2012
Velocity Selective Arterial Spin Labeling at 7T1Radiology, C.J. Gorter MRI Center, Leiden Univeristy Medical Center, Leiden, Netherlands, 2Radiology, Center for Image Sciences, Univeristy Medical Center Utrecht, Utrecht, Netherlands
Synopsis
Keywords: Arterial Spin Labelling, Arterial spin labelling
Motivation: Velocity selective (VS)-ASL can be of great added benefit for fMRI at ultra-high field because of its specificity and ATT-insensitivity.
Goal(s): Our goal was to show the feasibility of VS-ASL at 7T with minimal TR, which involves minimizing SAR and timing parameters within the sequence.
Approach: VS-ASL was implemented using BIR4 labeling module and compared to the robust FAIR ASL. Image quality was measured based on quantified ASL-signal and tSNR-efficiency.
Results: Good agreement between FAIR and VSSinv-ASL was found. VSSinv-ASL was used to create intrinsic BGS without additional SAR. A shortest TR of 4500ms was achieved which could potentially be shorted with pTx.
Impact: We showed the feasibility of Velocity Selective (VS)-ASL at UHF and the application in fMRI. VS-ASL showed comparable but less homogeneous tSNR as FAIR. VS-ASL is of added benefit for fMRI at ultra-high field because of its specificity and ATT-insensitivity.
Background:
Despite the longer T1 and therefore less severe decay of label, arterial spin labeling (ASL) at ultra-high field (UHF: 7T and above) has been found challenging mainly due to magnetic field inhomogeneities, B1-inhomogeneities, increase in physiological noise, shorter T2, and high specific absorption rate (SAR)(1). Over the last years, pseudo continuous (pC)ASL(2) and pulsed (P)ASL using FAIR(3) have shown to provide robust perfusion maps at 7T. Velocity selective (VS)-ASL creates label within the imaging volume by saturating the blood flowing above a certain cut-off velocity (Vcut) and is therefore insensitive to arterial-transit-time (ATT) delays which enables scanning with short PLDs(4). Moreover, the fact that label is also created within the sweet spot of the transmit coil, could be the essential advantage of VS-ASL over other ASL-approaches. In this abstract, we show the first feasibility of 3D VS-ASL at 7T and compared it to current state-of-the-art FAIR and show its use in fMRI.Methods:
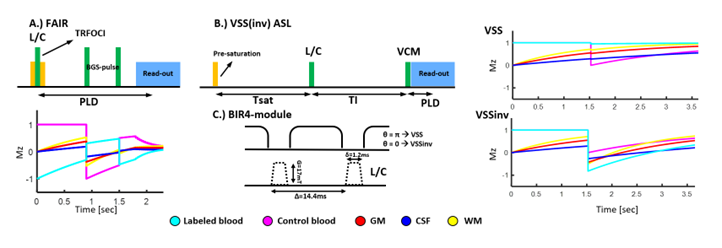
Velocity selective saturation (VSS)-ASL was implemented using a BIR4 labeling module (Figure 1) that consists of adiabatic excitation and refocusing to guarantee proper performance in the presence of severe B1- and B0-inhomogeneties. Meta-materials were placed around the head to homogenize B1(5). Because of the short T2 of blood (54ms) at 7T, single refocusing (BIR4) with its short TE was chosen over a double-refocused hyperbolic-secant (DRHS). Further design criteria were minimal SAR and thereby TR, especially to support neuroscience applications of VS-ASL.In this abstract, we first compared VSS-ASL to the current state-of-the-art implementation of FAIR. Secondly, we investigated the effect of background suppression (BGS) on the VSS-ASL signal by comparing VSS-ASL to VSSinv-ASL(6). In the latter, a π/2 phase-offset is added to the last BIR4 segment resulting in an inversion of the static tissue providing intrinsic BGS without additional SAR. The influence of CSF diffusion weighting was studied by short TI experiments. Lastly, we studied whether the recommendations from the VS-ASL grey-paper(4) are also applicable at 7T by varying Tsat (750:250:1500ms) and Vcut (1,2 and 4cm/s), because we hypothesized that these are most dependent on B1-coverage (Figure 1).
Volunteers were scanned on a Philips 7T Achieva (Best, Netherlands) equipped with a 32R-2Tx Nova head coil. The read-out (3D Gradient-echo EPI, FOV=210x210x51mm, voxel-size=3x3x3mm (reconstructed at 1.8mm inplane), SENSERL=3, FA=20°, TR/TE=26/8.3ms, SPIR fat-suppression) was kept the same for VSS-ASL and FAIR. FAIR scanning parameters: PLD=1800ms, QUIPPSII=1000ms, 2 BGS-pulses at 900ms and 1500ms, TR=7000ms (Figure 1A). Base parameters of VSS(inv)-ASL: TI=1500ms, Vcut=2cm/s, Tsat=1500ms and vascular-crushing-module (VCM) (Figure 1B,C). For all scans, 20 averages were acquired at ≈85% of the SAR-limit.
Results & Discussion
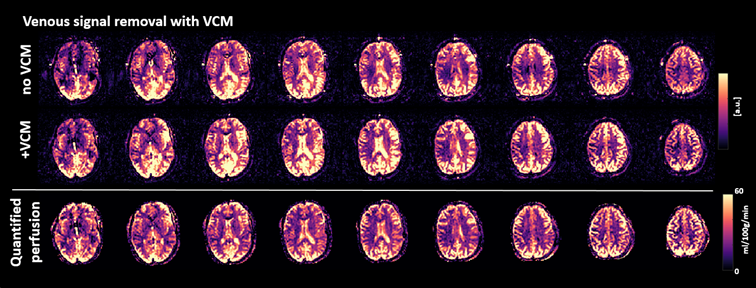
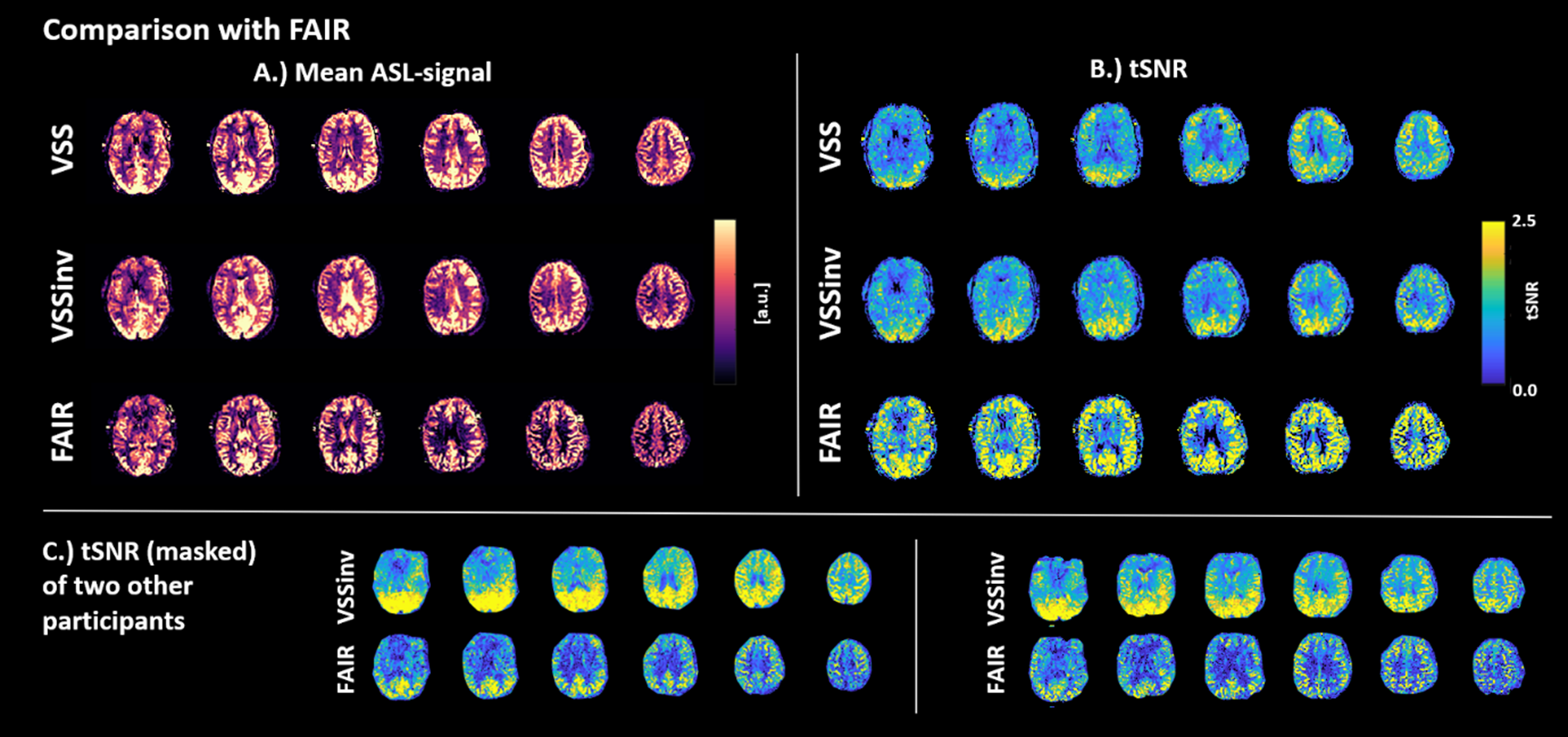
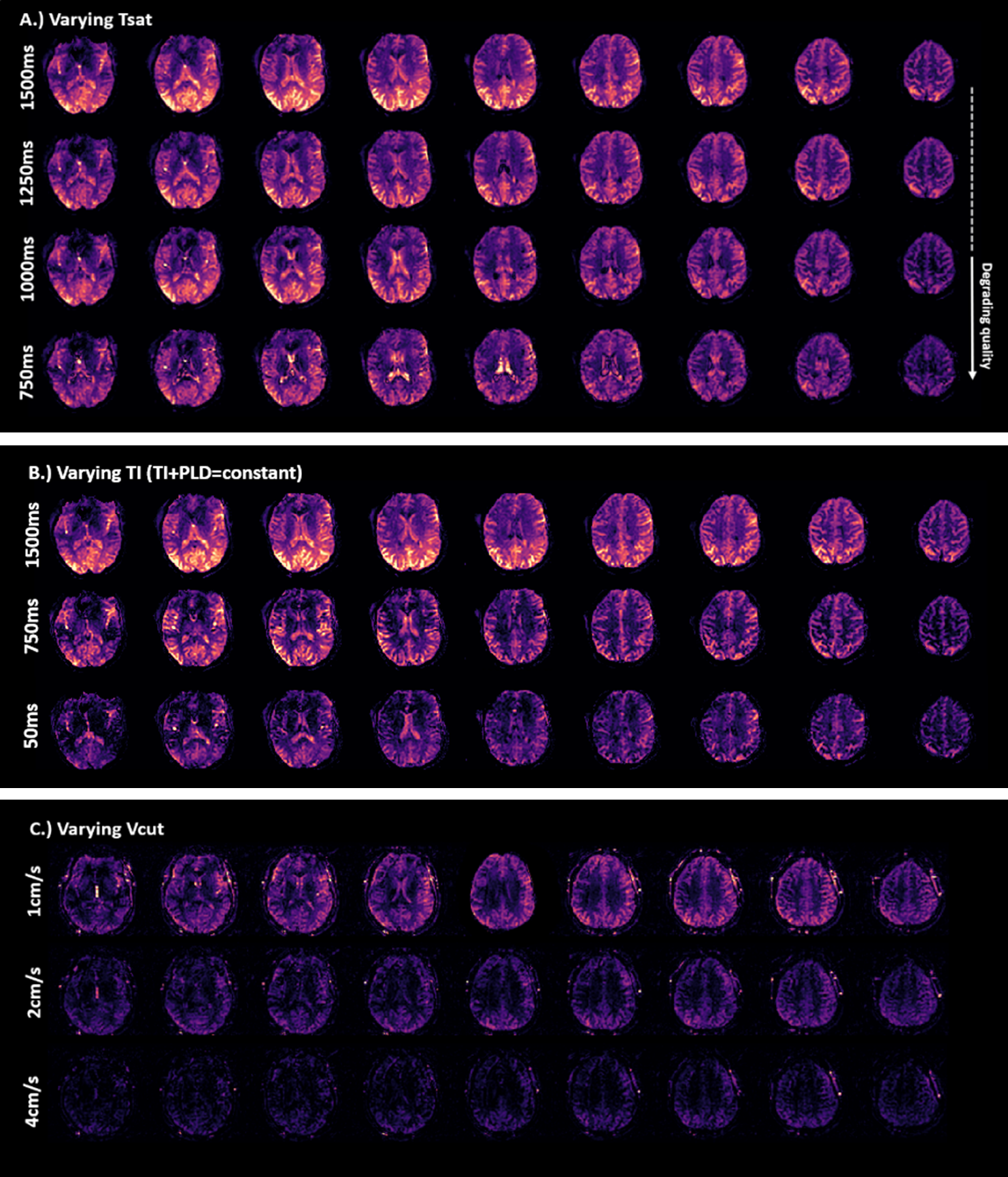
Figure 2 shows ASL-maps without and with VCM, as well as quantitative perfusion maps of VSSinv-ASL. Mean GM perfusion of this participant was 41.1ml/100g/min which is in line with average literature values. Comparable mean GM perfusion values were found (42.7ml/100g/min) between VSSinv and FAIR (Figure 3). Mean GM tSNR was similar for FAIR (1.73±0.5) and VSASL (1.77±0.3). However, for VSS-ASL it should be noted that the tSNR is especially good in the posterior part of the brain and that the FAIR tSNR is more homogeneous within the cortex and would therefore be preferable. The high tSNR in the posterior lobe could be explained by the meta-materials placement. The use of pTx would be a good solution to improve B1-homogeneity.Because of the selective pre-saturation and limited extent of the transmit coil, the Tsat could potentially be shorter than 1500ms since a clear decrease in ASL-signal was only found for Tsat=750ms (Figure 4A), however already a small penalty in ASL-signal was found at Tsat=1250ms. Besides the decreased ASL-signal, it can also be observed that the ventricles become more visible, which could be partly explained by difference in BGS.
To investigate diffusion-weighting, the TI and PLD were shortened, since it is expected that diffusion-weighting will remain the same (as can be seen in Figure 4B in the ventricles), but perfusion signal will decrease. This proves that while it is possible to measure perfusion at 7T, CSF diffusion-weighting is also present, although smaller than the signal due to perfusion. Additionally, in Figure 4C variations in ASL-signal can be seen as a function of Vcut, where also at 7T, with the small transmit coverage, a Vcut around 1-2cm/s seems optimal.
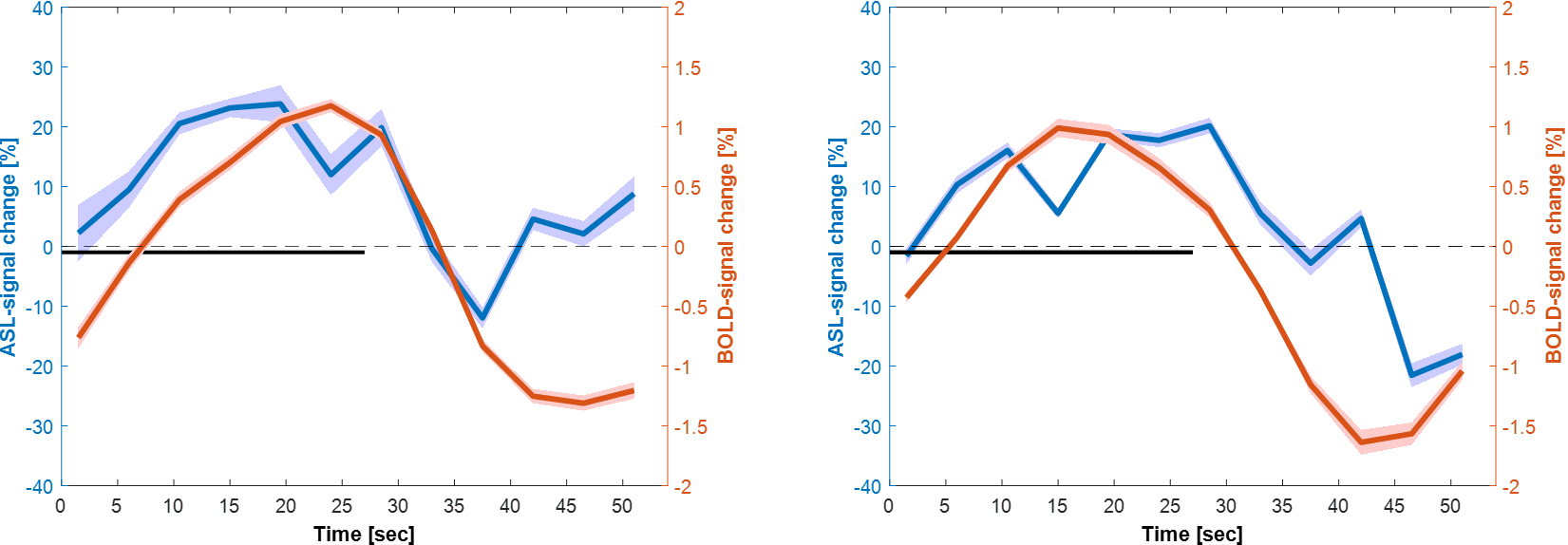
Lastly, Figure 5 shows a proof of concept of the use of VSSinv-ASL at UHF for fMRI with a visual stimulation (27s on-27s off, 11 repeats) showing both activation curves in the visual cortex for ASL and BOLD.
Conclusion:
We showed the feasibility of Velocity Selective (VS)ASL at UHF and its potential use in fMRI.Acknowledgements
This project is funded by: TTW-ZonMW-SGF-LHS Human Measurement models grant #18969-Virtual Cerebrovascular Responses.References
1. Teeuwisse WM, Webb AG, van Osch MJ. Arterial spin labeling at ultra‐high field: all that glitters is not gold. International Journal of Imaging Systems and Technology. 2010;20(1):62-70.
2. Zhao C, Shao X, Shou Q, Ma SJ, Gokyar S, Graf C, et al. Whole-Cerebrum distortion-free three-dimensional pseudo-Continuous Arterial Spin Labeling at 7T. NeuroImage. 2023:120251.
3. Kashyap S, Ivanov D, Havlicek M, Huber L, Poser BA, Uludağ K. Sub-millimetre resolution laminar fMRI using Arterial Spin Labelling in humans at 7 T. PLOS ONE. 2021;16(4):e0250504.
4. Qin Q, Alsop DC, Bolar DS, Hernandez‐Garcia L, Meakin J, Liu D, et al. Velocity‐selective arterial spin labeling perfusion MRI: A review of the state of the art and recommendations for clinical implementation. Magnetic Resonance in Medicine. 2022;88(4):1528-47.
5. Koloskov V, Brink W, Webb A, Shchelokova A. Flexible metasurface for improving brain imaging at 7T. arXiv preprint arXiv:231020019. 2023.
6. Guo J. Robust dual‐module velocity‐selective arterial spin labeling with velocity‐selective saturation and inversion. Magnetic Resonance in Medicine. 2023;89(3):1026-40.
Figures