2026
Theoretical and experimental optimization of random vessel-encoded ASL to improve vascular territorial mapping and CBF quantification1Biomedical Engineering, Northwestern University, Evanston, IL, United States, 2Radiology, Northwestern University, Chicago, IL, United States
Synopsis
Keywords: Arterial Spin Labelling, Arterial spin labelling
Motivation: Planning-free random vessel-encoded ASL (rVE-ASL) greatly simplifies the vessel-selective ASL scan settings and shows great potential for vascular territorial imaging in clinical applications.
Goal(s): To theoretically and experimentally optimize rVE-ASL to establish an efficient and reliable rVE-ASL protocol
Approach: Simulation and in-vivo experiments were conducted to evaluate and optimize rVE-ASL in terms of labeling efficiency, total number of encoding steps, and reliability of vascular territorial and CBF measurements.
Results: Reliable territorial mapping and CBF measurements from both ICA and VA can be achieved by optimized rVE-ASL. At least 20 encoding steps are needed to achieve reliable territorial mapping and CBF measurements in rVE-ASL.
Impact: We have theoretically and experimentally optimized rVE-ASL, which can provide reliable vascular territorial mapping and CBF quantification. The rVE-ASL technique holds a potential to be a useful imaging tool for assessing vascular territorial alterations and collaterals in various clinical applications.
INTRODUCTION
Characterizing cerebral vascular territories is clinically important, particularly in the assessment of cerebrovascular disorders, such as collateral evaluation in steno-occlusive disease. Vessel-selective arterial spin labeling (VS-ASL) is an attractive non-invasive MRI technique that enables vascular territorial mapping from individual feeding arteries. Nevertheless, the clinical implementation of VS-ASL has been hindered by its operational complexity during the scan setup. Recently, a planning-free random vessel-encoded ASL (rVE-ASL) has recently been introduced to greatly simplify the VS-ASL scan settings, thus showing great potential for clinical applications. In this work, we aim to both theoretically and experimentally optimize rVE-ASL, in terms of labeling efficiency, vascular territory mapping, and CBF quantification with a goal of establishing a reliable rVE-ASL protocol for potential clinical applications.METHODS
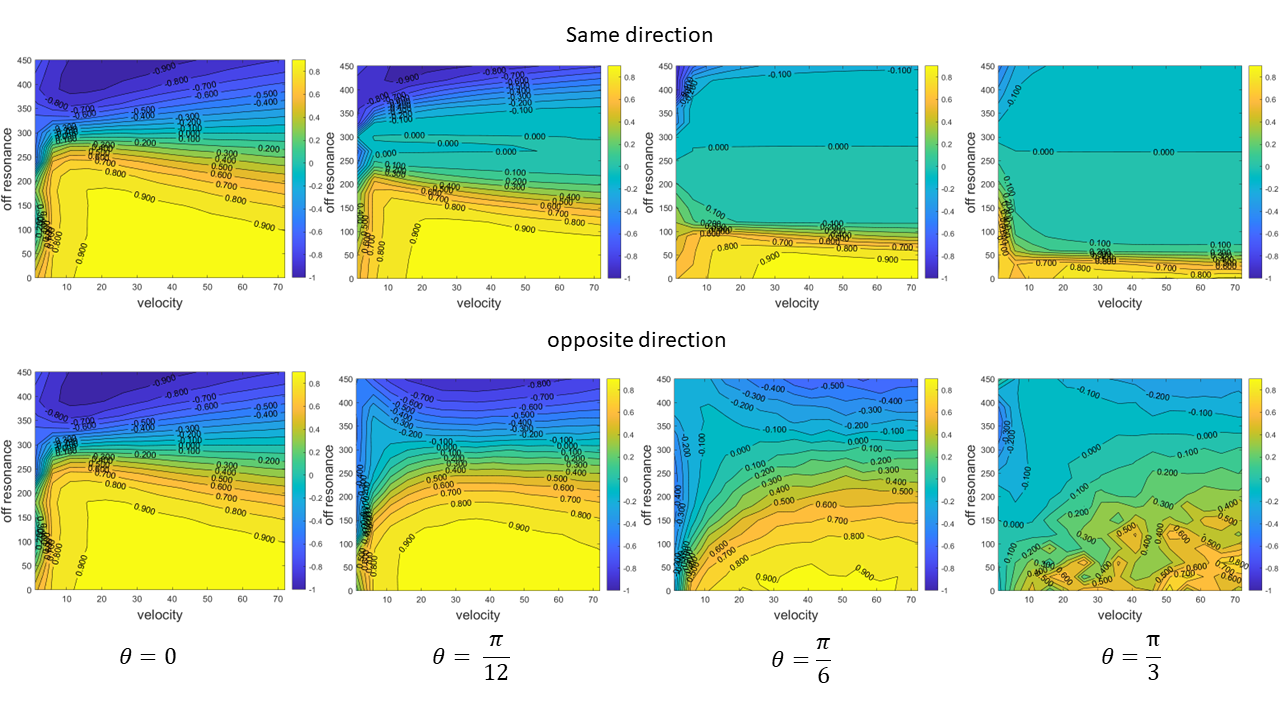
SimulationsFlow driven inversion was simulated using hard pulse approximation of the Bloch equations for rVE-ASL sequence using a step size = 4 μs considering the conditions of the labeled vessel is or is not perpendicular to the labeling plane. Simulations were performed for off-resonance phase shifts from 0Hz to 420Hz and velocity from 0 to 72cm/s.
In vivo imaging
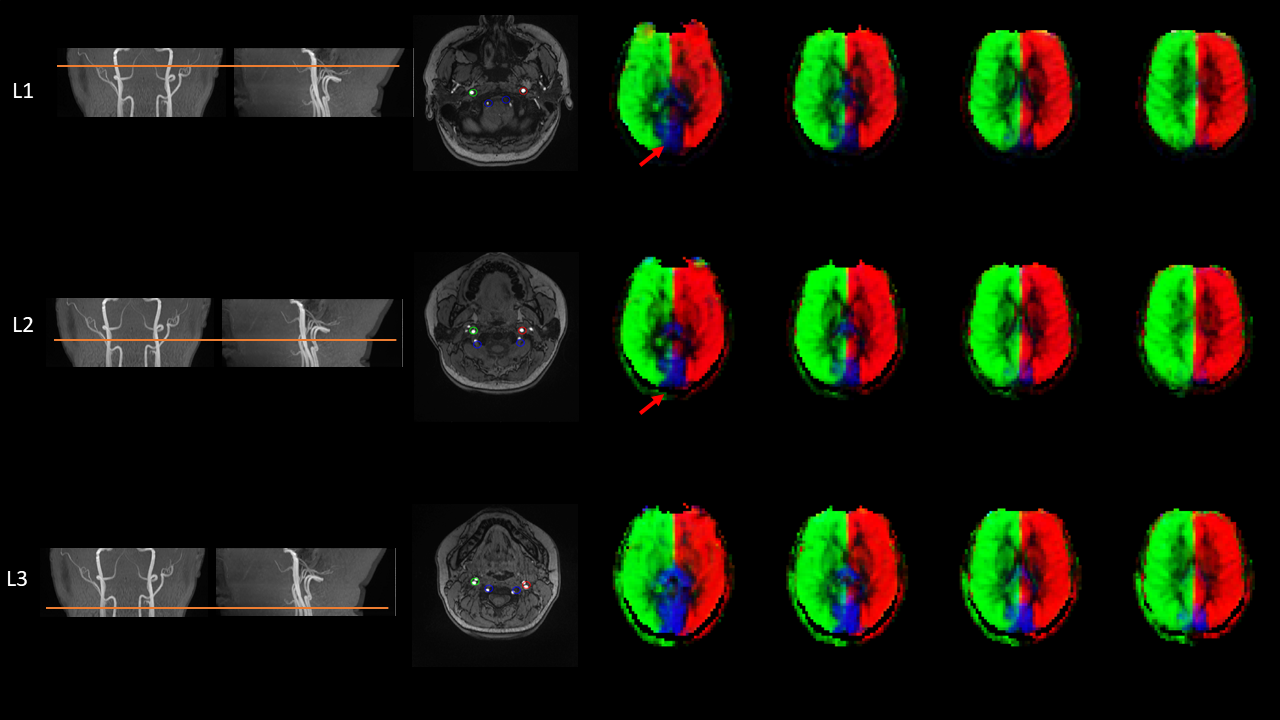
In-vivo MRI experiments were conducted on a Siemens Prisma 3T MRI scanner. Three rVE-ASL scans with different labeling planes were performed on 7 participants using identical imaging parameters, including FOV= 220×220 mm2, matrix size=64×64, TE/TR=36/4000ms, 12 slices with slice thickness of 8mm, 60 pairs of encoding steps with random orientation, phase and wavelength were acquired with two additional pairs of global label/control. Three labeling planes were chosen based on the TOF angiogram (as shown in Figure 2 in the result section). For CBF comparison, conventional pCASL scans with the same spatial coverage (24 slices with 4mm slice thickness) and same labeling planes were also performed. The locations of feeding arteries and corresponding territories were identified by dictionary matching. CBF was calculated by single-compartment model.
RESULTS and DISCUSSION
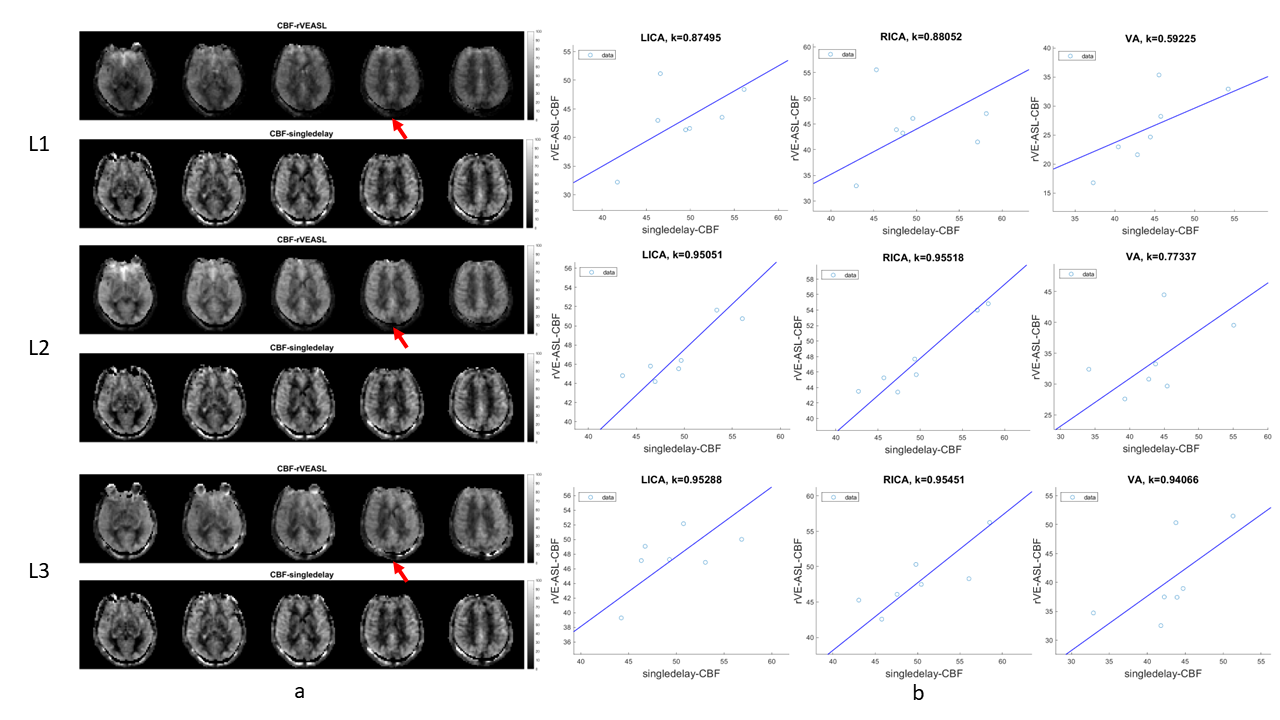
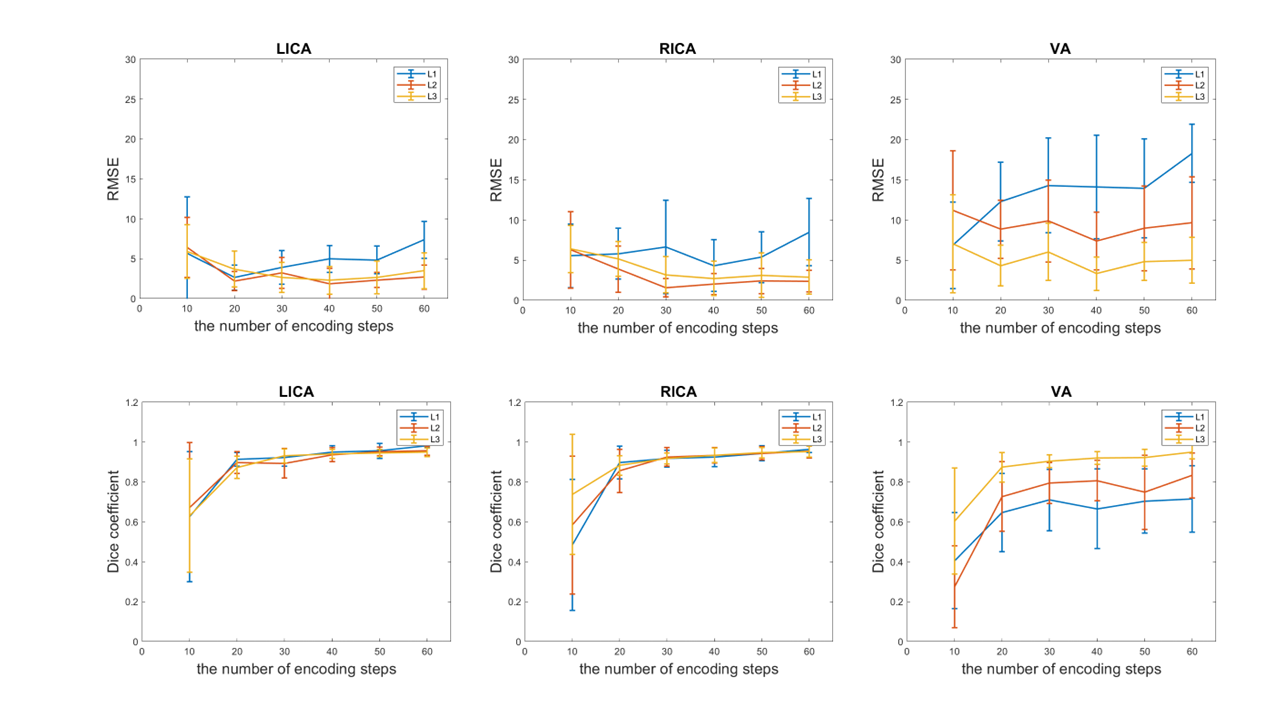
Bloch simulations (Figure 1) reveal that the behavior of inflowing spins in the VE-ASL closely resembles that in the conventional pCASL when the target vessel is perpendicular to the labeling plane (q=0). However, when the vessel is tilted towards transverse plane in both directions, the labeling efficiency quickly drops when the titled angle was greater than 30o. The simulations indicate that the labeling efficiency of VE-ASL is sensitive to the selection of labeling planes. Figure 2 shows the vascular territory mapping obtained by rVE-ASL at three labeling planes (L1, L2, and L3). The territories of left and right ICA and VA were successfully detected. However, a reduced VA territory was observed with the labeling plane L1 where the VA was not perpendicular to the labeling plane. Figure 3a presents the CBF maps by rVE-ASL and standard pCASL from a single subject. By visual inspection, comparable gray-matter ICA-CBF intensities were observed for all three labeling planes, whereas lowest VA-CBF intensities was observed with the labeling plane L1. Figure 3b shows the comparison of mean gray matter territorial CBF between rVE-ASL and pCASL across subjects. In line with the visual inspection, CBF values by rVE-ASL and pCASL were highly correlated with each other, regardless of labeling plane. However, it was also noticed that rVE-CBF exhibited overall smaller CBF values in the VA territory when the labeling plane was set to L1 and L2 compared to pCASL, which is consistent with the visual inspection. The in vivo results suggest that the labeling plane L3 is optimal for rVE-ASL where all feeding vessels are almost perpendicular to the labeling plane, which is in good accordance with the simulation. We further evaluated the effects of the total number of encoding steps in rVE-ASL on the territorial and CBF calculations using Dice coefficient and RMSE, respectively. Our results (Figure 4) showed that reliable vascular territories were obtained with 20 encoding steps or more and CBF measurements were relatively insensitive to the number of encoding steps.CONCLUSION
In this study, we optimized rVE-ASL through both simulation and in vivo studies. Our results have shown that the optimal labeling location is right above the bifurcation of the common carotid artery where both feeding arteries of both ICA and VA are relatively straight. When employing 20 encoding steps or more, rVE-ASL can provide reliable territorial mapping and CBF measurements. This optimized rVE-ASL technique is now poised as a reliable imaging approach for the assessment of brain vascular territories. Future work will be conducted to evaluate the clinical utility of the optimized rVE-ASL in different clinical applications.Acknowledgements
This work was partly supported by National Institute of Health (NIH) grants R01NS118019, RF1AG072490, and BrightFocus Foundation A20201411S.References
Wong EC et al. MAGMA 2012
Li Zhao et al. MRM 2017
Figures