2015
Improving pCASL CBF mapping in neonates and adults with enhanced background suppression and complex subtraction1Department of Biomedical Engineering, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 2Department of Radiology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 3Department of Pediatrics, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 4Department of Diagnostic Radiology and Nuclear Medicine, University of Maryland School of Medicine, Baltimore, MD, United States, 5F.M. Kirby Research Center for Functional Brain Imaging, Kennedy Krieger Research Institute, Baltimore, MD, United States
Synopsis
Keywords: Arterial Spin Labelling, Perfusion
Motivation: Standard arterial spin labeling (ASL) uses modest background-suppression to enhance SNR, which may not be optimal in reducing noise.
Goal(s): Our goal was to further improve the SNR in ASL and reliably measure the cerebral blood flow (CBF) in low-perfusion scenarios such as neonates.
Approach: We utilized an enhanced background suppression to minimize the signal from static background tissue. Complex subtraction of control/labeled signals was done to correct the magnetization sign-switching in between.
Results: Enhanced background suppression combined with complex subtraction improved the reliability of CBF measurement in both neonates and adults, particularly benefiting the quality of neonatal CBF mapping.
Impact: The improvement of SNR in ASL through enhanced background suppression coupling complex subtraction can facilitate the quality of cerebral blood flow measurement. The benefits are more pronounced in low-perfusion scenarios, such as bolstering the reliability of neonatal ASL.
INTRODUCTION
Arterial spin labeling (ASL) is a useful and well validated non-invasive, quantitative technique for measuring CBF in adults in research and clinical applications.1-4 However, the implementation of ASL in neonates is still challenging,5,6 primarily attributed to small brain sizes and low perfusion.5 The signal of neonatal ASL is bound by physical limits, e.g., the amount of perfusion spins available. Therefore, we aim to reduce the noise in ASL. Standard ASL uses modest background suppression to ensure that the signs of the magnetizations remain positive and the control signal intensity is always greater than the label intensity.7 Here we used complex subtraction of control/labeled signals to remove this constraint, which allowed us to utilize an enhanced background suppression scheme. The SNR benefits of this scheme were tested in both adults and healthy neonates.METHODS
Background suppression schemes: Enhanced background suppression (denoted as enhanced BS) was developed and compared to regular background suppression (regular BS) using a 3D GRASE pseudo-continuous arterial-spin-labeling (pCASL) sequence. Figure 1a illustrates the T1-relaxation simulation for the enhanced BS, which employs two inversion pulses (2136ms, 3430ms after pre-saturation) to achieve minimal signal from static background tissue (gray/white matter) (Figure 1b). In contrast, the regular BS retains ~4% of tissue signal.Study 1: Evaluation of enhanced BS in adults: We first tested this method in adults. The two BS schemes described above were performed in 4 healthy adults (24.0±0.8 years) on a 3T Siemens Prisma system. Labeling duration=1800ms, PLD=2000ms, 4 segments, number-of-pairs=24.
CBF quantification: CBF values were computed using the standard single-compartment model1:
$$CBF=\frac{6000\cdot \lambda \cdot \triangle M\cdot e^{\frac{PLD}{T_{1,blood} } } }{2\cdot \alpha \cdot T_{1,blood}\cdot M_{0}\cdot (1-e^{-\frac{\tau }{T_{1,blood} } }) } $$
Both magnitude subtraction and complex subtraction were assessed as means to obtain ∆M from the enhanced background-suppressed pCASL images. For complex subtraction, we conducted vector subtraction in the complex plane between control and labeled signals, followed by taking its magnitude.
Study 2: Enhanced background suppression in neonates: The enhanced BS and regular BS schemes were performed in 4 healthy, non-sedated neonates (3 males, gestational age 39.1±0.1 weeks). A previously described AFS-pCASL sequence8 was employed to minimize macrovascular contaminations in neonatal ASL CBF images with labeling duration=1800ms, PLD=2175ms, FOV=140×140×72mm³, voxel-size=3.5×3.5×4mm³, TR/TE=5000/24.76ms, number-of-pairs=20, scan time=3'30''. Each BS scheme was performed twice to allow test-retest assessment.
RESULTS AND DISCUSSION
Figure 1c displays representative pCASL control images obtained from regular BS and enhanced BS schemes. The profiles of absolute signal intensity of a highlighted row are shown in Figure 1d. As demonstrated, the enhanced scheme resulted in substantially lower tissue signals.Figures 2a,b,c show the CBF maps acquired with the two BS schemes. A substantial amount of negative CBF values were observed in the enhanced BS CBF map when the traditional processing of magnitude subtraction was used (Figure 2b). These errors primarily occurred in voxels where there was a sign switching in magnetization between the control/labeled signals. We illustrated this in Figure 2d using three representative voxels. However, upon using complex subtraction, the erroneous values in Figure 2b have been corrected (Figure 2c).
To test whether the enhanced BS scheme can improve the reliability of the CBF map, we split the twenty-four CBF measurements into bins and averaged data in each bin (with standard deviation [STD] evaluation across bins). Different bin sizes were tested. Figure 3a displays a group-averaged map of STD, while quantitative STD values are shown in Figure 3b. Enhanced BS showed a lower STD than the regular BS, especially when bin size is small (i.e., noise level is high).
The benefits of enhanced BS are more important in low-perfusion scenarios such as neonates. Figure 4a displays CBF maps of a representative neonate acquired using enhanced BS and regular BS. Each sequence was performed twice. The enhanced BS improved the quality of the CBF maps in both runs.
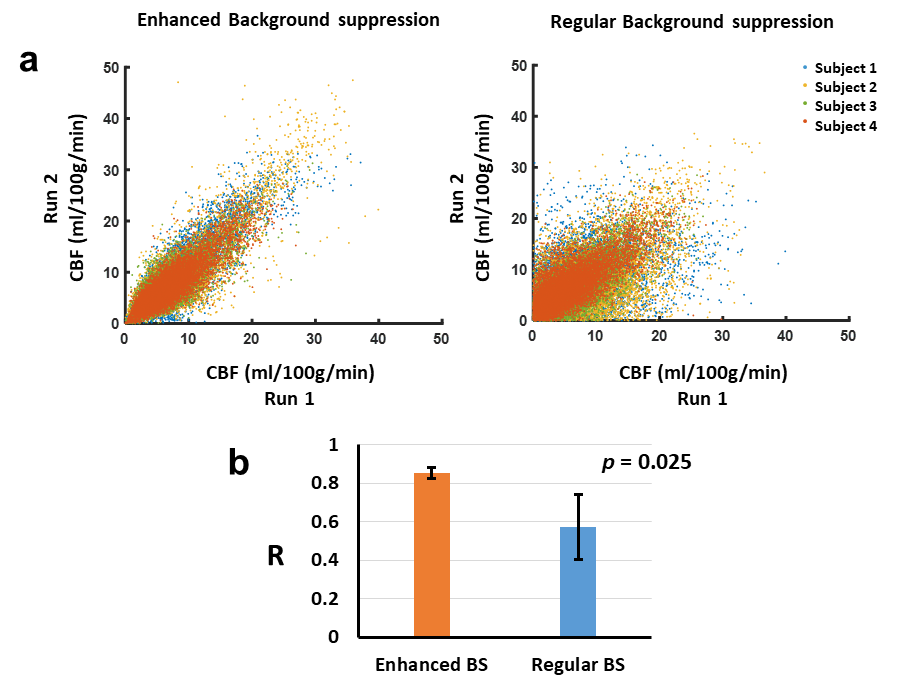
To quantitatively evaluate the reproducibility, the scatter plot of CBF values between two runs in all 4 subjects were shown (Figure 5a). It can be seen that the results from enhanced BS were better clustered compared to the regular BS. The spatial correlation of enhanced BS (R=0.85±0.03) was significantly higher than regular BS (R=0.57±0.17) (P=0.025, Figure 5b).
We recognize that reproducibility of complex numbers should also include phase angle consistencies. Figure 4b displays voxels that exhibited inconsistent phase angles of complex difference vectors between two runs (i.e. angles>90°), constituting 1.8% of the entire brain volume. These mainly occurred in white matter regions.
CONCLUSION
We demonstrated that pCASL with enhanced background suppression, when combined with complex subtraction, can improve the quality of CBF measurement, thus bolstering the reliability of neonatal pCASL.Acknowledgements
No acknowledgement found.References
1. Alsop DC, Detre JA, Golay X et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med 2015;73:102-116.
2. De Vis JB, Peng SL, Chen X, Li Y, Liu P, Sur S, Rodrigue KM, Park DC, Lu H. Arterial-spin-labeling (ASL) perfusion MRI predicts cognitive function in elderly individuals: A 4-year longitudinal study. J Magn Reson Imaging 2018;48:449-458.
3. Benedictus MR, Binnewijzend MAA, Kuijer JPA, Steenwijk MD, Versteeg A, Vrenken H, Scheltens P, Barkhof F, van der Flier WM, Prins ND. Brain volume and white matter hyperintensities as determinants of cerebral blood flow in Alzheimer's disease. Neurobiol Aging 2014;35:2665-2670.
4. Proisy M, Corouge I, Legouhy A, Nicolas A, Charon V, Mazille N, Leroux S, Bruneau B, Barillot C, Ferre JC. Changes in brain perfusion in successive arterial spin labeling MRI scans in neonates with hypoxic-ischemic encephalopathy. Neuroimage Clin 2019;24:101939.
5. Baranger J, Villemain O, Wagner M, Vargas-Gutierrez M, Seed M, Baud O, Ertl-Wagner B, Aguet J. Brain perfusion imaging in neonates. Neuroimage Clin 2021;31:102756.
6. Delmas J, Toupin S, Pfeuffer J, Chateil JF. A practical guide to optimize arterial spin labeling in neonates at 1.5 Tesla: what the radiologist needs to know. Pediatr Radiol 2022;52:1370-1380.
7. Maleki N, Dai W, Alsop DC. Optimization of background suppression for arterial spin labeling perfusion imaging. MAGMA 2012;25:127-133.
8. Hu Z, Jiang D, Shepard J, Uchida Y, Oishi K, Liu P, Lin D, Yedavalli V, Tekes A, Golden WC, Lu H. Macrovasculature-suppressed ASL MRI in neonates: quantification of cerebral blood flow and arterial transit time. In: Proceedings of the ISMRM & SMRT Annual Meeting & Exhibition 32th Annual Meeting. 2023.
Figures
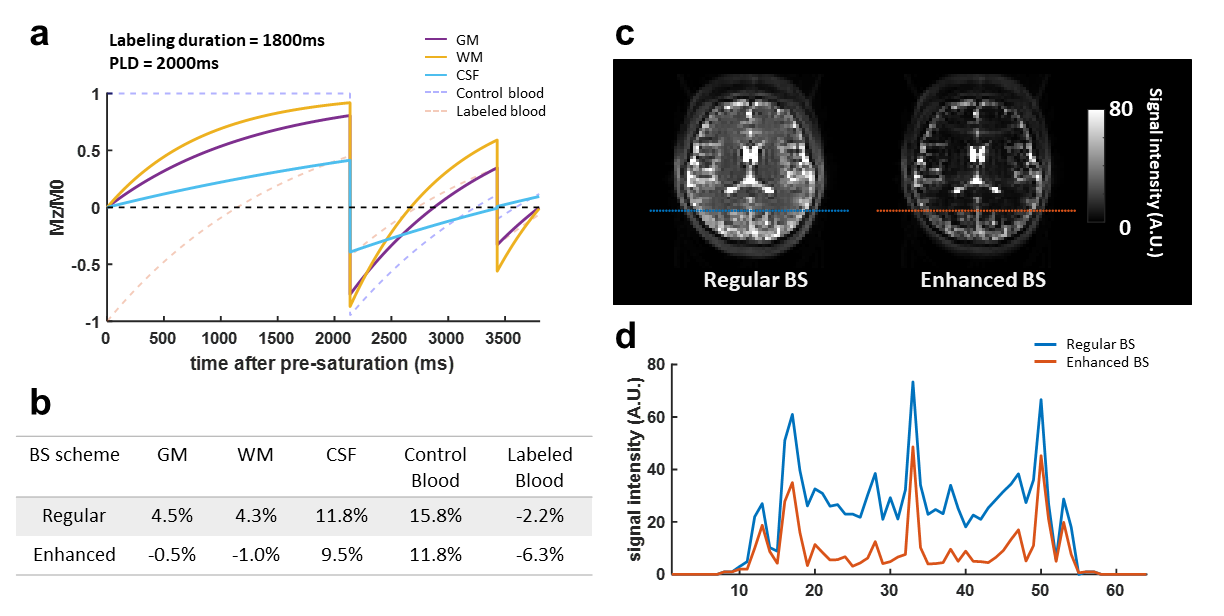
Figure 1. Illustration and representative data of pCASL with enhanced and regular background suppression. (a) T1 relaxation simulation of enhanced BS. ASL parameters: labeling duration=1800ms, PLD=2000ms, inversion time 1 = 2136ms, inversion time 2 = 3430ms. (b) Summary of residual signal percentages for regular BS and enhanced BS. (c) pCASL control images of a representative. (d) The profiles of absolute signals in pCASL control images of the highlighted row in (c).
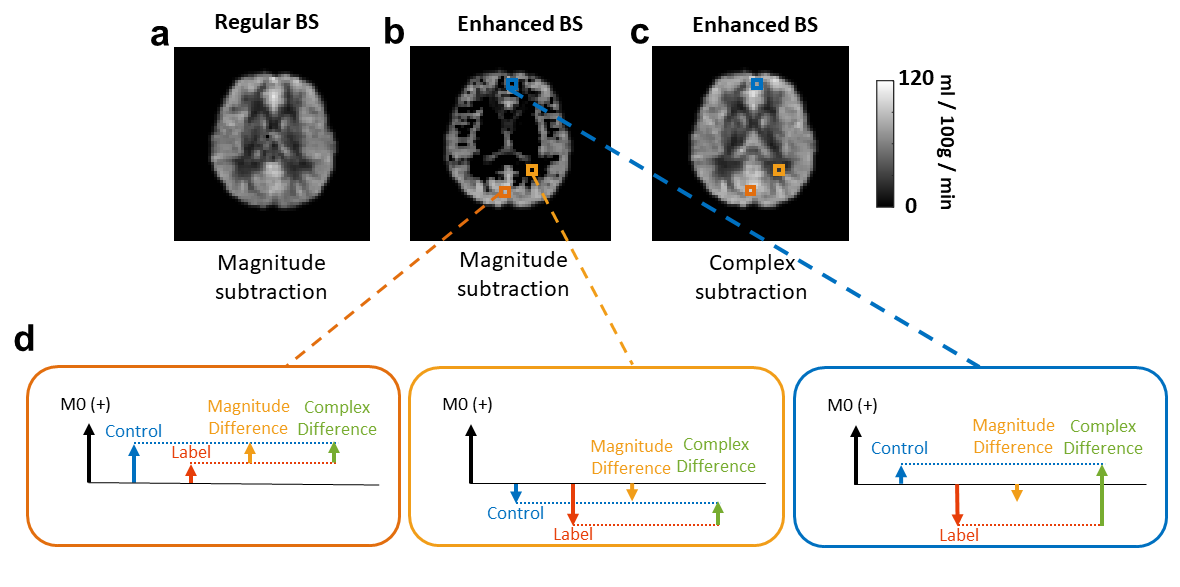
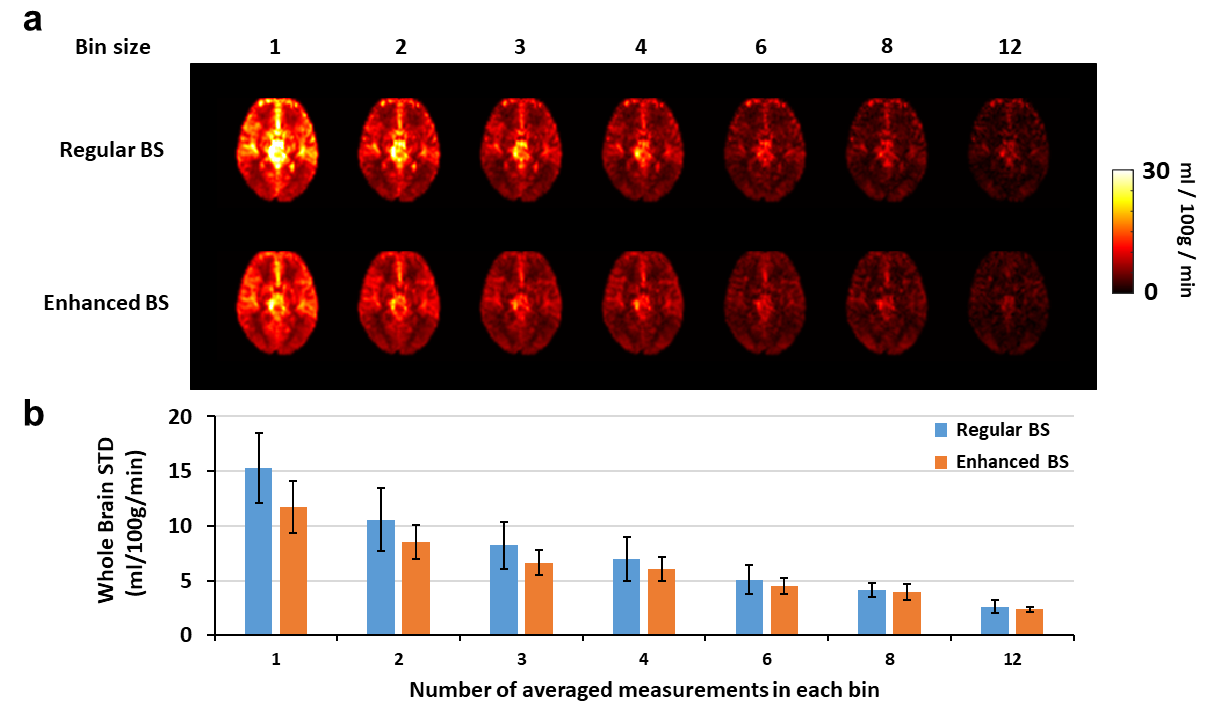
Figure 3. Comparison among standard deviations across bins between regular BS and enhanced BS. (a) Group-averaged standard deviation maps with different bin sizes. STDs across bins were computed after CBF measurements were averaged within bins. (b) Bar plot of whole brain averaged standard deviation.
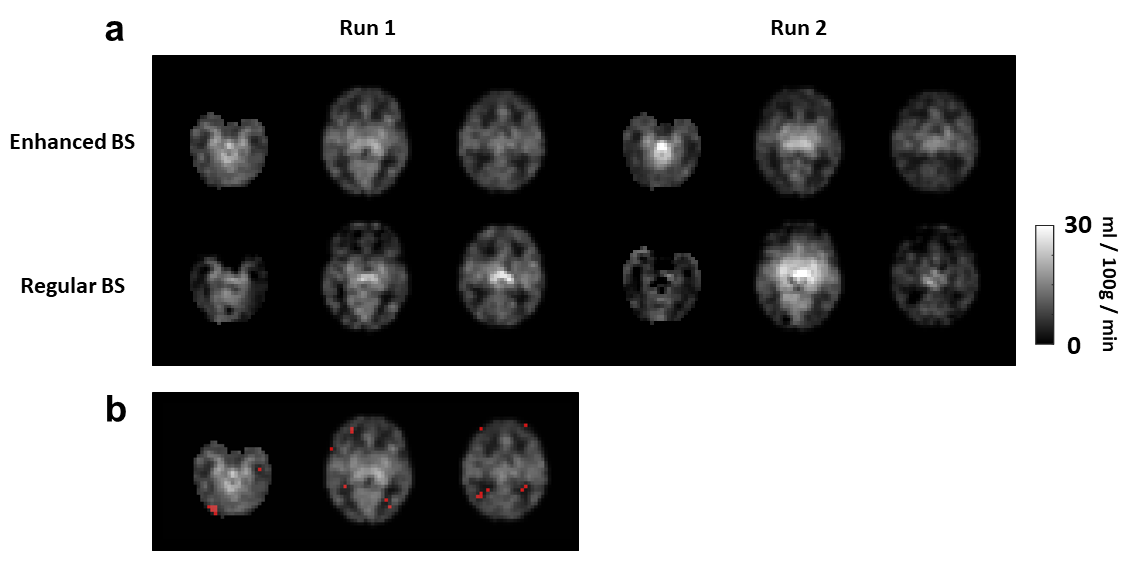
Figure 4. Test-retest of background suppression schemes in CBF measurements of a representative neonate. (a) CBF maps acquired from enhanced BS and regular BS in two separate runs. (b) Voxels that exhibited inconsistent orientations of complex difference vectors between two runs (i.e. angles > 90°).