2033
White Matter Damage and Myelin Loss in Rare PolyG Diseases: A 3T MRI Pilot Study1Department of Neuroradiology, National Neuroscience Institute, Singapore, Singapore, 2Duke-NUS Medical School, Singapore, Singapore, 3Department of Diagnostic Radiology, Singapore General Hospital, Singapore, Singapore, 4Department of Neurology, National Neuroscience Institute, Singapore, Singapore, 5Department of Diagnostic Radiology, Singapore General Hospital, SINGAPORE, Singapore, 6Department of Radiology, University of British Columbia, Vancouver, BC, Canada, 7Department of Pathology and Laboratory Medicine, University of British Columbia, Vancouver, BC, Canada, 8Department of Physics and Astronomy, University of British Columbia, Vancouver, BC, Canada, 9International Collaboration on Repair Discoveries (ICORD), University of British Columbia, Vancouver, BC, Canada
Synopsis
Keywords: White Matter, Diffusion/other diffusion imaging techniques, myelin, brain, myelin water imaging, diffusion
Motivation: Literature suggests that white matter (WM) may be specifically affected in polyG diseases, a novel class of genetic neurodegenerative diseases including fragile X-associated tremor/ataxia syndrome (FXTAS) and neuronal intranuclear inclusion disease (NIID).
Goal(s): To use advanced MRI to characterize WM in polyG disease.
Approach: 3T myelin water imaging and diffusion tensor imaging in participants with FXTAS and NIID.
Results: FXTAS and NIID demonstrated diffuse cerebral WM damage and myelin loss. Middle cerebellar peduncle (MCP) changes were seen in FXTAS, but not in NIID. Diffusion hyperintense foci in the MCP (FXTAS) and frontal WM (FXTAS and NIID) matched foci of highest dysmyelination.
Impact: Fragile X-associated tremor/ataxia syndrome and neuronal intranuclear inclusion disease show diffuse cerebral white matter abnormalities and myelin damage, and spatially differential changes in the frontal white matter and middle cerebellar peduncle.
Introduction
MRI is an important imaging modality for diagnosing polyglycine (polyG) diseases, a group of genetic neurodegenerative disorders1. polyG diseases are a new disease entity characterized by polyG protein deposits in the nucleus with a common genetic cause: CGG repeat expansions in the 5’UTR regions2. Fragile X-associated tremor/ataxia syndrome (FXTAS) and adult-onset neuronal intranuclear inclusion disease (NIID) are polyG diseases associated with major brain MRI features, including widespread white matter (WM) abnormalities, brain atrophy and bilateral middle cerebellar peduncle (MCP) signal changes3,4. Characteristic NIID MRI findings include curvilinear high signal at the grey-WM junction on isotropic diffusion-weighted imaging (DWI) and confluent WM hyperintensities, but there is some MRI overlap between these polyG diseases5-7. The underlying pathology of the various WM changes in polyG diseases (characterised by proteinaceous inclusion bodies within the nucleus) are not well understood. Our objective was to use quantitative and specific MRI, specifically myelin water imaging (MWI) and diffusion tensor imaging (DTI), to more indepthly characterize WM microstructural changes in polyG disease.Methods
Participants: This pilot study included a 62 year-old healthy control (HC) woman, a 65 year-old man with FXTAS (FMR1 gene positive), and a 61 year-old man with NIID (NOTCH2NLC gene positive).MRI: 3T brain MRI (Philips Ingenia) included 3D GRASE MWI (32 echo, TR/TE=1056/10-320ms, FA=90°, slices=40, slice thickness=5mm, matrix=240x240, FOV=230x230mm2, time=8.5min), DTI (TR/TE=6028/98ms, FA=90°, slices=50, slice thickness=3mm, matrix=144x144, FOV=240x240mm2, 15 diffusion-encoding directions each at 1000, 2000s/mm2 with 3 b=0 volumes, time=4.5 min), plus clinical FLAIR and DWI.
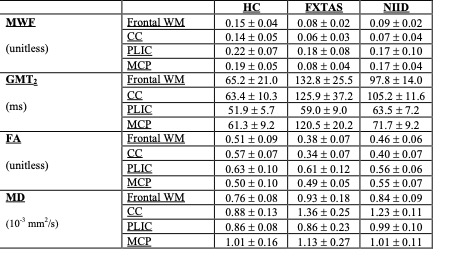
Analysis: MWI data was analysed using NNLS8 to determine myelin water fraction (MWF, fractional signal with T2 < 40ms) and geometric mean T2 (GMT2, mean 40<T2<200ms). Diffusion data was eddy current corrected and smoothed using a Gaussian kernel. DTI analysis yielded fractional anisotropy (FA), and mean, axial and radial diffusivity (MD, AD, RD)9,10. MWI and DTI metrics were extracted from manually drawn WM ROIs (genu of corpus callosum (CC), frontal WM, posterior limb of internal capsule (PLIC), middle cerebellar peduncle (MCP)).
Results
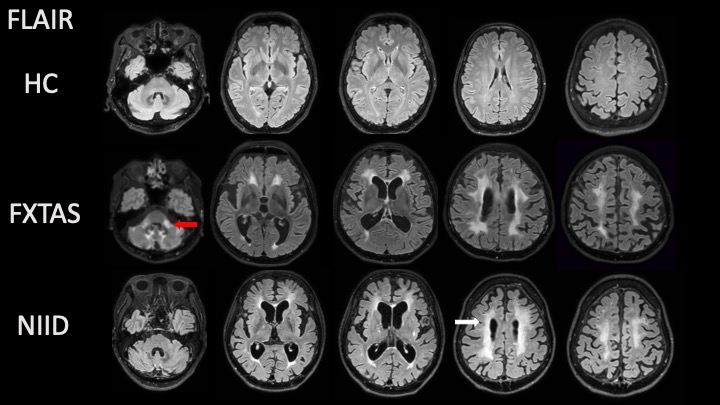
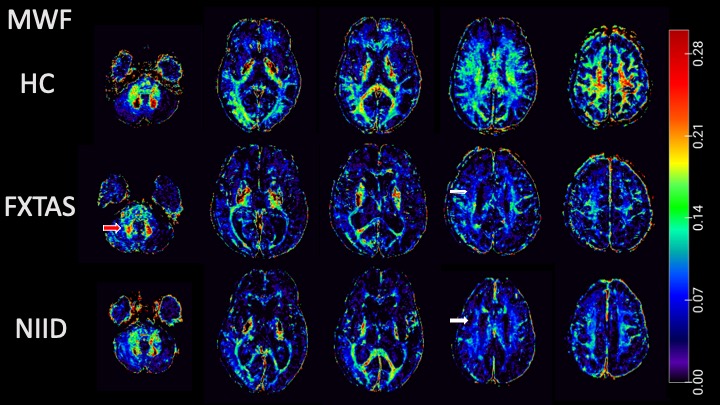
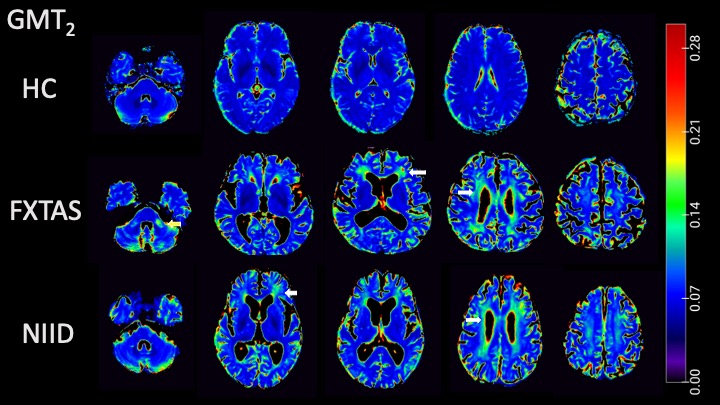
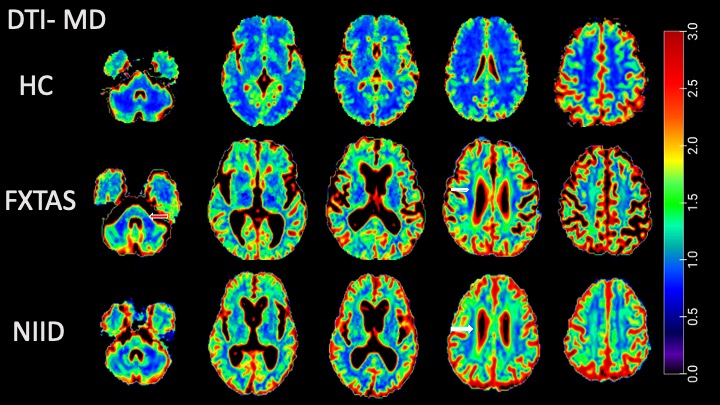
Diffuse volume atrophy, ventriculomegaly and bilateral confluent WM hyperintensity were qualitatively noted on FLAIR in FXTAS and NIID (Fig.1). On corresponding isotropic DWI, curvilinear hyperintensities were seen at the grey-WM junction in FXTAS and NIID. In FXTAS, FLAIR and DWI high signals were also noted in the MCP.Quantitatively, relative to control WM, MWI and DTI revealed decreased MWF and FA, and increased GMT2 and MD in cerebral WM of both FXTAS and NIID, including the frontal WM, CC and PLIC (Fig.2-4, Table 1). FXTAS showed decreased MWF in frontal WM (-46%), CC (-40%), PLIC (-18%) with similar decreases in NIID in frontal WM (-40%), CC (-50%), PLIC (-22%). FXTAS showed increased MD in frontal WM (+22%), CC (+54%), while NIID showed somewhat less MD increases in frontal WM (+10%), CC (+39%) and PLIC (+15%). MWI and DTI abnormalities in MCP WM were predominantly seen in FXTAS (-57% MWF and +11% MD for FXTAS versus -10% MWF and 0% MD for NIID). The diffusion hyperintense foci in the MCP (in FXTAS) and frontal grey-WM junction in both FXTAS and NIID matched foci of highest GMT2 (Fig.3). Increased diffusivity in respective regions of WM in FXTAS and NIID was also observed both in AD and RD.
Discussion
We demonstrated that generalised WM damage was detected and quantified in both FXTAS and NIID. The abnormalities detected on conventional FLAIR and DWI imaging in both polyG diseases are often non-specific, and do not provide insight into underlying pathophysiology. Therefore, we employed more advanced MRI, in particular MWI and DTI, to specifically look at WM microstructure. Consistent with prior DWI, DTI and conventional MRI literature, WM damage and loss of myelin were seen diffusely in the cerebral WM fibre tracts for both FXTAS and NIID4. However, changes in the MCP WM were noted in FXTAS, but not NIID. In addition, hyperintense foci on DWI in the MCP and frontal WM matched foci of highest dysmyelination in both FXTAS and NIID patients. We showed, for the first time, MWI and DTI characteristics of polyG diseases.Conclusion
Our findings suggest that the MCP could be a target of further investigation in FXTAS. In addition, GMT2 could serve as a useful quantitative surrogate biomarker to track severity or activity of WM damage in neuronal inclusion polyG diseases. This is the first study to use MWI in polyG disease. Advanced MRI techniques such as MWI and DTI may be helpful to elucidate the distinctive clinical and imaging phenotypes, and potentially to diagnose and monitor WM damage in this novel group of degenerative diseases.Acknowledgements
Our sincere thanks to Qian Hui Cheng, Wai Yung Yu, Zheyu Xu, and Zhiyong Chen for assistance with this study.References
1. Zhou ZD, Jankovic J, Ashizawa T, Tan EK. Neurodegenerative diseases associated with non-coding CGG tandem repeat expansions. Nat Rev Neurol. 2022;18(3):145-57.
2. Liufu T, Zheng Y, Yu J, Yuan Y, Wang Z, Deng J, et al. The polyG diseases: a new disease entity. Acta Neuropathol Commun. 2022;10(1):79.
3. Hagerman RJ, Hagerman P. Fragile X-associated tremor/ataxia syndrome - features, mechanisms and management. Nat Rev Neurol. 2016;12(7):403-12.
4. Brown SS, Stanfield AC. Fragile X premutation carriers: A systematic review of neuroimaging findings. J Neurol Sci. 2015;352(1-2):19-28.
5. Sugiyama A, Sato N, Kimura Y, Maekawa T, Enokizono M, Saito Y, et al. MR Imaging Features of the Cerebellum in Adult-Onset Neuronal Intranuclear Inclusion Disease: 8 Cases. AJNR Am J Neuroradiol. 2017;38(11):2100-4.
6. Sone J, Mori K, Inagaki T, Katsumata R, Taka gi S, Yokoi S, et al. Clinicopathological features of adult-onset neuronal intranuclear inclusion disease. Brain. 2016;139(Pt 12):3170-86.
7. Yu WY, Xu Z, Lee HY, Tokumaru A, Tan JMM, Ng A, et al. Identifying patients with neuronal intranuclear inclusion disease in Singapore using characteristic diffusion-weighted MR images. Neuroradiology. 2019;61(11):1281-90.
8. Prasloski T, Madler B, Xiang QS, MacKay A, Jones C. Applications of stimulated echo correction to multicomponent T2 analysis. Magn Reson Med. 2012;67(6):1803-14.
9. Andersson JLR, Sotiropoulos SN. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage. 2016;125:1063-78.
10. Tabesh A, Jensen JH, Ardekani BA, Helpern JA. Estimation of tensors and tensor-derived measures in diffusional kurtosis imaging. Magn Reson Med. 2011;65(3):823-36.
Figures