2062
Association between cerebral blood flow and cerebral small vessel disease: a comparison between ASL and phase-contrast MRI1The 2nd Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China, 2College of Biomedical Engineering & Instrument Science, Zhejiang University, Hangzhou, China
Synopsis
Keywords: White Matter, Brain
Motivation: Chronic hypoperfusion is a central mechanism of cerebral small vessel disease (CSVD), but studies using different methods have shown different results.
Goal(s): To compare the associations between CSVD and CBF measured by phase-contrast MRI and ASL in the same cohort.
Approach: 69 subjects were totally recruited in the study. WMH, FW, and tFA were used to reflect the disease severity. The associations between CSVD and CBF measured by two methods were investigated.
Results: Compared to CBFPC, CBFASL showed a negative association with FW and a positive association with tFA. The ratio of CBFASL to CBFPC was also correlated with FW and tFA.
Impact: Future studies need to consider the differences between CBF measured by ASL and phase-contrast MRI and choose a more appropriate method according to the research purpose.
INTRODUCTION
Cerebral small vessel disease (CSVD) is highly prevalent in older adults, and can significantly contribute to stroke and dementia1. Although its etiology has not been studied completely, chronic hypoperfusion has been considered a central mechanism. However, controversial results were reported regarding to the cerebral blood flow (CBF) in CSVD in large-scale studies2. Different associations with CSVD have been found using phase-contrast imaging and arterial spin labeling (ASL). One possible explanation is that CSVD is more associated with local CBF provided by ASL other than the global flow measured by phase contrast sequence. In this work, 69 participants were recruited to investigate the CSVD characters with the 4D phase-contrast MRI and ASL.METHODS
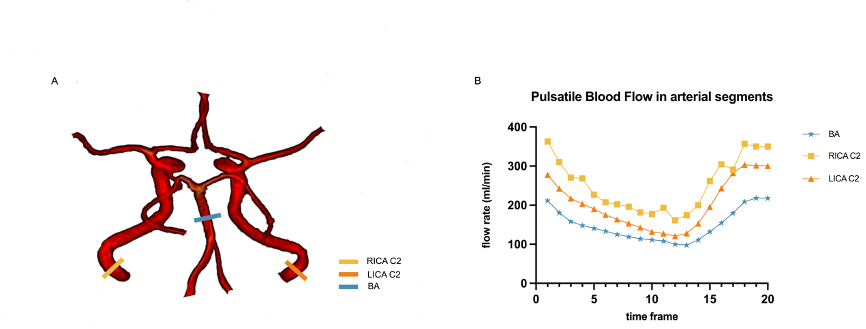
The study protocol has been approved by the ethics committee of the local hospital. Each subject went through full clinical assessments and multi-modal MRI performed on a United Imaging uMR790 3.0T scanner (Shanghai, China) with a 32-channel head coil. The parameters of 4D flow were: imaging volume = 224*170*60mm3, velocity encoding (venc) = 100cm/s, reconstructed voxel size= 1*1*0.75mm3, TR = 29.3 ms, TE = 4.09 ms, flip angle = 8°, scan time ~= 10 min. The ASL sequence used a 3D background-suppressed, multiple post-label delayed pseudo-continuous ASL scheme, with parameters: TR = 6141ms, TE = 13.86ms, PLD = 1500, 1800, 2100, 2400ms, voxel size = 3.5*3.5*4 mm3. ASL data were analyzed using the FMRIB Software Library (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki) and in-house software scripts. Brain tissues were segmented using CAT12 (https://neuro-jena.github.io/cat/). Flow analysis from 4D flow data was conducted in the cvi42 software (https://www.circlecvi.com/). The total CBFPC (tCBFPC, in mL/min) was calculated by adding CBF in the bilateral internal carotid artery C2 segments and the basilar artery (Figure 1). The tCBFPC was then normalized using total intracranial volume and average brain density from previous studies (ntCBFpc, mL/100g/min)3. The ratio between CBFASL and CBFPC was calculated. To reflect CSVD severity, white matter hyperintensity (WMH) volume normalized using intracranial volume, white matter free water (FW), and tissue fractional anisotropy (tFA)4 were calculated following the MarkVCID project (https://markvcid.partners.org/).The associations between CSVD and the CBF measured by the phase contrast and ASL were investigated including age, sex, vascular risk factors (VRFs, 0-4, including hypertension, hyperlipidemia, diabetes, and smoking), CBFPC, CBFASL, and CBF ratio respectively. Finally, a linear regression model was built, where the WMH volume, FW, and tFA were set as the dependent variables, and CBFPC, CBFASL, and CBF ratio as the independent variables separately, with age, sex, and VRF total score corrected. The p-value for statistical significance was set at 0.05, 2-tailed.
RESULTS
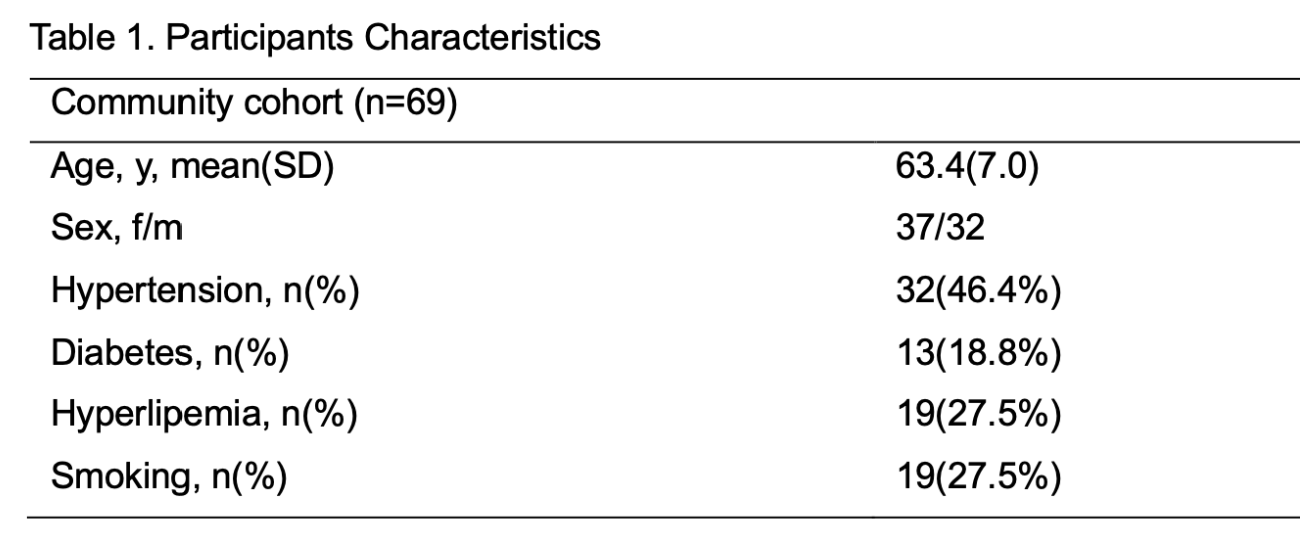
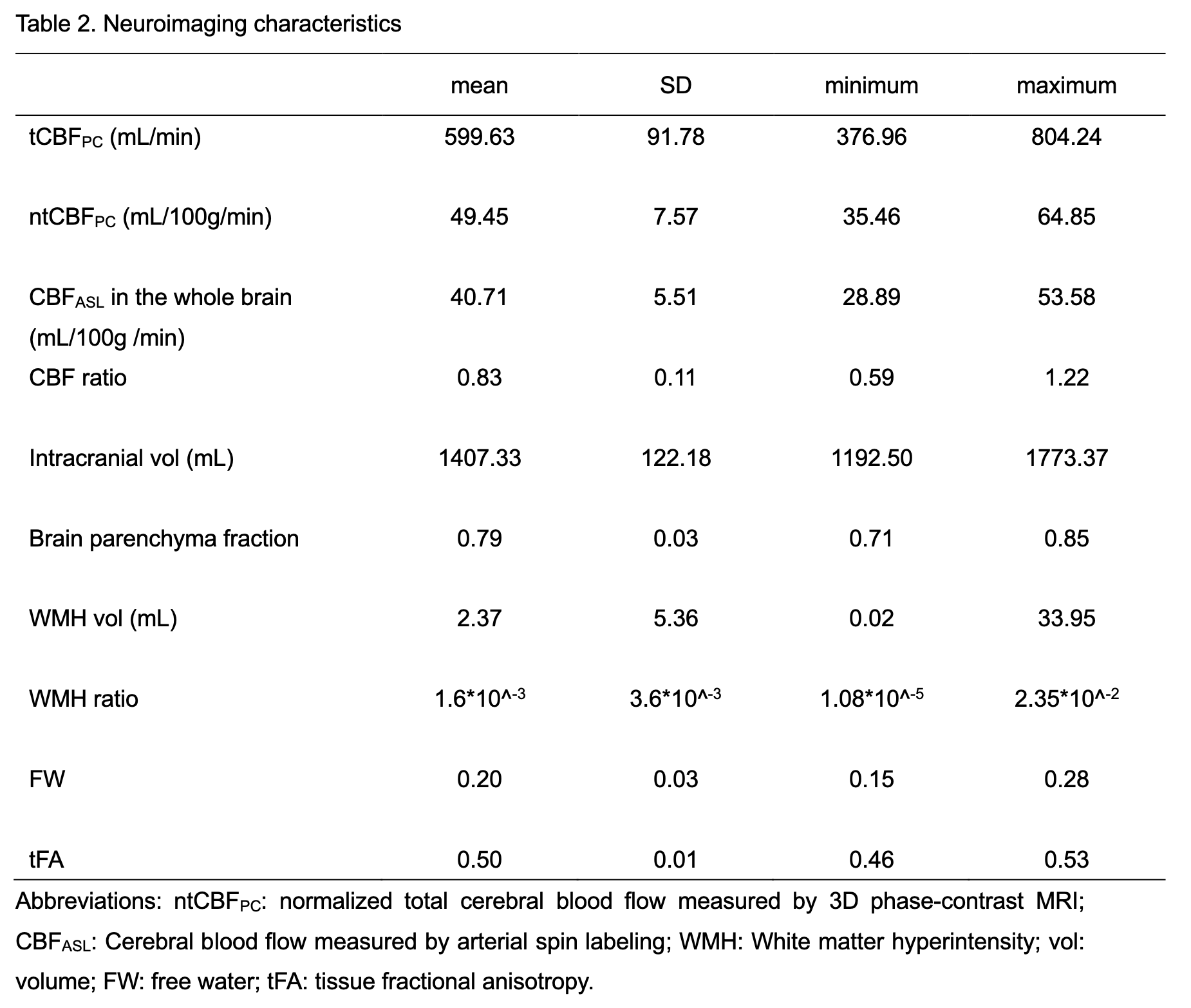
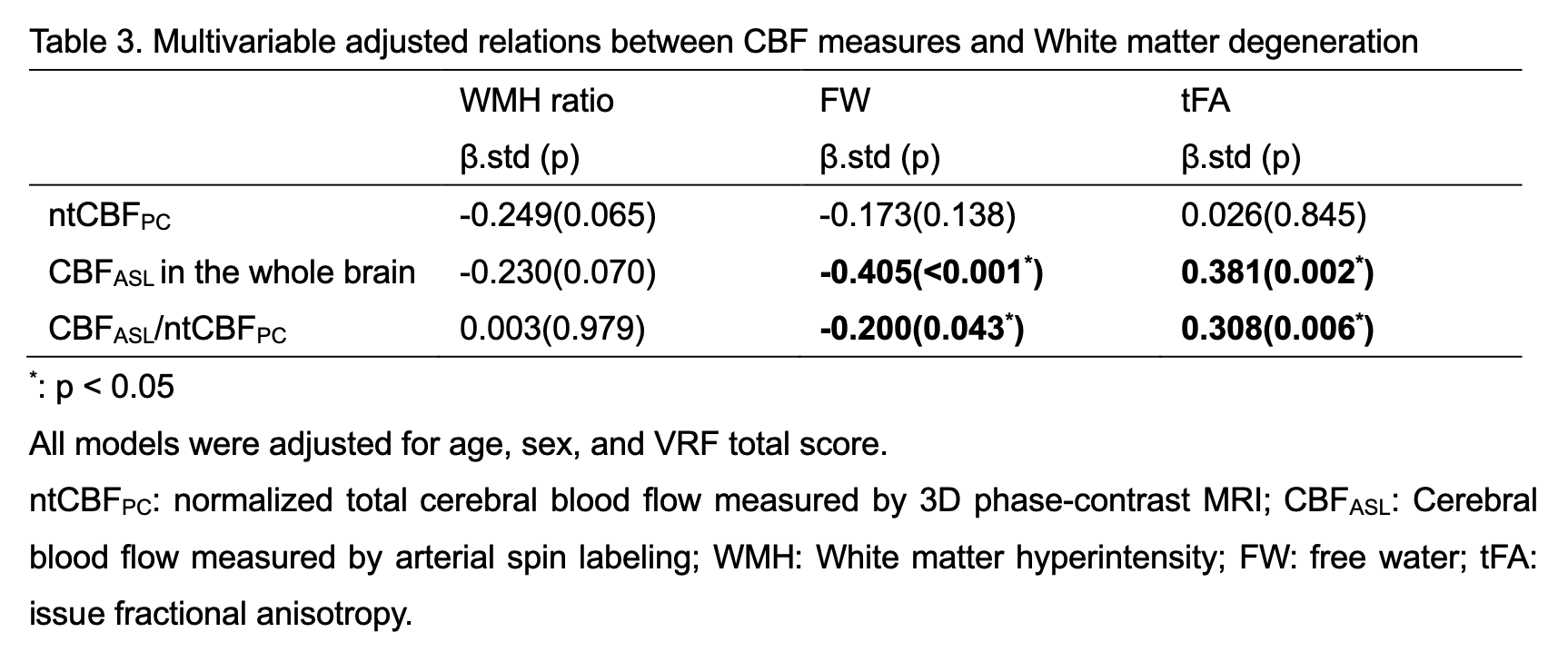
The demographic information of the participants was shown in Table 1 and the neuroimaging characteristics were presented in Table 2. A significant correlation between ntCBFPC and CBFASL was found in the whole brain (r = 0.577, p < 0.001). Compared to females, males had significantly lower ntCBFPC (53.21 vs 45.11, p < 0.001) and CBFASL in the whole brain (42.89 vs 38.22, p < 0.001). Importantly, CBFASL showed a negative association with FW and a positive association with tFA. ntCBFPC/CBFASL was also correlated with FW and tFA. However, ntCBFPC showed no association with WMH, FW, or tFA.DISCUSSION
FW and tFA are known features related to CSVD severity. CBF measured by ASL, but not 4D flow, showed significant associations with FW and tFA. These results confirmed our hypothesis and were consistent with previous studies. No significant association was observed between CBF and WMH volume, another common feature of the CSVD. It might be due to the relatively small sample size and low WMH burden in community subjects. Interestingly, the ratio between CBFASL and CBFPC was also associated with FW and tFA. The CBFPC reflects blood flowing into the brain cavity and the CBFASL reflects blood that reaches brain tissues. In CSVD, pathological changes, such as capillary dysfunction and thickened vessel walls, may hamper the transfer of blood from vessels to tissue and lead to decreased CBFASL. Therefore, a lower CBFASL/CBFPC may reflect more severe small vessel damages.CONCLUSION
CBFASL but not CBFPC showed significant associations with CSVD severity.Acknowledgements
Not applicable.References
1. Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010;9(7):689-701.
2. Shi Y, Thrippleton MJ, Makin SD, et al. Cerebral blood flow in small vessel disease: A systematic review and meta-analysis. J Cereb Blood Flow Metab. 2016;36(10):1653-1667.
3. Barber TW, Brockway JA, Higgins LS. The density of tissues in and about the head. Acta Neurol Scand. 1970;46(1):85-92.
4. Huang P, Zhang R, Jiaerken Y, et al. White Matter Free Water is a Composite Marker of Cerebral Small Vessel Degeneration. Transl Stroke Res. 2022;13(1):56-64.
Figures