter-group differences in demographic, Fatigue Assessment Scale (FAS) and Impact of Event Scale-Revised (IES-R) scores for all participants are shown in Table 1. In terms of global metrics, acute-COVID showed significantly higher γ and σ (both P< 0.05) and lower λ (P < 0.01). Nodal metrics indicated that acute-COVID had a lower clustering coefficient in the left insular gyrus and higher nodal efficiency in the right inferior frontal gyrus (all P < 0.001) (Figure 1). λ of acute-COVID was negatively correlated with IES-R (Pearson ρ=-0.196, P=0.016), FAS (Pearson ρ=-0.198, P=0.015) and FAS-physical fatigue (Pearson ρ=-0.228, P=0.005) scores (Figure 2). In post hoc testing, regarding global metrics, COVID-F had significantly lower λ compared to HC and COVID-N (P < 0.001 and P < 0.01, FDR corrected), lower Lp (all P < 0.01, FDR corrected), and higher Eglob (P < 0.05 and P < 0.01, FDR corrected). Nodal metrics revealed lower clustering coefficient in the left insular gyrus and higher nodal efficiency in the right inferior frontal gyrus in COVID-F compared to HC (all P < 0.001, FDR corrected) (Figure 3). Additionally, λ in acute-COVID was positively correlated with IES-R (Pearson ρ=0.428, P<0.001), FAS (Pearson ρ=0.427, P<0.001), FAS-psychological fatigue (Pearson ρ=0.416,P<0.001) and FAS-physical fatigue (Pearson ρ=0.418, P<0.001) scores (Figure 4).Discussion
Our investigation revealed global and nodal functional network differences relative to COVID-19. Acute-COVID showed increased network segregation (higher γ) and decreased network integration (lower λ), indicative of a shift towards “weaker small-worldization” [6]. Increased nodal efficiency in the inferior frontal gyrus and decreased clustering coefficient in the insular reflect compensatory and damaged network nodes in acute-COVID, partially explaining the global network metric changes. Altered λ correlated with IES-R, FAS, and FAS-physical fatigue scores in acute-COVID, hinting at a potential role in the development of fatigue and PTSD.Among three groups, COVID-F exhibited higher Eglob and lower λ and Lp, indicating increased long-distance functional connections in patients, particularly involving the insular and inferior frontal gyrus. This further confirms our previous results. Given that the small-world model reflects an optimal balance between local specialization and global integration, these results thus indicate a disturbance of the normal balance in functional brain networks of COVID-19 patients[7].
Crucially, we found a strong positive association between acute phase network metrics and chronic phase IES-R and FAS scores, including subscales. This suggests that the level of λ during the acute phase can effectively predict the recovery of fatigue and PTSD symptoms in COVID-19 patients.
Conclusion
Our study identified significant network changes and their predictive value for chronic symptoms, offering potential for early identifying COVID-19 patients at risk of developing persistent fatigue and PTSD after infection. This may improve the management of long-COVID.Acknowledgements
Thanks to all colleagues for their cooperation and support in this project.References
[1] Schou T M, Joca S, Wegener G, et al. Psychiatric and neuropsychiatric sequelae of COVID-19 - A systematic review [J]. Brain Behav Immun, 2021, 97: 328-48.
[2] Xiong Q, Xu M, Li J, et al. Clinical sequelae of COVID-19 survivors in Wuhan, China: a single-centre longitudinal study [J]. Clin Microbiol Infect, 2021, 27(1): 89-95.
[3] Stavem K, Ghanima W, Olsen M K, et al. Prevalence and Determinants of Fatigue after COVID-19 in Non-Hospitalized Subjects: A Population-Based Study [J]. Int J Environ Res Public Health, 2021, 18(4).
[4] Yan C G, Wang X D, Zuo X N, et al. DPABI: Data Processing & Analysis for (Resting-State) Brain Imaging [J]. Neuroinformatics, 2016, 14(3): 339-51.
[5] Fan L, Li H, Zhuo J, et al. The Human Brainnetome Atlas: A New Brain Atlas Based on Connectional Architecture [J]. Cereb Cortex, 2016, 26(8): 3508-26.
[6] Bullmore E, Sporns O. The economy of brain network organization [J]. Nat Rev Neurosci, 2012, 13(5): 336-49.
[7] Zhang J, Wang J, Wu Q, et al. Disrupted brain connectivity networks in drug-naive, first-episode major depressive disorder [J]. Biol Psychiatry, 2011, 70(4): 334-42.
Figures