2016
Impact of Bayesian-Inference vs Least-Squares Fitting on Multi-Delay Arterial Spin Labelling Parameter Estimation1School of Health Sciences, Faculty of Biology, Medicine and Health, The University of Manchester, Manchester, United Kingdom, 2Geoffrey Jefferson Brain Research Centre, Manchester Academic Health Science Centre, Manchester, United Kingdom, 3Quantified Imaging, London, United Kingdom, 4Philips, Farnborough, United Kingdom, 5Gold Standard Phantoms Limited, London, United Kingdom, 6Sir Peter Mansfield Imaging Centre, School of Medicine, University of Nottingham, Nottingham, United Kingdom
Synopsis
Keywords: Arterial Spin Labelling, Data Processing, Arterial Spin Labelling, Analysis, Bayesian, Kinetic Modelling
Motivation: Multi-delay Arterial Spin Labelling has application across multiple patient groups, but accurate quantification remains difficult, particularly for prolonged transit times and noisy data.
Goal(s): Compare least-squares and Bayesian-inference model fitting for perfusion estimate accuracy.
Approach: Least-squares and Bayesian-inference, specifically BASIL, pipelines were run on simulated and in-vivo ASL data with different SNR with three choices of prior/initial value for arterial transit time (ATT). The resulting cerebral blood flow (CBF) and ATT maps were compared.
Results: ATT quantification is impacted by ATT prior/initial value in Bayesian-inference fitting more than least-squares fitting. Least-squares fitting is more susceptible to CBF overestimation at lower SNR.
Impact: MD-ASL analysis method can impact ATT accuracy. Bayesian-inference fitting is better for lower SNR data when CBF is the primary interest. Least-squares fitting is better for higher SNR data, when prior/estimate is not well known, and for accurate ATT estimation.
Introduction
Multi-delay arterial spin labelling (MD-ASL), in comparison to single delay data, allows for more accurate cerebral blood flow (CBF) quantification and the estimation of arterial transit time (ATT)1,2 which is shown to be prolonged in multiple diseases3,4. ASL-MRI however suffers from low signal-to-noise-ratio (SNR) making quantification of ATT difficult5. Recently the Open Science Initiative for Perfusion Imaging (OSIPI) group published an ASL processing pipeline inventory, highlighting BASIL as a robust pipeline for quantification6. BASIL uses Bayesian-inference with priors to aid in quantifying CBF and ATT7,8, including options to modify the ATT prior. The impact of ATT priors on parameter estimates has not been reported.This study compares quantification of perfusion parameters between BASIL and least-squares fitting for both simulated and in-vivo MD-ASL data at a range of SNR using different ATT priors.
Methods
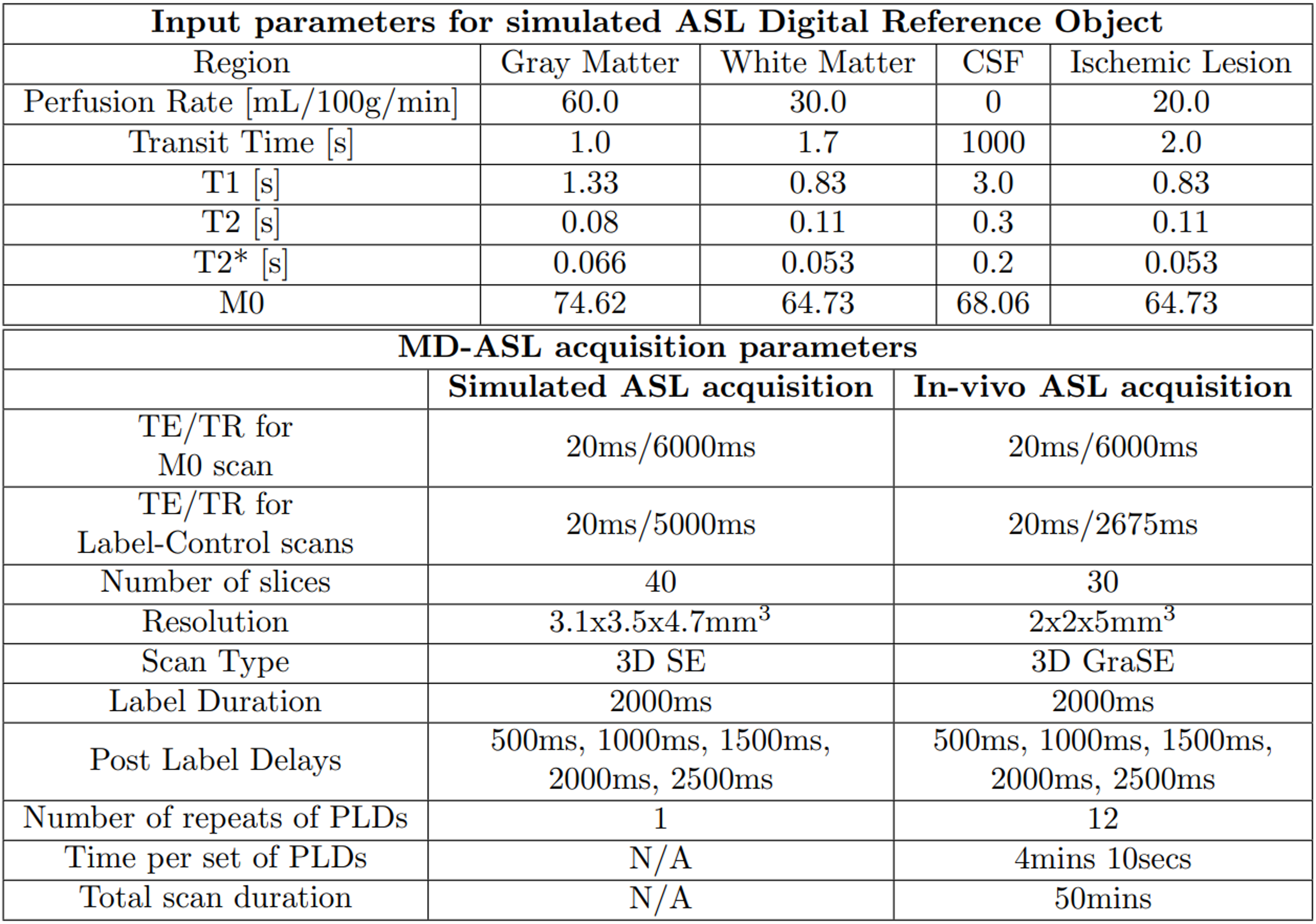
MD-ASL data was simulated using the ASL Digital Reference Object software available through OSIPI9,10, including both a dataset with no noise and the ASLDRO default noise of 100, which is considered to be a similar SNR to typical in-vivo data11. Typical grey matter/white matter input values were simulated and a region of prolonged ATT and low CBF was added, mimicking an ischemic region as might be seen in stroke (Figure 1).In-vivo ASL data was acquired on one healthy 26-year-old male with the scan acquisition parameters described in Figure 1. 12 repeats of the MD-ASL data were sub-sampled and averaged to vary the SNR of each dataset: 12 datasets of 1 repeat (lowest SNR), 6 datasets of 2 repeats, 4 datasets of 3 repeats, etc.
Data was analysed using BASIL and least-squares fitting (in Python) with ATT priors/initial values of 1.3, 1.7, and 2secs12,13 to determine how SNR of data and prior/initial ATT value impacted the quantification of CBF and ATT. Least-squares and BASIL analysis used the ‘single blood compartment’ model14 with T1blood=1.65secs, grey matter M0 calibration for simulated data, and CSF M0 calibration in-vivo. BASIL used no macrovascular compartment, spatial priors on, and structural image provided. For the simulated ASL data, BASIL was run with varying weight given to the prior, determined by the standard deviation of the prior. The default standard deviation of 1sec (denoted SD=1sec) was compared to SD=10secs.
Results and Discussion
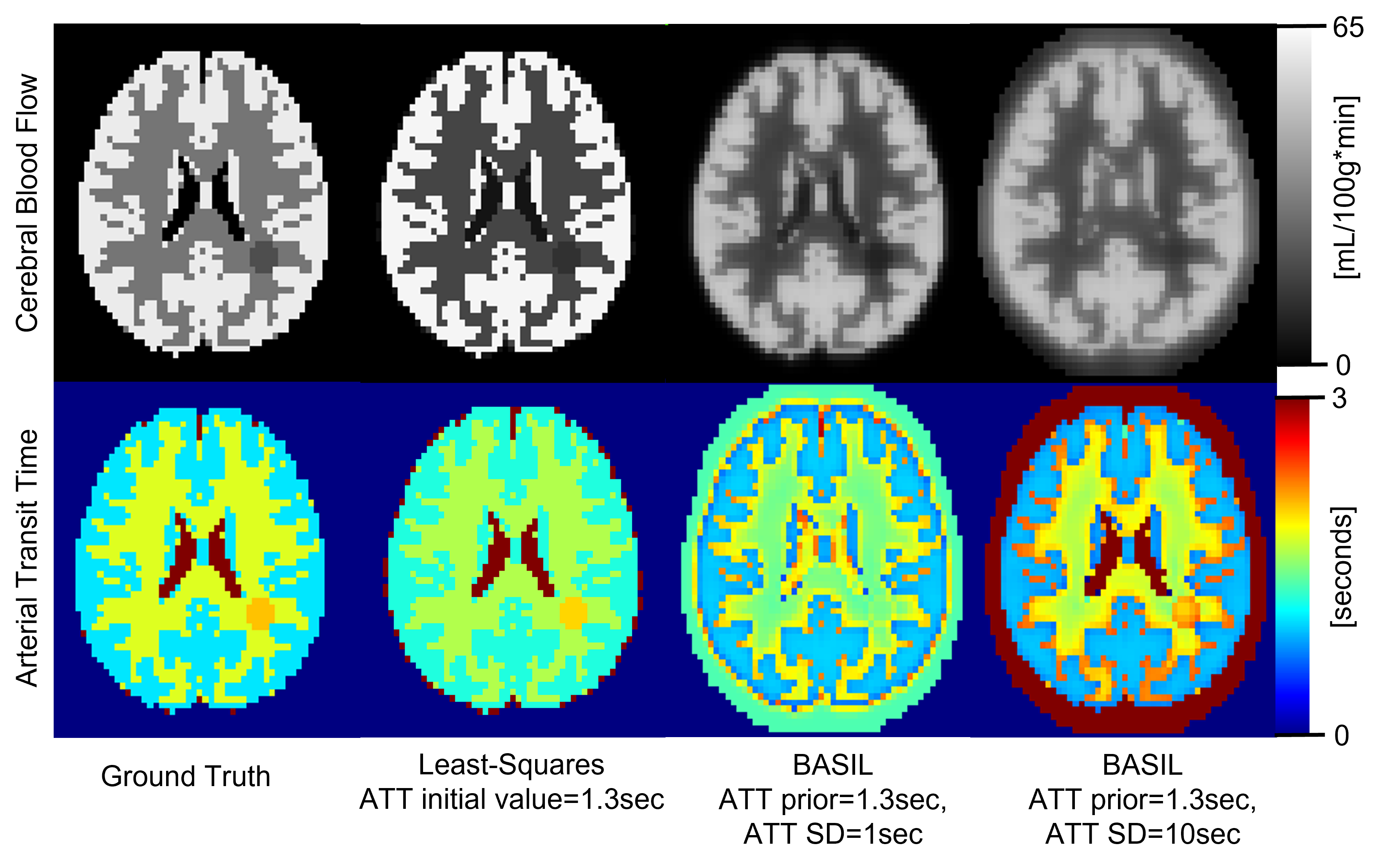
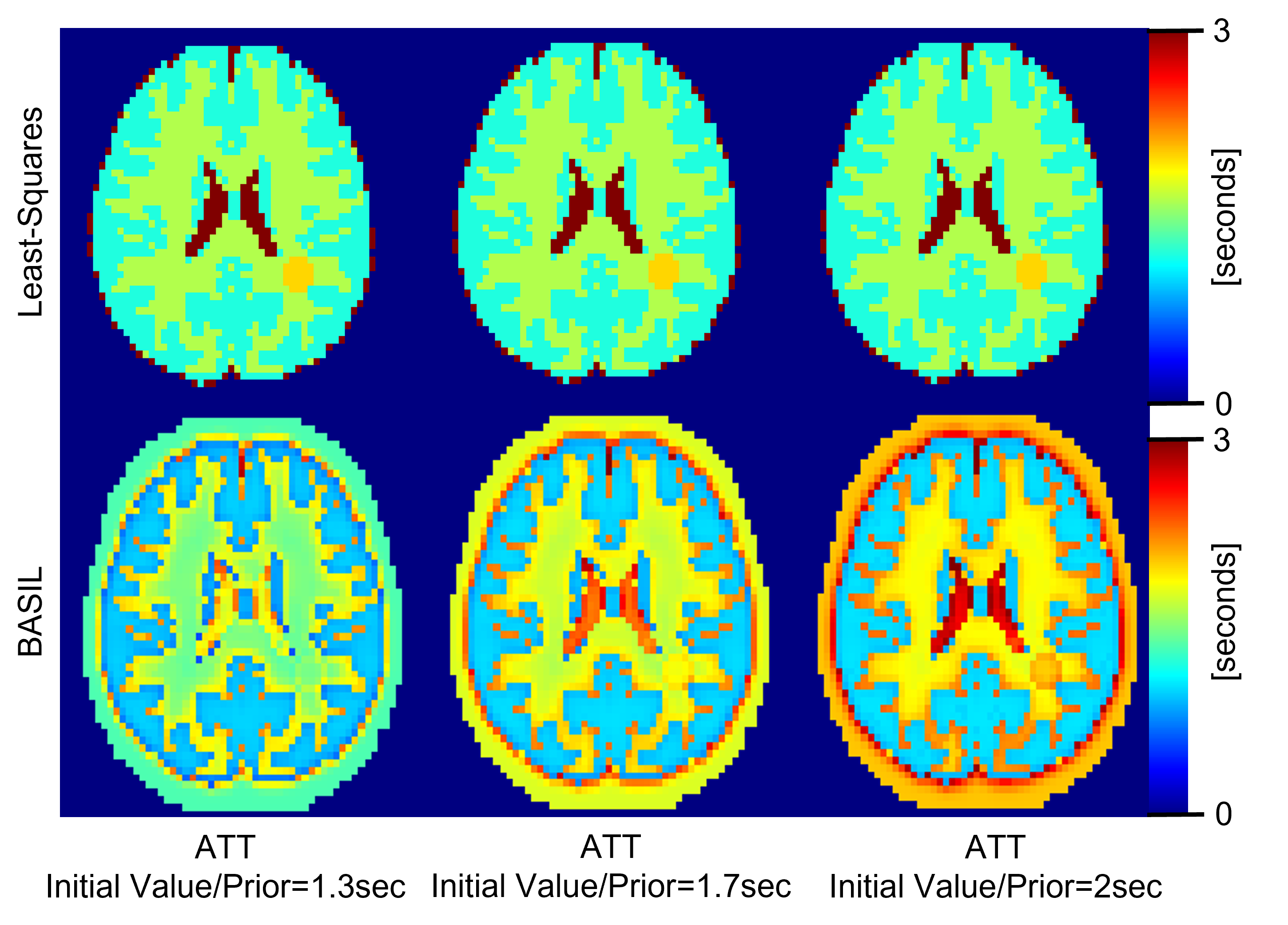
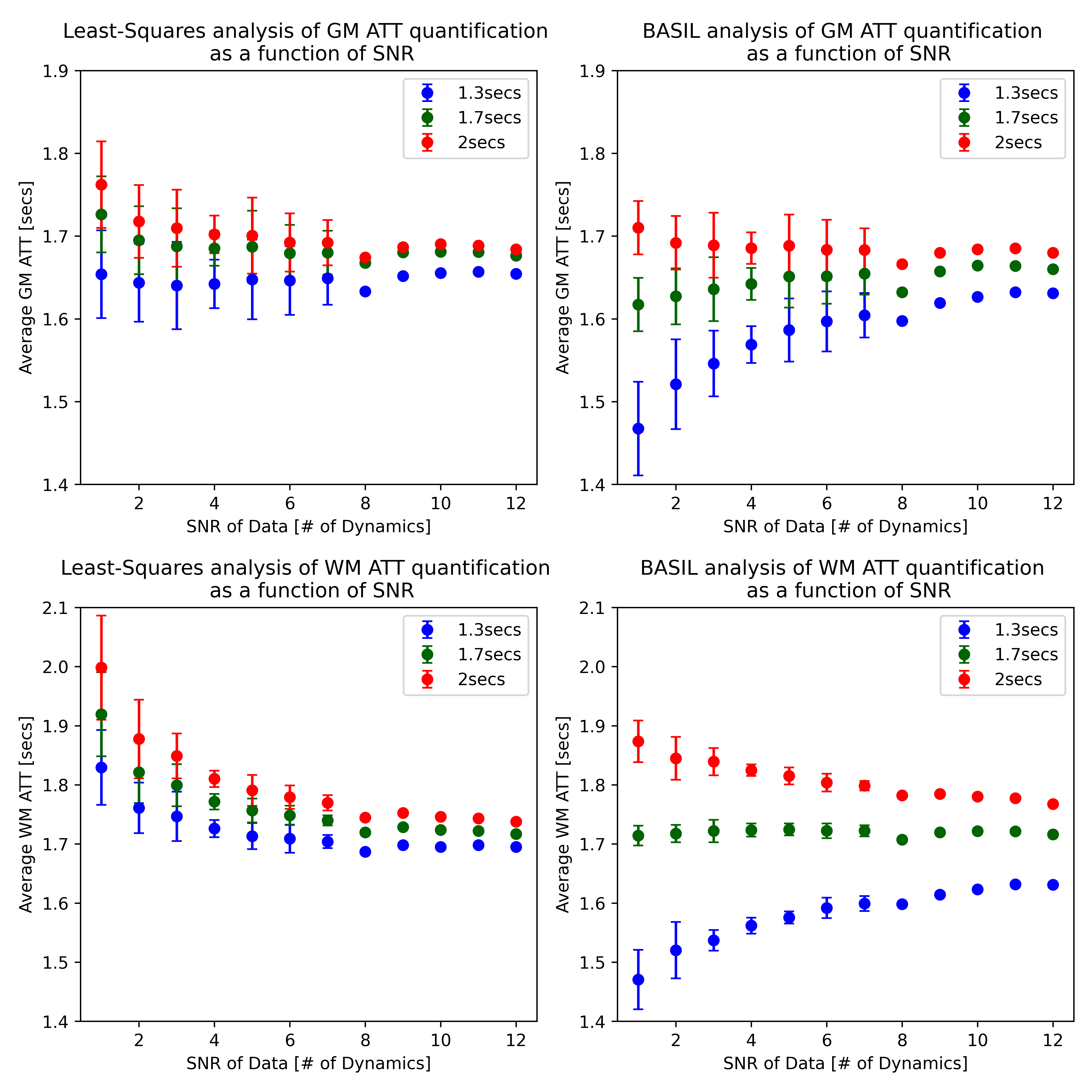
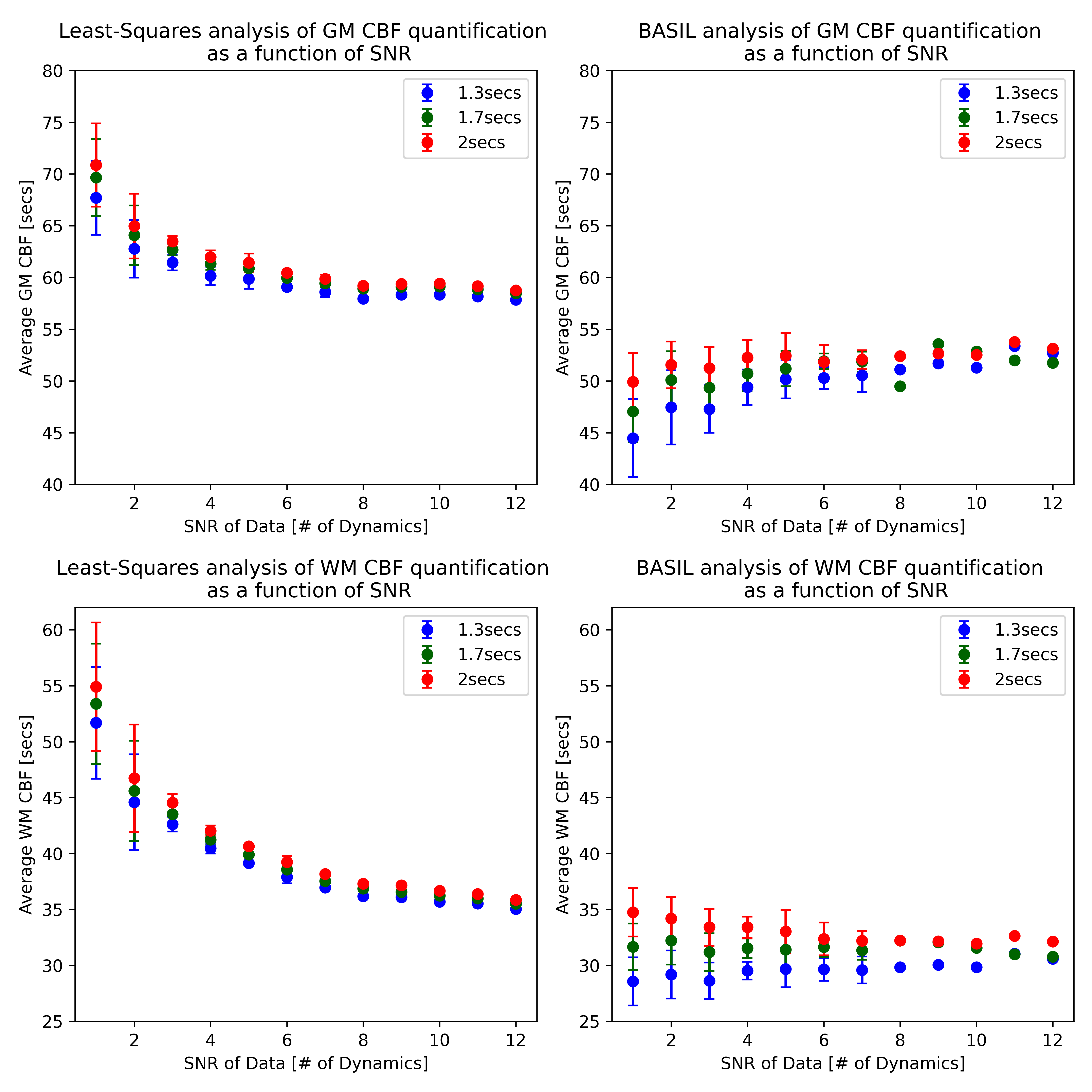
The CBF and ATT maps from the noise-free simulated data (Figure 2) show that the lesion with prolonged ATT is not easily visible using default BASIL processing (ATT prior=1.3secs and SD=1sec), but becomes more apparent for the BASIL run with an ATT SD of 10secs. The lesion is also more distinguishable if the ATT prior is modified to 1.7secs or 2secs (Figure 3). The lesion was more visible for least-squares fitting than BASIL regardless of ATT prior/initial value, but ATT was systematically underestimated. The least-squares and BASIL pipelines showed similar results in the noisy simulated MD-ASL data.In-vivo MD-ASL results show that quantification of transit time is more dependent on the ATT prior/initial value for lower SNR data particularly for analysis done with BASIL (Figure 4). The average ATT quantified using least-squares was less dependent on the ATT initial value, however, ATT appears to be overestimated at lower SNR. Figure 5 shows that the CBF quantified using least-squares fitting is overestimated at lower SNR, particularly in white matter, but this overestimation and the CBF quantification is less impacted by the ATT initial value compared to CBF quantified using BASIL. BASIL showed more consistent CBF estimates across SNR levels compared to least-squares, suggesting BASIL performs better at quantifying accurate CBF at lower SNR.
Conclusion
Several studies have used BASIL to analyse MD-ASL including stroke studies with regions of low perfusion and/or long ATT similar to those simulated in this study15–17. However, the simulation results of this study show that, even with noise-free data, absolute quantification of ATT and the ability to distinguish a region of prolonged ATT is dependent on the prior given (seen in Figure 3).Overall, this study indicates that care should be taken when deciding the processing for MD-ASL data (including an accurate ATT prior or modifying the SD of the prior), particularly for lower SNR data, or patient groups with prolonged ATT. Additionally, when comparing the CBF and ATT results of different studies both the similarity of processing pipelines and the data acquisition (specifically data SNR) need to be considered.
These findings are important for clinical applications of ASL where model choices may influence visibility of abnormally perfused tissue (particularly prolonged ATT) or where clinical variation in ATT is a similar to size12 to the variation seen from quantification done using different ATT priors.
Acknowledgements
The authors acknowledge support from Philips healthcare for funding the studentship of AF.References
1. Golay X, Ho ML. Multidelay ASL of the pediatric brain. Br J Radiol. 2022;95(1134):20220034. doi:10.1259/bjr.20220034
2. Woods JG, Achten E, Asllani I, et al. Recommendations for Quantitative Cerebral Perfusion MRI using Multi-Timepoint Arterial Spin Labeling: Acquisition, Quantification, and Clinical Applications. Published online September 6, 2023. doi:10.31219/osf.io/4tskr
3. Amemiya S, Watanabe Y, Takei N, et al. Arterial Transit Time-Based Multidelay Combination Strategy Improves Arterial Spin Labeling Cerebral Blood Flow Measurement Accuracy in Severe Steno-Occlusive Diseases. J Magn Reson Imaging. 2022;55(1):178-187. doi:10.1002/jmri.27823
4. Fan AP, Guo J, Khalighi MM, et al. Long-Delay Arterial Spin Labeling Provides More Accurate Cerebral Blood Flow Measurements in Moyamoya Patients. Stroke. 2017;48(9):2441-2449. doi:10.1161/STROKEAHA.117.017773
5. Petcharunpaisan S, Ramalho J, Castillo M. Arterial spin labeling in neuroimaging. World J Radiol. 2010;2(10):384-398. doi:10.4329/wjr.v2.i10.384
6. Fan H, Mutsaerts HJMM, Anazodo U, et al. ISMRM Open Science Initiative for Perfusion Imaging (OSIPI): ASL pipeline inventory. Magn Reson Med. n/a(n/a). doi:10.1002/mrm.29869
7. Chappell MA, Groves AR, Whitcher B, Woolrich MW. Variational Bayesian inference for a nonlinear forward model. IEEE Trans Signal Process. 2009;57(1):223-236. doi:10.1109/TSP.2008.2005752 8. Groves AR, Chappell MA, Woolrich MW. Combined spatial and non-spatial prior for inference on MRI time-series. NeuroImage. 2009;45(3):795-809. doi:10.1016/j.neuroimage.2008.12.027
9. Oliver-Taylor A, Hampshire T, Smith NAS, et al. “ASLDRO: Digital reference object software for Arterial Spin Labelling.” Proceedings of ISMRM, London, 2021
10. GitHub - gold-standard-phantoms/asldro: Digital Reference Object for Arterial Spin Labelling. Development Version (sha1: 97608be). https://github.com/gold-standard-phantoms/asldro/tree/master
11. Series Type: ASL — ASL DRO documentation. Accessed October 29, 2023. https://asldro.readthedocs.io/en/stable/usage/series-asl.html?highlight=noise#single-value-parameters
12. Al-Bachari S, Vidyasagar R, Emsley HC, Parkes LM. Structural and physiological neurovascular changes in idiopathic Parkinson's disease and its clinical phenotypes. J Cereb Blood Flow Metab. 2017 Oct;37(10):3409-3421. doi: 10.1177/0271678X16688919.
13. McFadden J, Matthews J, Scott L, Herholz K, Lohezic M, Parkes LM, ‘Oxygen Extraction Fraction is higher in elderly participants with a higher cardiovascular disease risk; a combined QSM and ASL study’, Proceedings of ISMRM, Toronto, 2022
14. Alsop DC, Detre JA, Golay X, et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med. 2015;73(1):102-116. doi:10.1002/mrm.25197
15. Luijten SPR, Bos D, van Doormaal PJ, et al. Cerebral blood flow quantification with multi-delay arterial spin labeling in ischemic stroke and the association with early neurological outcome. NeuroImage Clin. 2023;37:103340. doi:10.1016/j.nicl.2023.103340
16. Harston GWJ, Okell TW, Sheerin F, et al. Quantification of Serial Cerebral Blood Flow in Acute Stroke Using Arterial Spin Labeling. Stroke. 2017;48(1):123-130. doi:10.1161/STROKEAHA.116.014707
17. Okell TW, Harston GWJ, Chappell MA, Sheerin F, Kennedy J, Jezzard P. Measurement of collateral perfusion in acute stroke: a vessel-encoded arterial spin labeling study. Sci Rep. 2019;9:8181. doi:10.1038/s41598-019-44417-7
Figures