2008
Quantitative measurement of renal arterial spin labeling: a noninvasive indicator of perfusion in renal artery stenosis1Department of Radiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, China, 2Department of Radiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 3MR Research Collaboration, Siemens Healthineers Ltd., Beijing, China, 4MR Application Predevelopment, Siemens Healthcare GmbH, Beijing, China
Synopsis
Keywords: Arterial Spin Labelling, Perfusion
Motivation: There are few validated noninvasive indicators for renal perfusion and renal function in patients with renal artery stenosis (RAS)
Goal(s): To explore the utility of arterial spin labeling (ASL) as a noninvasive indicator of renal perfusion and function in patients with RAS.
Approach: We evaluated correlations between ASL-measured preoperative renal blood flow (RBF) and renal function, then compared preoperative and postoperative RBF.
Results: ASL-measured RBF was significantly correlated with renal function. ASL was able to evaluate perfusion improvement in patients with RAS after interventional therapy.
Impact: ASL can be used as an indicator of renal function and perfusion in patients with RAS. It can also be used to assess changes in renal perfusion after interventional therapy.
Introduction
Renal artery stenosis (RAS) is the most common cause of secondary hypertension1. Severe narrowing of both renal arteries can lead to serious consequences, such as end-stage renal failure2. Digital subtraction angiography, the gold standard for diagnosis of RAS, can also be used for interventional treatment. However, digital subtraction angiography cannot evaluate renal perfusion and function. The estimation of glomerular filtration rate (GFR) based on serum creatinine (i.e., eGFR) is a simple method for evaluating renal function, but it does not evaluate renal function in a single kidney. Although renal dynamic imaging-derived GFR can evaluate renal function in a single kidney, this approach is expensive and may exacerbate renal impairment. Advances in magnetic resonance imaging technology have enabled arterial spin labeling (ASL)-based quantitative assessments of renal function and perfusion; this approach has not been used to evaluate RAS 3. Therefore, this study was performed to assess the utility of ASL as a noninvasive indicator of renal perfusion in patients with RAS, then explore improvements in perfusion after interventional therapy.Method
Eleven patients with digital subtraction angiography-confirmed RAS were enrolled in this study; all patients were scheduled for interventional therapy. All patients underwent preoperative ASL examination on a 3T scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany); seven patients returned for postoperative ASL examination. For data acquisition, ASL was obtained using an investigational three-dimensional turbo gradient spin echo sequence and pseudo-continuous ASL approach in the coronal plane. Quantitative renal blood flow (RBF) maps were generated in-line after data acquisition. In total, 22 renal arteries and kidneys were individually analyzed by division into groups according to the degree of renal artery stenosis: none, mild (≤75%), and severe (>75%). We collected clinical data, including preoperative and postoperative systolic and diastolic blood pressures, preoperative eGFR, and single-kidney GFR. RBF values in the renal parenchyma and regions of abnormal perfusion were measured by freehand delineation of regions of interest (ROI) on preoperative and postoperative RBF maps. Regions of abnormal perfusion were subjectively evaluated by a radiologist. We compared preoperative RBF values among the three groups, assessed the relationship between preoperative RBF and preoperative single-kidney GFR, and analyzed differences between preoperative and postoperative RBF.Result
All patients with RAS exhibited lower systolic and diastolic blood pressures after therapy. RBF in the renal parenchyma was highest in the no stenosis group, followed by the mild stenosis group; it was significantly reduced in the severe stenosis group (273.68±62.77 (ml/ (100 ml*min)) vs 187.33±49.66 (ml/ (100 ml*min)) vs 156.77±75.21 (ml/ (100 ml*min)); p<0.05). Preoperative RBF in the renal parenchyma was positively correlated with preoperative single-kidney GFR (r=0.504, p=0.024); there were no significant correlations between preoperative RBF and preoperative estimated GFR. In the renal parenchyma, postoperative RBF was higher than preoperative RBF (203.19±51.42 (ml/ (100 ml*min)) vs.164.00±68.10 (ml/ (100 ml*min)); p=0.005). In regions of abnormal perfusion, postoperative RBF was also higher than preoperative RBF (159.92±46.10 (ml/ (100 ml*min)) vs. 108.55±39.57 (ml/ (100 ml*min)); p=0.001).Discussion
This study showed that ASL-measured RBF was a noninvasive indicator of renal perfusion in patients with RAS. RBF in the renal parenchyma was significantly correlated with unilateral renal function; increases in RBF after interventional therapy could be used to evaluate improvements in renal perfusion. Currently, GFR is the metric most commonly used to assess renal function; it can be estimated by blood creatinine clearance, but estimated values do not reflect unilateral renal function. Among patients with RAS, inconsistency in the degree of bilateral RAS can lead to dissimilar renal perfusion injury between kidneys4. Initially, unilateral renal perfusion may be reduced, but eGFR values remain normal. When a decrease in eGFR finally becomes evident, the renal structure may have undergone irreversible damage5. This study shows that RBF can be used to identify unilateral decline in renal function and facilitate early intervention in affected patients. Additionally, this study showed that RBF increased after interventional therapy in patients with RAS, suggesting that ASL can serve as an indicator of perfusion improvement after interventional therapy.Conclusion
ASL-measured RBF was significantly correlated with single-kidney GFR and could be used to evaluate improvements in perfusion among patients with RAS after interventional therapy.Acknowledgements
NoReferences
1 R.D. Safian. Renal artery stenosis. Prog Cardiovasc Dis. 2021; 6560-70.
2 V. Aboyans, I. Desormais, J. Magne, et al. Renal Artery Stenosis in Patients with Peripheral Artery Disease: Prevalence, Risk Factors and Long-term Prognosis. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2017; 53(3):380-385.
3 J.L. Zhang, V.S. Lee. Renal perfusion imaging by MRI. J Magn Reson Imaging. 2020; 52(2):369-379.
4 C. Cuspidi, R. Dell'Oro, C. Sala, et al. Renal artery stenosis and left ventricular hypertrophy: an updated review and meta-analysis of echocardiographic studies. Journal of hypertension. 2017; 35(12):2339-2345.
5 S. Manohar, A. Hamadah, S.M. Herrmann, et al. Total Renal Artery Occlusion: Recovery of Function After Revascularization. Am J Kidney Dis. 2018; 71(5):748-753.
Figures
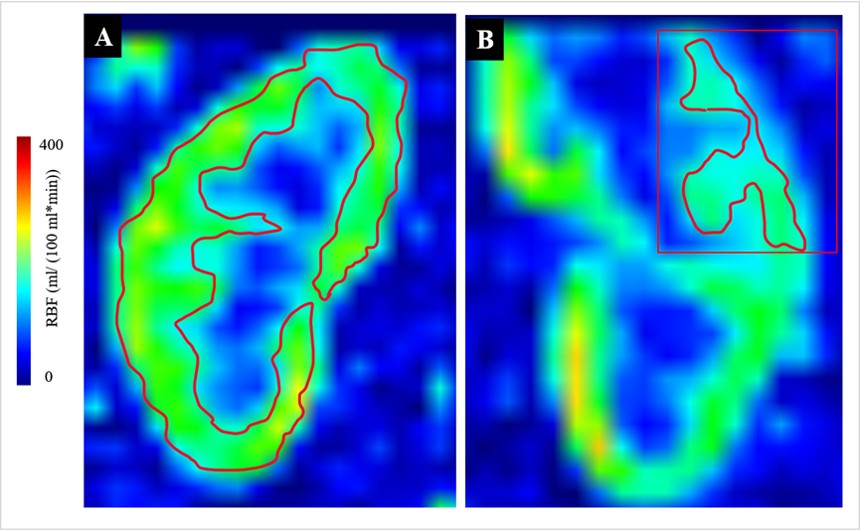
Figure 1 Schematic representation of ROI. Figure A demonstrates the ROI measuring the RBF in the renal parenchyma, figure B demonstrates the ROI measuring the RBF in the region of abnormal perfusion. The region of abnormal perfusion refers that the perfusion of the region is significantly lower than other region in the renal parenchyma.
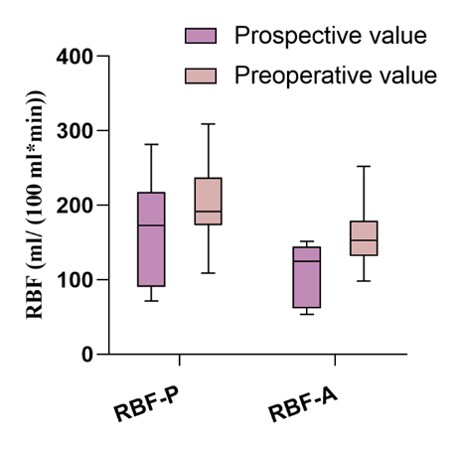
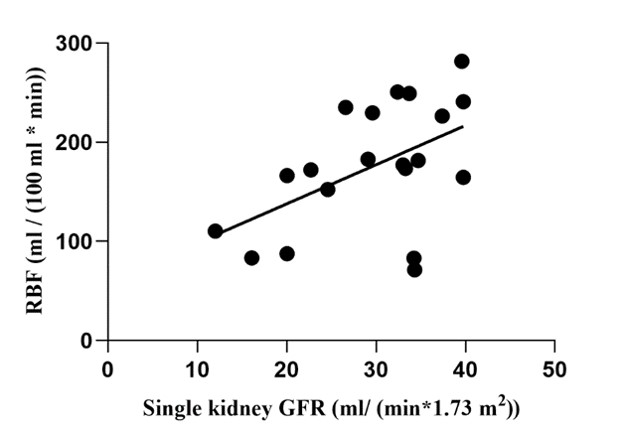
Figure 3 Scatterplot of single-kidney GFR and RBF. There was a positive correlation between RBF in the renal parenchyma and single-kidney GFR (r=0.504, p=0.024).
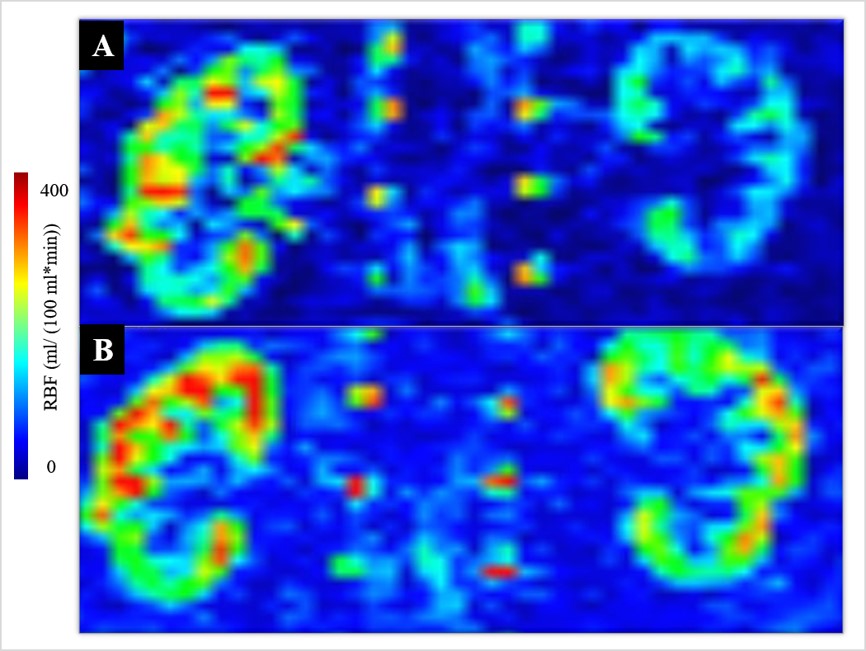
Figure 4 Preoperative and postoperative ASL images of a 53-year-old man. Preoperative RBF image shows severely impaired perfusion in the left kidney (A). At 2 months after left renal artery stenting, ASL examination revealed substantially improved perfusion in the left kidney (B).