2027
Optimizing velocity-selective inversion pulses for improved labeling efficiency and robustness1Bioengineering, University of California Riverside, Riverside, CA, United States
Synopsis
Keywords: Arterial Spin Labelling, Arterial spin labelling
Motivation: Current Fourier Transform-based velocity-selective inversion (VSI) pulses are sensitive to field inhomogeneities, leading to labeling errors or inefficiency.
Goal(s): To improve the labeling robustness and efficiency of the VSI pulses for more robust and high-SNR perfusion measurement.
Approach: A new design with 6-segment FT-VSI pulse was implemented and tested in healthy subjects using dual-module VSI labeling.
Results: Compared with the existing VSI pulse, the new pulse significantly improved the labeling robustness against field inhomogeneities and the overall labeling efficiency, leading to >15% higher ASL signal (p<0.0002) and >20% higher temporal SNR (p<0.009).
Impact: This new VSI pulse can effectively improve the labeling robustness against field inhomogeneities, while increasing the labeling efficiency and reducing the SAR. These features are especially beneficial with dm-VSASL implementation and in ultra-high field applications for delay-insensitive ASL perfusion imaging.
Introduction
Velocity-selective arterial spin labeling (VSASL) 1, 2, especially those inversion based labeling methods 3, 4, holds great promise in imaging perfusion without the sensitivity to arterial transit artefacts. Current velocity-selective inversion (VSI) pulses are mainly based on the Fourier Transform (FT) principles 5, 6, and implemented with hard RF pulses that exhibit sensitivities to field inhomogeneities 3, 4, 7. Methods, such as applying phase cycling to the RF pulses 3, 8, help improve the robustness, but are not designed to improve the labeling efficiency.Methods
The labeling efficiency of VS pulses are attenuated by the T2 relaxation during the pulses, i.e. e-eTE/T2a, where eTE is the effective echo time of the labeling pulse and T2a is the T2 of arterial blood. The T2 relaxation can be reduced by shortening the eTE, for example, by applying a sinc-shaped modulation (sinc-VSI) on the rectangular-shaped VSI pulse (rect-VSI) of the same length 4, 7. Current implementation of FT-VSI pulses, including rect-VSI 3 and sinc-VSI 4, consist of 8 repeated segments of a small-flip-angle RF and a pair of composite 180° refocusing pulses, and a small-flip-angle (SFA) RF pulse at the end. The 180° pulses use a MLEV-16 phase cycling pattern to reduce its B1 sensitivity 3.Using less segments in the VSI labeling pulse can reduce the eTE, and therefore, improve its labeling efficiency. In addition, a shorter VSI pulse duration may potentially improve its robustness against motion and field inhomogeneities, and can reduce the SAR. In this study, we designed a 6-segmented FT-VSI pulse, with the flip-angles of the 7 SFA pulses to be (11.6°, 24.5°, 34.7°, 38.5°, 34.7°, 24.5°, 11.6°) for sinc-VSI (and 25.7° each for rect-VSI), and an (MLEV-8 + MLEV-4) phase-cycling scheme.
The performance of the new VSI pulses were evaluated in vivo with dual-module VSASL (dm-VSASL) 7. Five healthy subjects (1 female, age 25-40) were scanned on a 3T scanner (Siemens Prisma, Erlangen, Germany) under an IRB approval. The labeling parameters included: 1) PCASL 9 as a reference: LD/PLD=1.8/1.8s; dm-VSI (TI1/TI2=1.45/0.55s, PLD=0.03s) with 2) 8-segment sinc-VSI; and 3) 6-segment sinc-VSI. Other imaging parameters included: single-shot 3D GRASE EPI readout with GRAPPA 10 (x2 PE acceleration), FOV=220x220mm (64x64), 24 slices, 4mm thickness, TR/TE=5s/21.4ms, 20 label/control pairs, cutoff velocity=2cm/s along S/I in VSASL. Fully relaxed M0 and T1w anatomical images were acquired.
The ASL signals were obtained after complex image reconstruction and pair-wise subtraction, and then normalized by the M0 image. Temporal SNR (tSNR) 11 of the ASL signal was estimated. Gray matter (GM) and white matter (WM) regions of interest were obtained from the co-registered anatomical images using FSL 12. The ASL signal and tSNR in GM and WM were compared between 8-segment and 6-segment VSI using paired t-tests.
Results
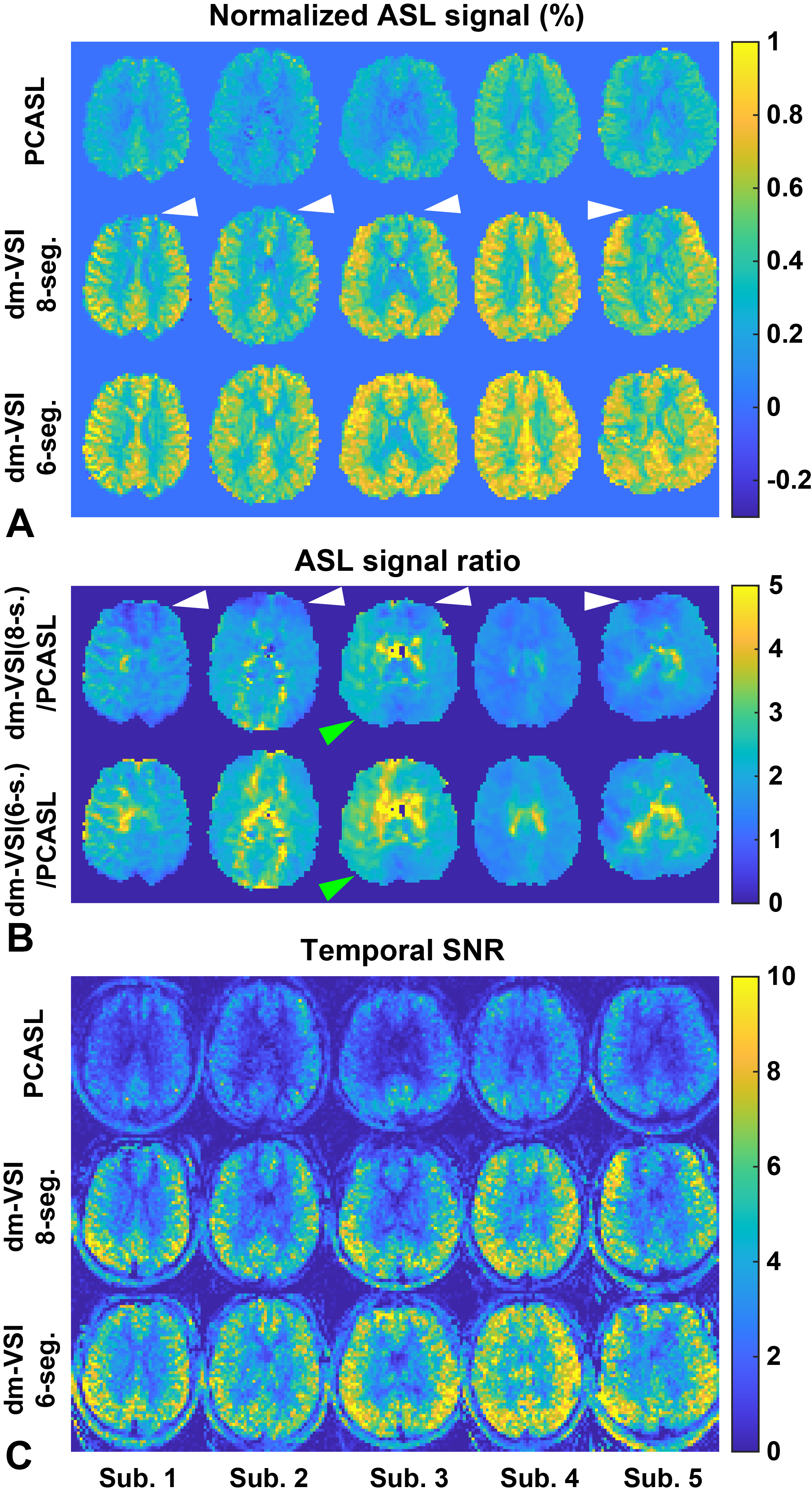
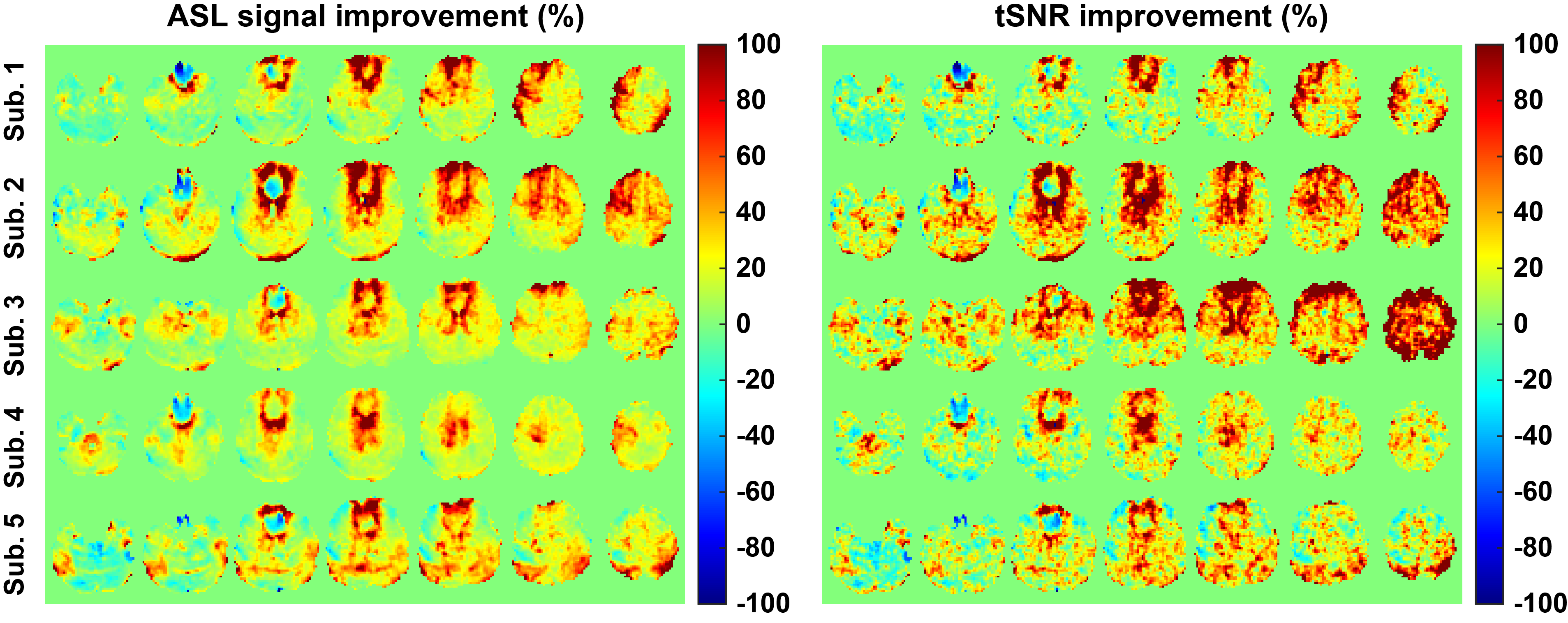
The normalized ASL signal, the ratio of the ASL signals between dm-VSI and PCASL, and the tSNR maps are shown in Figure 1. Compared to 8-segment dm-VSI, notable ASL signal and labeling efficiency improvement can be observed in regions with compromised field homogeneities with 6-segment dm-VSI, and was more evident in the ratio maps when compared with PCASL (Figure 1B), and in the tSNR maps. In addition, higher ASL signals were observed throughout the brain with 6-segment dm-VSI with reduced eTE.The percentage improvement of 6-segment vs. 8-segment dm-VSI are shown in Figure 2. The ASL signal and tSNR were improved throughout the brain, especially in the regions with field inhomogeneities.
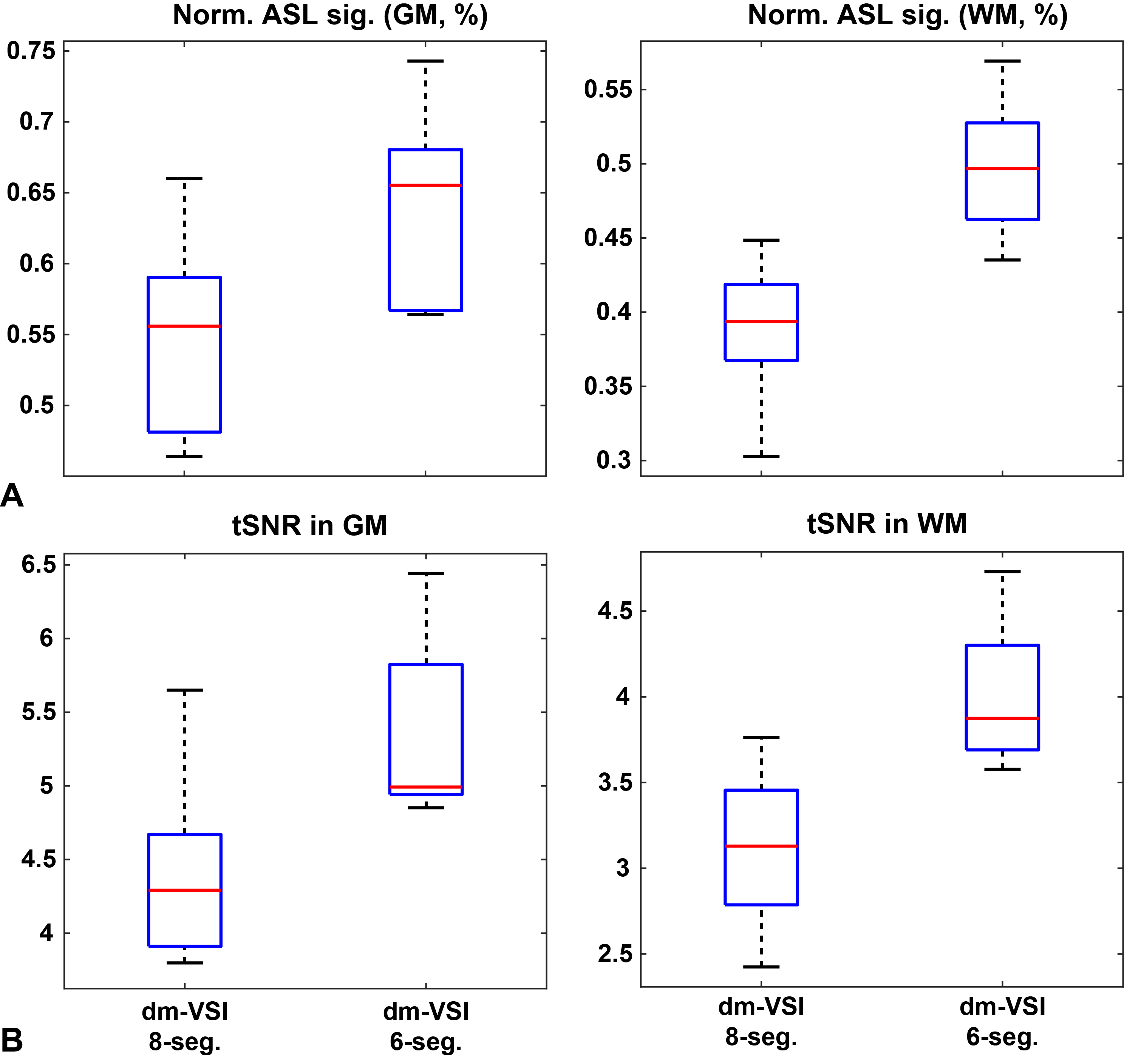
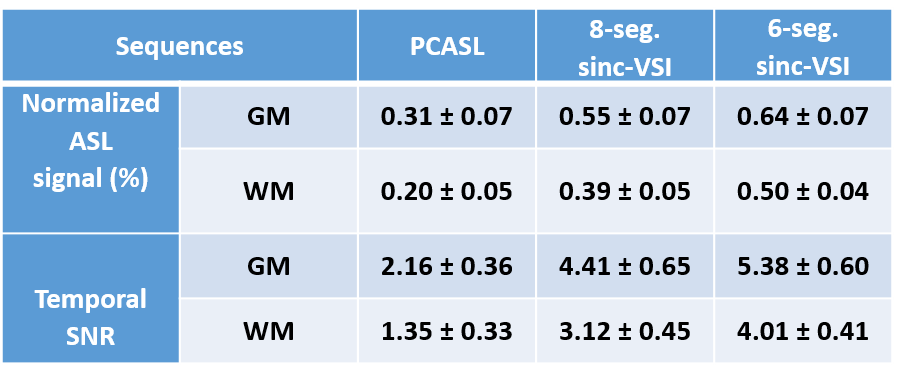
Averaged normalized ASL signals and tSNR across the subjects are shown in Figure 3 and Table 1. Compared to 8-segment VSI, 6-segment VSI improved the ASL signal by 17.0±3.3% in GM (p=0.0001) and 28.7±7.7% in WM (p=0.0002), and improved the tSNR by 23.0%±11.7 in GM (p=0.009) and 29.9±9.9% in WM (p=0.0006).
Discussion
Demonstrated by the in vivo results, this simple modification can effectively improve the labeling robustness against field inhomogeneities, while increasing the labeling efficiency by shortening the eTE, and reducing the SAR. These features are especially beneficial with dm-VSASL implementation and in ultra-high field applications.Similar improvements were observed with the 6-segment design when implemented with rect-VSI pulses (results not shown), but the ASL signals were lower due to a longer eTE. Four-segment implementation was also experimented, but the initial results showed compromised labeling robustness. Further optimization of the FT-VSI pulses is needed, including the sensitivity to eddy currents and diffusion.
The dynamic phase-cycling scheme 8 can be applied with the proposed 6-segment VSI to further improve its robustness, but at the expense of reduced temporal resolution.
Conclusion
6-segment FT-VSI can significantly improve the labeling efficiency and robustness of VSI labeling.Acknowledgements
This work was supported by National Institutes of Health, R01EB033210.References
1. Wong EC, Cronin M, Wu W-C, Inglis B, Frank LR, Liu TT. Velocity-selective arterial spin labeling. Magn Reson Med. 2006;55(6):1334-41.
2. Qin Q, Alsop DC, Bolar DS, Hernandez-Garcia L, Meakin J, Liu D, et al. Velocity-selective arterial spin labeling perfusion MRI: A review of the state of the art and recommendations for clinical implementation. Magn Reson Med. 2022;88(4):1528-47.
3. Qin Q, van Zijl PC. Velocity-selective-inversion prepared arterial spin labeling. Magn Reson Med. 2016;76(4):1136-48.
4. Guo J, Das S, Hernandez-Garcia L. Comparison of velocity-selective arterial spin labeling schemes. Magn Reson Med. 2021;85(4):2027-39.
5. Pauly J, Nishimura D, Macovski A. A k-space analysis of small-tip-angle excitation. J Magn Reson. 1989;81(1):43-56.
6. Norris DG, Schwartzbauer C. Velocity Selective Radiofrequency Pulse Trains. J Magn Reson. 1999;137:231-6.
7. Guo J. Robust dual-module velocity-selective arterial spin labeling (dm-VSASL) with velocity-selective saturation and inversion. Magn Reson Med. 2023;89(3):1026-40.
8. Liu D, Li W, Xu F, Zhu D, Shin T, Qin Q. Ensuring both velocity and spatial responses robust to B 0 / B 1 + field inhomogeneities for velocity-selective arterial spin labeling through dynamic phase-cycling. Magn Reson Med. 2021;85(5):2723-34.
9. Dai WY, Garcia D, de Bazelaire C, Alsop DC. Continuous Flow-Driven Inversion for Arterial Spin Labeling Using Pulsed Radio Frequency and Gradient Fields. Magn Reson Med. 2008;60(6):1488-97.
10. Griswold MA, Jakob PM, Heidemann RM, Nittka M, Jellus V, Wang J, et al. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn Reson Med. 2002;47(6):1202-10.
11. Murphy K, Bodurka J, Bandettini PA. How long to scan? The relationship between fMRI temporal signal to noise ratio and necessary scan duration. Neuroimage. 2007;34(2):565-74.
12. Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TEJ, Johansen-Berg H, et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage. 2004;23:S208-S19.
Figures