2076
Dysfunction of glymphatic system in recovered COVID-19 patients: A diffusion tensor image analysis along the perivascular space (DTI-ALPS)1Department of Radiology, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, China, 2Jiangxi Province Medical Imaging Research Institute, Nanchang, Jiangxi, China, 3Clinical Research Center For Medical Imaging, Nanchang, Jiangxi, China, 4MR Research, GE Healthcare, Beijing, China, 5Department of Psychiatry and Psychotherapy, Jena University Hospital, Jena, Germany., Jena, Germany, 6Center for Intervention and Research on adaptive and maladaptive brain Circuits underlying mental health (C-I-R-C), Jena-Magdeburg-Halle, Germany., Jena-Magdeburg-Halle, Germany
Synopsis
Keywords: Infectious Disease, COVID-19, Glymphatic system;DTI-ALPS
Motivation: Central nervous related sequelae are often reported in recovered COVID-19 patients. It’s unclear whether recovered patients have glymphatic impairment and clinical correlation.
Goal(s): Assessing glymphatic function in recovered patients and the clinical correlation.
Approach: 61 recovered patients and 38 healthy controls were enrolled. Glymphatic function was assessed using DTI-ALPS and compared between recovered and HC subjects.
Results: The impairment of glymphatic function was observed in recovered patients and was more obvious in older patients. It was correlated with sleep quality and anxiety status in a subgroup of recovered patients.
Impact: Our study firstly provided evidence of glymphatic function impairment in recovered COVID-19 patients.
Introduction
More than 90% of patients with COVID-19 survive, but varied types and frequencies of sequelae present after recovery, even in patients with mild symptoms after COVID-19 infection [1]. The post-sequelae symptoms range from neurocognition to respiratory and musculoskeletal symptoms, with predominant symptoms including headache, fatigue, breathlessness, arthralgia, sleep difficulties, and chest pain [2]. Within one year of follow-up, neurological symptoms and psychological abnormalities are the most reported complications of sequelae [2].Some studies postulate that this neurological syndrome may result from damage in olfactory sensory neurons, causing reduced outflow of cerebrospinal fluid through the cribriform plate and further leading to congestion of the glymphatic system with subsequent toxic build-up within the central nervous system [3]. However, the relationship between COVID-19 infection and glymphatic function has not been clarified. Diffusion tensor imaging (DTI) has been proposed as a noninvasive method to evaluate glymphatic function by calculating the diffusion metrics along the perivascular space (DTI-ALPS). The DTI-ALPS index was shown to be closely related to glymphatic clearance function as assessed by classical methods [4]. Thus, this study aimed at investigating if the glymphatic function was declined in recovered COVID-19 patients using DTI-ALPS.
Methods and Materials
Patients61 patients recovered from COVID-19 and 38 age- and sex- matched healthy controls (HC) were enrolled. They all received clinical assessment including MoCA, FSS, PHQ-9, PSQI, GAD-7, HAMD,and HAMA.
MRI acquisition
MRI scans were performed using a 3T scanner (Signa Premier; GE Healthcare, CA, USA) with 32-channel head coil. DTI was conducted using spin-echo single-shot echo-planar pulse sequences with 32 diffusion directions: TR/TE=1015/73.5ms, slice thickness=2.5 mm, matrix size= 28×128, FOV =224×224mm2, and b-value=1000 s/mm2. SWAN was used and acquired with TR/TE=43.2/4.0ms, slice thickness=2 mm, matrix size=220×220mm2, FOV=224×224mm2, and flip angle=20o.
Data analysis
The data were processed using DSI studio software (version 2021). Diffusion images for each subject were registered to SWAN to accurately select the brain areas with veins and perivascular spaces running over the x-axis. Over the slice, using the colour-coded principal diffusion direction map, we drew two regions of interest (ROIs): one ROI was drawn over the area of projection fibre and the other over the area of associative fibre. The DTI-ALPS index is calculated as follows: DTI-ALPS=mean(Dx-proj, Dx-assoc)/mean(Dy-proj, Dz-assoc). A low DTI-ALPS index indicated impaired glymphatic function.
Statistical analysis
Comparisons were conducted using the chi-square test for categorical variables and independent samples t test or the Mann‒Whitney test for continuous variables according to a normal distribution tested with the Shapiro‒Wilk test. Continuous variables are represented as the mean values with standard deviations. One-tailed Pearson correlation was used for correlation analysis. Statistical significance was defined when the p value was less than 0.05.
Result
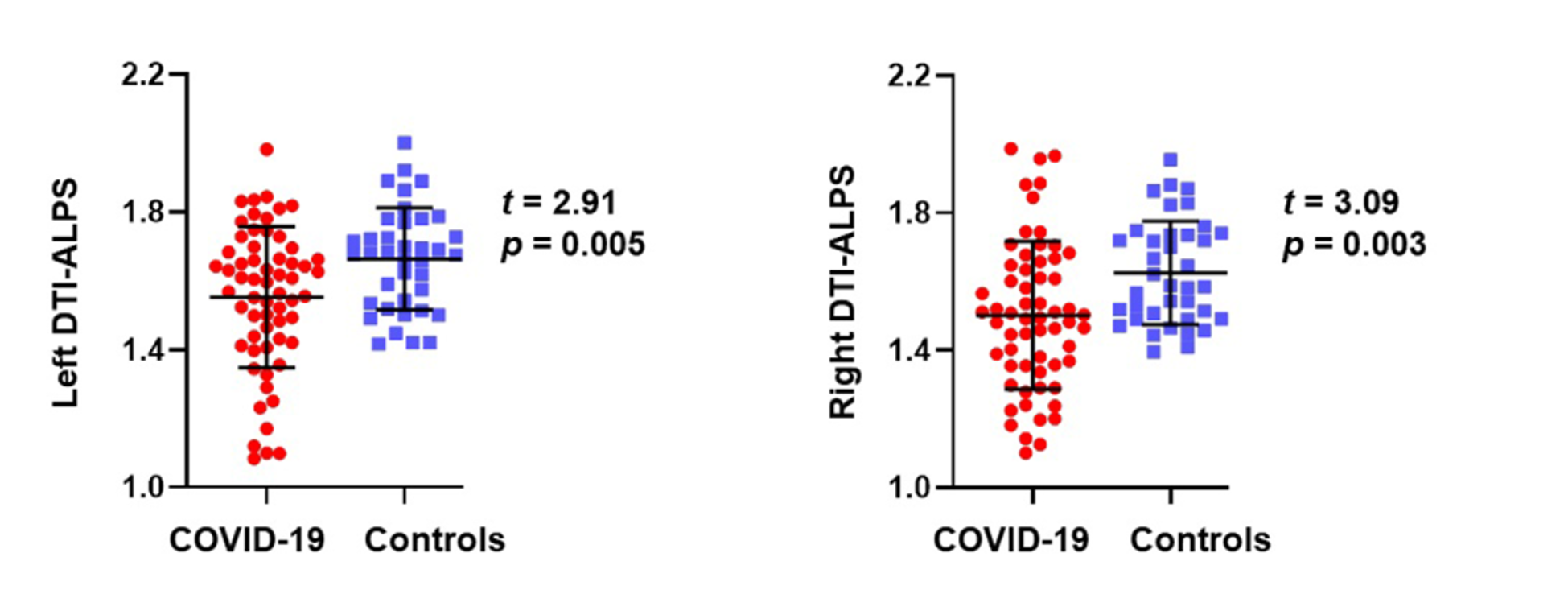
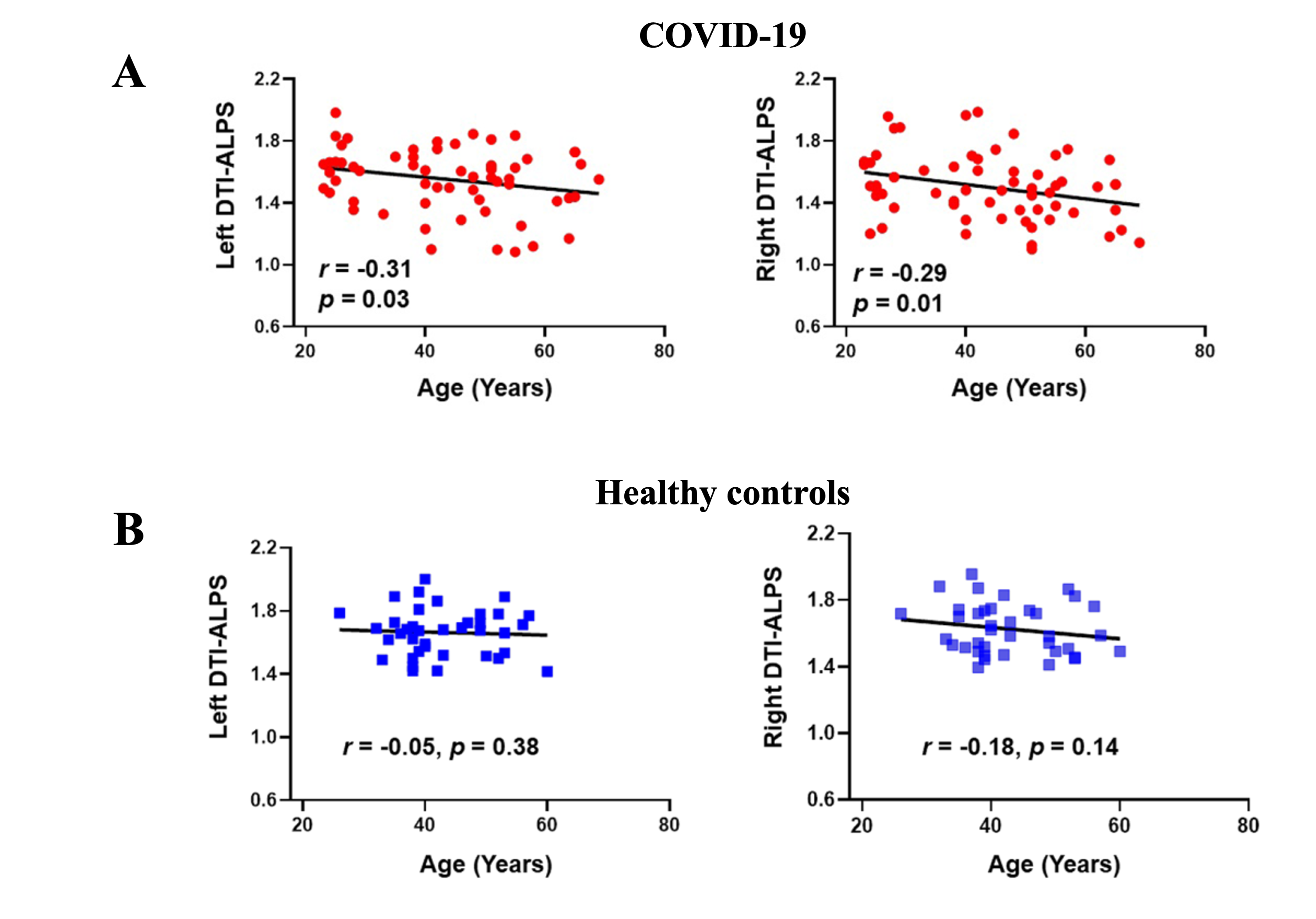
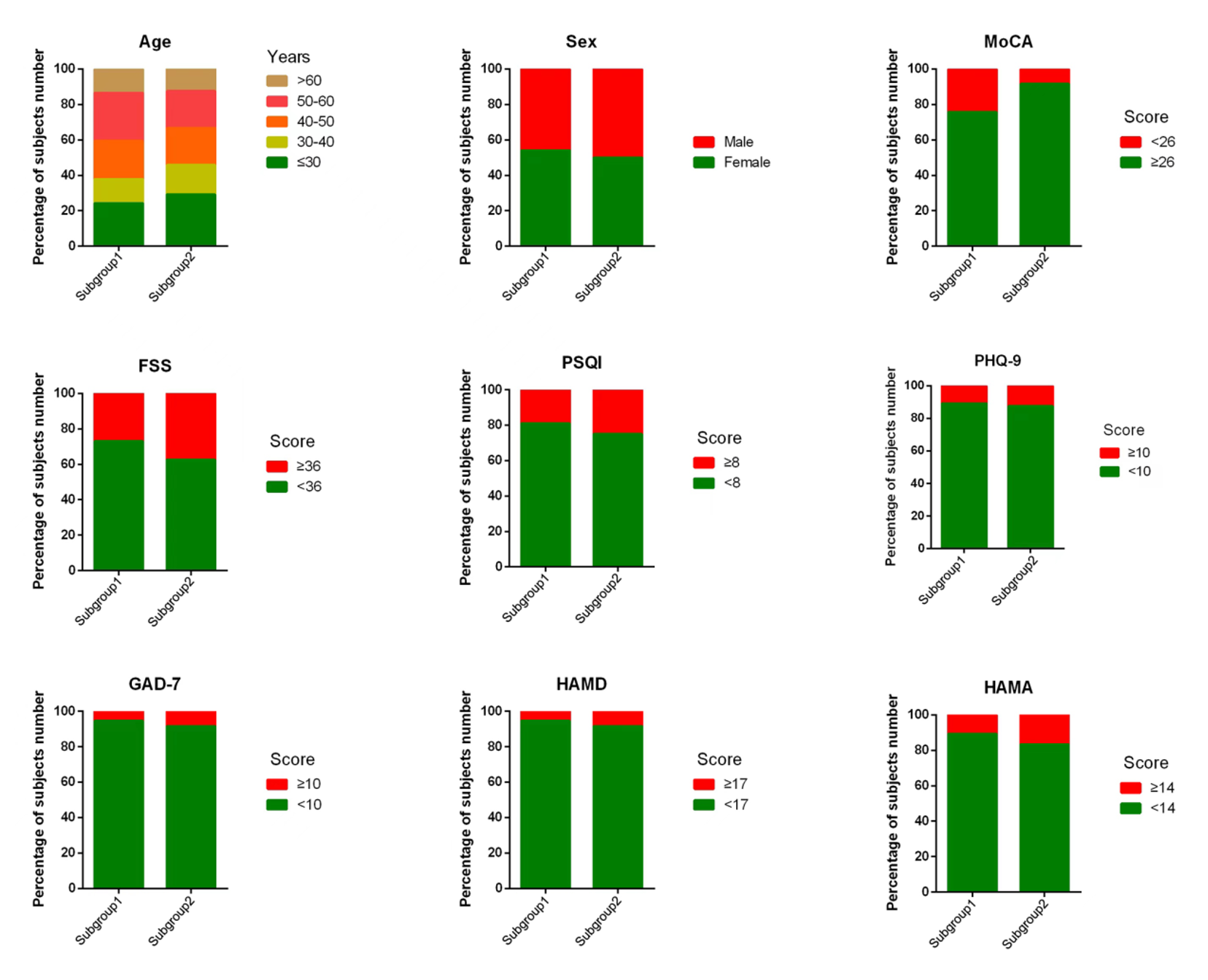
As shown in Figure 1, the left (1.54 vs. 1.66, P=0.001) and right (1.51 vs. 1.62, P=0.004) DTI-ALPS index in recovered COVID-19 patients was significantly lower than healthy controls. Furthermore, age was significantly correlated with the left (r=-0.307, P=0.016) and right DTI-ALPS index (r=-0.260, P=0.043) (Figure 2). Both left and right DTI-ALPS index was not significantly correlated with age (Figure 2; all P>0.05). After implementation of DTI-ALPS for hierarchical clustering in recovered COVID-19 patients, two clusters were identified: cluster 1 (n=37, 60.7%) and cluster 2 (n=24, 39.3%). Non-synergistic decline in the left and right DTI-ALPS index of cluster 2 (left 1.39 ± 0.20; right 1.60 ± 0.23) was more obvious than cluster 1 (left 1.66 ± 0.13; right 1.44 ± 0.18), and the proportion of poor cognitive scores was higher in cluster 2 (Figure 3). As shown in Table 1, the left DTI-ALPS index had significant effects on PSQI (reflecting sleep quality) and GAD-7 (reflecting anxiety status) in Subgroup 1. No significant effects were found in Subgroup 2 (data not shown).Discussion and Conclusion
In this study, we investigated the glymphatic function using DTI-ALPS. The results showed DTI-ALPS index is lower in recovered COVID-19 patients, which might reflect impairment of the glymphatic function. Douaudt et al. reported that the older the infected person is, the more severe the disease [5]. Our results showed the DTI-ALPS index was lower in older patients. Thus, it’s likely that older people infected with COVID-19 are more susceptible to impaired glymphatic system function. Hierarchical subgroup analysis showed that the decline of the DTI-ALPS index was non-synchronized in two hemispheres. Patients with a decreased right DTI-ALPS index showed a higher proportion of cognitive abnormalities. Future studies on cognitive impairment in older adults should rule out the effect of COVID-19 infection.In conclusion, this study provided evidence that the glymphatic function was declined in recovered COVID-19 patients which may related withsequelae.
Acknowledgements
No acknowledgement found.References
[1] Zhang H., Zang C., et al. Data-driven identification of post-acute SARS-CoV-2 infection subphenotypes. Nat Med. 2023; 29:226-235.
[2] Premraj L., Kannapadi N.V., et al. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J Neurol Sci. 2022; 434:120162.
[3] Wostyn P. COVID-19 and chronic fatigue syndrome: Is the worst yet to come? Med Hypotheses. 2021; 146:110469.
[4] Zhang W., Zhou Y., et al. Glymphatic clearance function in patients with cerebral small vessel disease. Neuroimage. 2021; 238:118257.[5] Douaud G., Lee S., et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature. 2022; 604:697-707.
Figures