2071
Segmentation of MRI White Matter Hyperintensities for longitudinal studies in CADASIL1Centre Neurovasculaire Translationnel, APHP, Paris, France, 2U1141 - Neurodiderot, INSERM, Paris, France, 3Université Paris-Cité, FHU NeuroVasc, Paris, France, 4Neurology, APHP, Paris, France
Synopsis
Keywords: White Matter, White Matter, CADASIL, WMH, longitudinal studies
Motivation: In CADASIL, the relationship between white matter hyperintensities (WMH) changes and disease progression remains unknown.
Goal(s): To estimate WMH changes, accurate segmentations are mandatory but remain challenging to obtain automatically because of patients MRI variability and heterogeneous contrast between WMH and normal appearing white matter. We aim to decrease correction time required to reach accurate results.
Approach: We used an incremental learning approach with a supervised algorithm from baseline segmentation data up to the final follow-up data to improve results and reduce manual correction time.
Results: A significant improvement of segmentation sensitivity and a reduction of manual correction time were obtained.
Impact: To accurately investigate the WMH progression in CADASIL, we propose an individual-based incremental training approach, with repeated learning of the segmentation algorithm from subsequent corrected data obtained along follow-up, to reduce the final manual correction time as much as possible.
Introduction
White Matter Hyperintensity (WMH) are a key MRI marker of cerebral Small Vessel Disease (cSVD). Their extent is strongly related to the clinical progression, particularly to the risk of stroke and cognitive decline [1]. CADASIL, a monogenic cSVD, is considered as an archetypal model of cSVD that can help understanding the complex mechanisms underlying the development of WMH of vascular origin [2]. Such imaging marker is one of the earliest manifestation of CADASIL and appears long before the occurrence of clinical symptoms. Even the total WHM load is not strongly related to the clinical severity, it is somehow related to clinical worsening [3-5]. Longitudinal studies of WMH in CADASIL are therefore crucial for preparing future treatment at early stage of the disease. Accurate delineation of these lesions is needed for longitudinal studies but automatic segmentation remains challenging because of the large variability, heterogeneous aspect and poor contrast between WMH and the normal appearing white matter (NAWM). Today, manual corrections are still mandatory to obtain hyper-accurate measures of WMH [6] but they are highly time-consuming. Herein, we propose a specific incremental training approach that can be used at individual level, based on successive learning of the algorithm from corrected data obtained along the follow-up, to reduce the final manual correction time as much as possible.Material & Methods
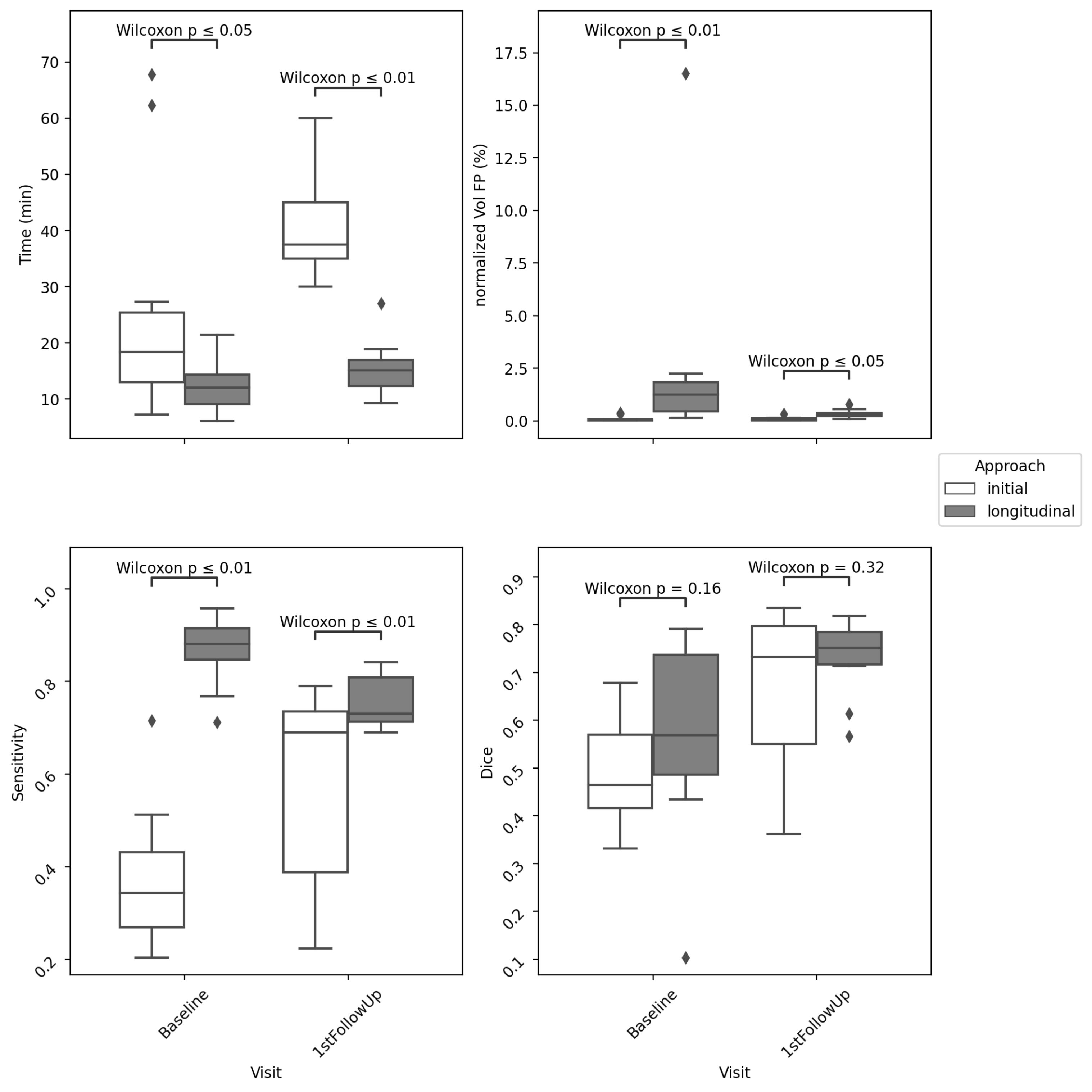
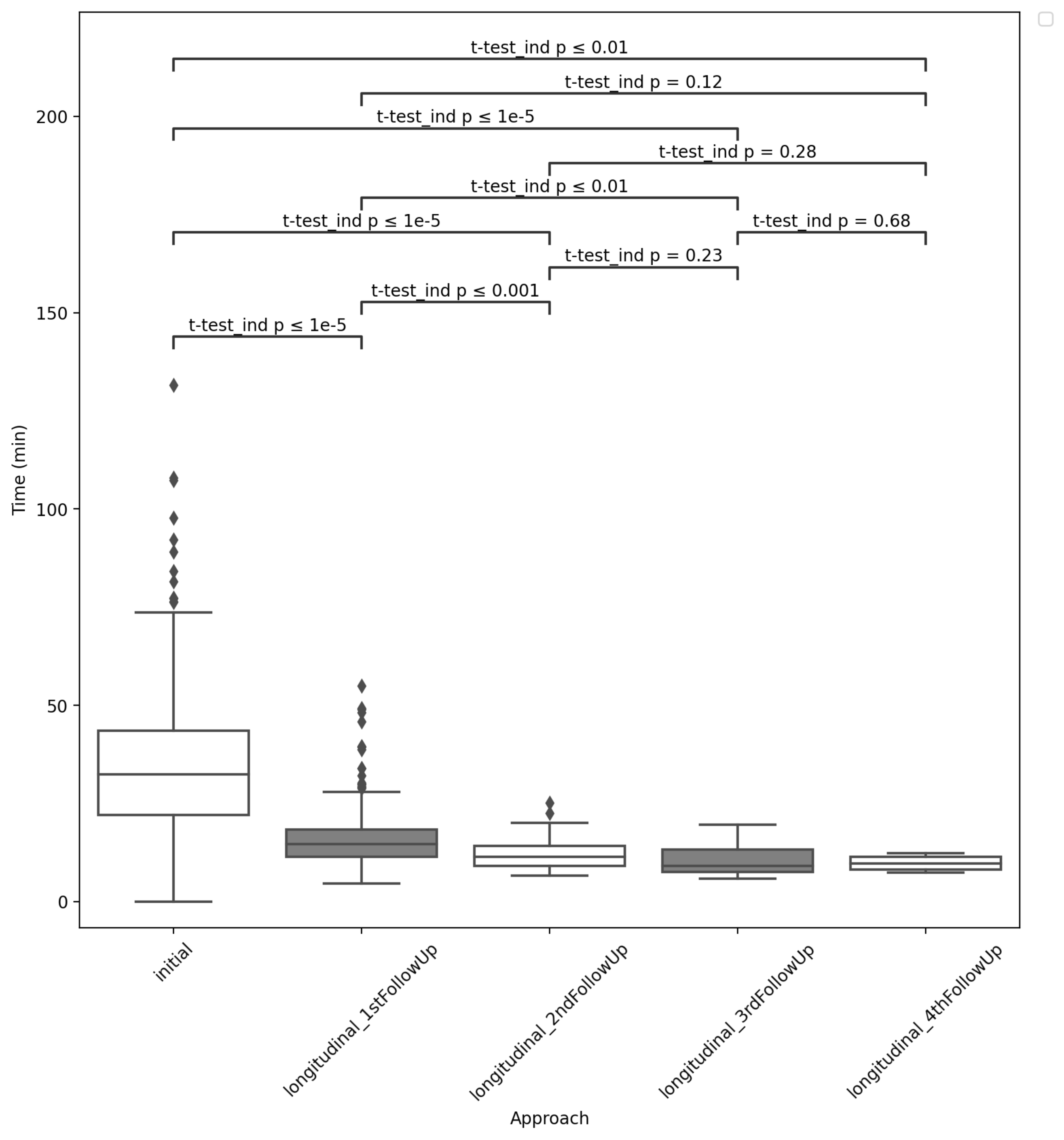
FLAIR and T1w-MRI were acquired on a 3T SIEMENS scanner on CADASIL patients followed every 2 years in the National French referral center for rare vascular diseases of the eyes and brain (CERVCO, https://www.cervco.fr). MRI data were bias corrected [7] and normalized for intensity range. WMH were first segmented from these data using the BIANCA algorithm (spatial weight set at 10, numbers of points included/excluded from the WMH masks set at 10000/40000)[6, 8, 9]. For 10 patients (mean age at inclusion: 39.1 +/- 7.1 yo), we designed two approaches: 1) for the ‘initial’ approach, we segmented the baseline and the 1st follow-up data using a training set of 20 WMH masks, manually delineated from high-resolute FLAIR data by an expert neuroradiologist and including various load of WMH [9]; 2) for the ‘longitudinal’ approach, we segmented again the data using a subject-specified training set including the corrected baseline (follow-up) mask associated with the baseline (follow-up) data and corrected mask registered to the follow-up (baseline) data to segment the follow-up (baseline) data. Each probability map was thresholded using a value automatically fixed from a clustering process and masks were manually corrected by a trained scientist. In addition to the time required for correction, we compared for both approaches, the False Positive volumes normalized by the corrected WMH volume, Sensitivity and the Dice scores computed between the automated and corrected masks, and final corrected WMH volumes. We also compared the WMH changes computed between corrected WMH volumes at baseline (initial approach) and at follow-up for both approaches. We then applied the initial approach to all baseline data available in the cohort (Nbaseline=421) and declined the longitudinal approach to available follow-up data (Nfollowup=271) with updating the subject-specific training set (for the 2nd follow-up we used the corrected baseline and 1st follow-up masks and so on). We then compared the subsequent correction times at the different steps of the process.Results
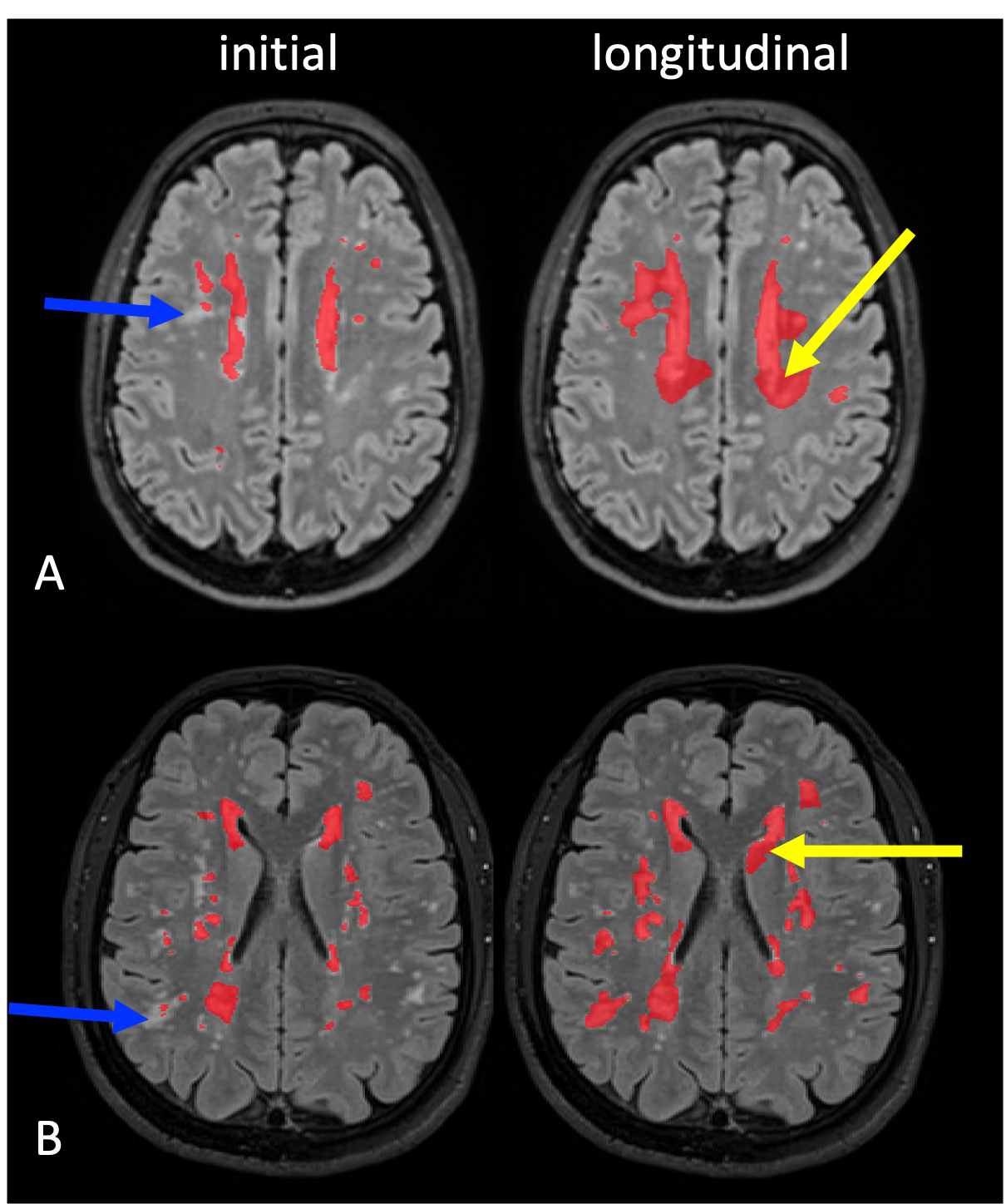
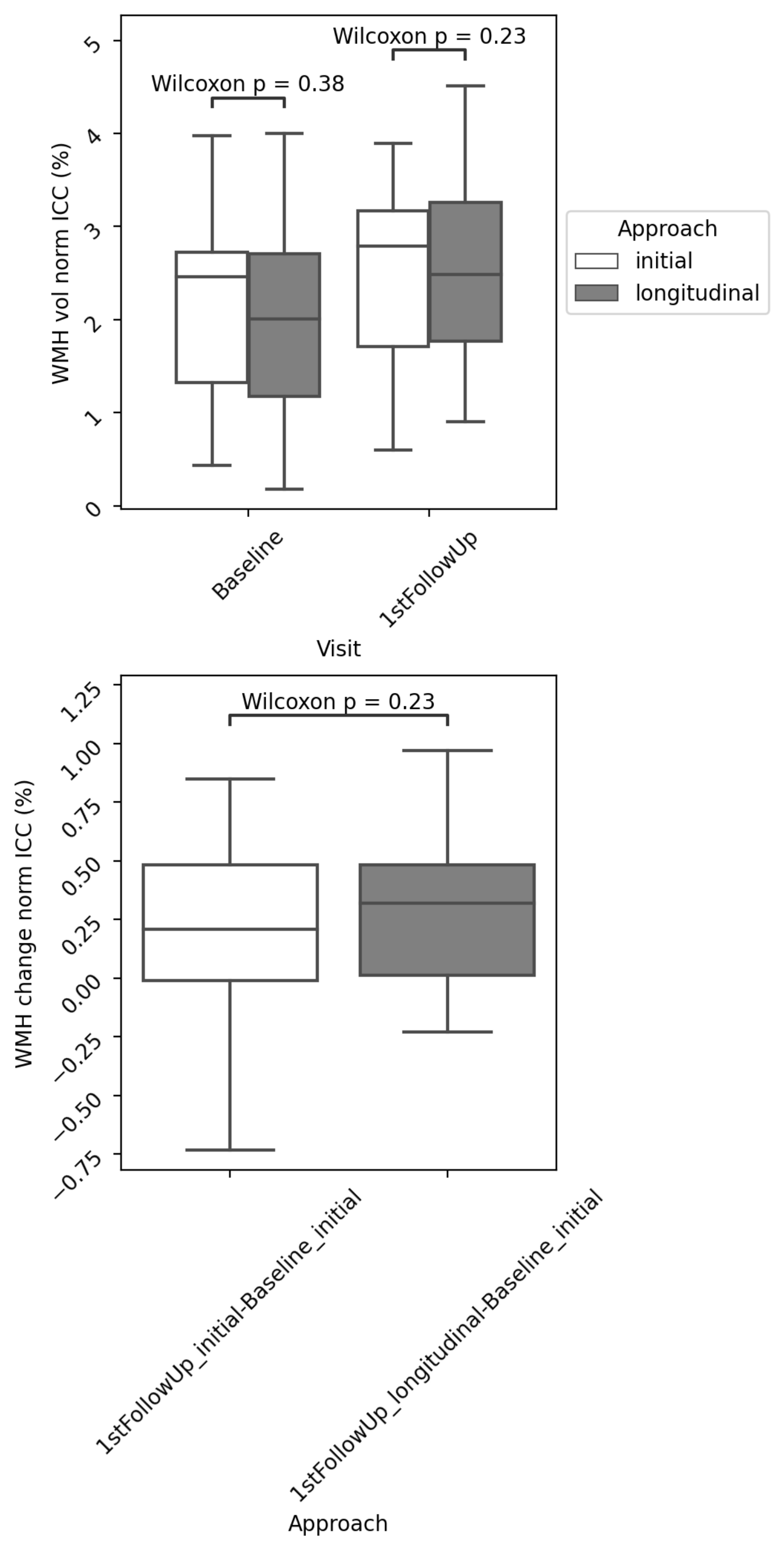
The longitudinal approach provided significantly more accurate masks, was less time consuming for manual corrections despite the detection of more false positive results (Figs1-2). Normalized WMH volumes obtained after manual corrections, and WMH changes estimated between visits were not significantly different between the different processing approaches (Fig3). Finally, correction times required when using the longitudinal approach were significantly lower than those observed with the initial approach and decreased considerably with the subsequent update of the follow-up training set (Fig4).Discussion & Conclusion
Our results show that repeated applications of a supervised segmentation algorithm along longitudinal data can help reduce considerably the correction time required to obtain hyper- accurate measures of WMH changes during the course of CADASIL. With repeated training of the algorithm using accurate subject data, we helped to learn from exact data with similar specificities, especially using the actual contrast between WMH and NAWM, and improved the sensitivity of results. The correction times were significantly reduced which is crucial for evaluating large datasets. This is crucial to investigate the variable progression of WMH among individuals and to analyze their predictors and long-term clinical impact.Acknowledgements
We thank the neuroradiology team of Lariboisière Hospital for MRI acquisitions and Dr Ruiting Zhang for the manual delineations of the high-resolute FLAIR data used for the initial approach. We thank very much Mr Abbas Taleb for collecting most of information along the cohort study and Mrs Nathalie Dias-Gastellier and Fanny Fernandes, the research managers in charge of the Cohort Study. We thank the CADASIL France Association for their help and permanent support and all patients and their relatives for their collaboration on this study.References
1. Lampe L, Kharabian-Masouleh S, Kynast J, Arelin K, Steele CJ, Löffler M, et al. Lesion location matters: The relationships between white matter hyperintensities on cognition in the healthy elderly , Lesion location matters: The relationships between white matter hyperintensities on cognition in the healthy elderly. J Cereb Blood Flow Metab. 2017:0271678X17740501.
2. Chabriat H, Joutel A, Tournier-Lasserve E, Bousser MG. CADASIL: yesterday, today, tomorrow. Eur J Neurol. 2020;27(8):1588-95.
3. Ouin E, Dimitrovic A, Grosset L, Lebenberg J, Guillonnet A, Guichard JP, et al. White Matter Hyperintensities of the Corpus Callosum Are Associated With Clinical Severity in CADASIL. Stroke. 2023;54(4):e138-e41.
4. Duchesnay E, Hadj Selem F, De Guio F, Dubois M, Mangin J-F, Duering M, et al. Different Types of White Matter Hyperintensities in CADASIL. Frontiers in Neurology. 2018;9.
5. Viswanathan A, Gschwendtner A, Guichard JP, Buffon F, Cumurciuc R, O'Sullivan M, et al. Lacunar lesions are independently associated with disability and cognitive impairment in CADASIL. Neurology. 2007;69(2):172-9.
6. Lebenberg JZ, Ruiting; Chabriat, Hugues, editor How to measure white matter hyperintensities in a long-term CADASIL cohort study? Annual Meeting of the Organization for Human Brain Mapping (OHBM); 2023; Montreal, Canada.
7. Tustison NJ, Avants BB, Cook PA, Zheng Y, Egan A, Yushkevich PA, et al. N4ITK: improved N3 bias correction. IEEE Trans Med Imaging. 2010;29(6):1310-20.
8. Griffanti L, Zamboni G, Khan A, Li L, Bonifacio G, Sundaresan V, et al. BIANCA (Brain Intensity AbNormality Classification Algorithm): A new tool for automated segmentation of white matter hyperintensities. NeuroImage. 2016;141:191-205.
9. Ling Y, Jouvent E, Cousyn L, Chabriat H, De Guio F. Validation and Optimization of BIANCA for the Segmentation of Extensive White Matter Hyperintensities. Neuroinform. 2018;16(2):269-81.
Figures