2002
Renal multiple post label times arterial spin label (ASL) read out by turbo spin echo (TSE)1School of Biomedical Engineering, Southern Medical University, Guangzhou, China, 2Guangdong Provincial Key Laboratory of Medical Image Processing, Southern Medical University, Guangzhou, China, 3Guangdong Provincial Engineering Laboratory for Medical Imaging and Diagnostic Technology, Southern Medical University, Guangzhou, China, 4Department of Rehabilitation, Zhujiang Hospital, Southern Medical University, Guangzhou, China, 5Medical Imaging Center, Nanfang Hospital, Southern Medical University, Guangzhou, China, 6Philips Healthcare, Shenzhen, China, 7Philips Healthcare, Guangzhou, China, 8Philips Healthcare, Shanghai, China
Synopsis
Keywords: Arterial Spin Labelling, Arterial spin labelling
Motivation: Renal imaging using echo planar imaging (EPI) readout may be sensitive to field inhomogeneities and induced ghost artifact. Besides, single inversion time is not enough for renal blood flow (RBF) quantification. Investigation of more stable clinical arterial spin label (ASL) imaging methods is required.
Goal(s): We aimed to design a stable clinical ASL sequence to quantify RBF accurately.
Approach: Multiple inversion time (TIs) readout by turbo spin echo (TSE) was processed, and the repeatability of quantification was evaluated in volunteers (n=7).
Results: Multiple TIs combined with TSE readout of FAIR-ASL provided more accurate RBF measurement and highly repeatability compare with pcASL-EPI.
Impact: Multi-PLDs readout by TSE may provide a stable clinical ASL-FAIR sequences to accurately quantify RBF.
Introduction
Functional imaging of blood flow, such as ASL[1], is sensitive to renal injury or disease[2]. Current clinical single–PLD ASL-EPI sequences are unstable and poorly repeatable and difficult to quantify renal blood flow. In this abstract, we designed renal multi-TI-ASL sequence readout by TSE and verified its stability and repetition in clinical measurement of RBF.Method
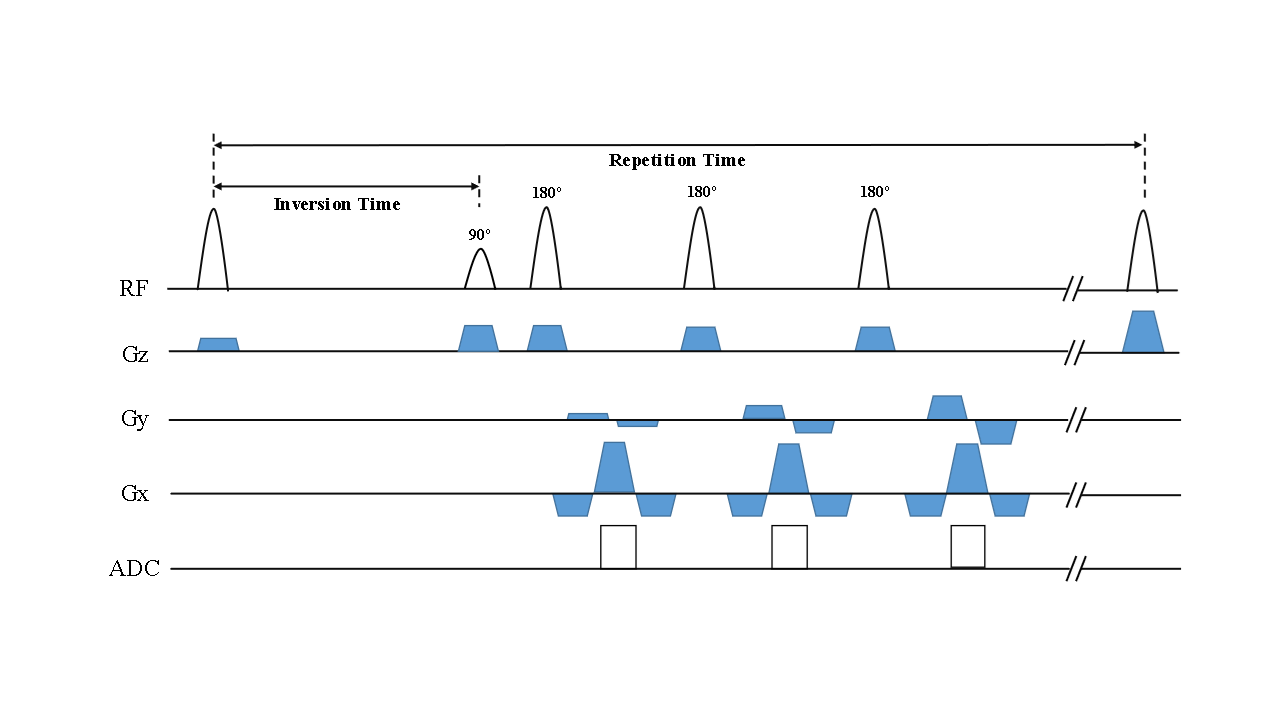
Sequence design: Figure 1 shows the sequence design in this study. The sequence consists of two components: the label module and the readout module. The label pulse consisted by an adiabatic flip pulse, which reduces the effect of B1 inhomogeneities.MRI: This experiment was approved by local institutional Review Board. MRI data were acquired in seven healthy volunteers (n=7) under breath hold on a Philips 3.0T scanner(Ingenia , Philips Healthcare, Best, The Netherlands)equipped with 32 channels torso coil. MRI examination was performed twice with one week interval to test the feasibility and repeatability. The ASL-FAIR sequence used the following acquisition parameters: FOV = 384 x 384 mm2, matrix= 256x256, resolution = 1.5x1.5 mm2, slice thickness = 5 mm, label thickness = 15 mm, control thickness = 500 mm, TR/TE = 4500/5.1 ms, single-shot TSE. In addition, single slice imaging was conducted for signal sampling of 9TIs (300,600,900,1200,1500,1800,2100,2400 and 3000ms).
Data Analysis: The image processing and analyses were performed on MATLAB R2022b(The MathWorks,Natick,MA). The images were registered by principal component analysis (PCA) using Elastix[3], and de-noised by Non-Local Means. Then, the images were fitted by inversion recovery T1 model. The perfusion measurements of the kidney were calculated by the classic Buxton model [4]. Subsequently, the renal cortex region of interests (ROIs) were determined manual on the T1mapping image and applied to all registered datasets.
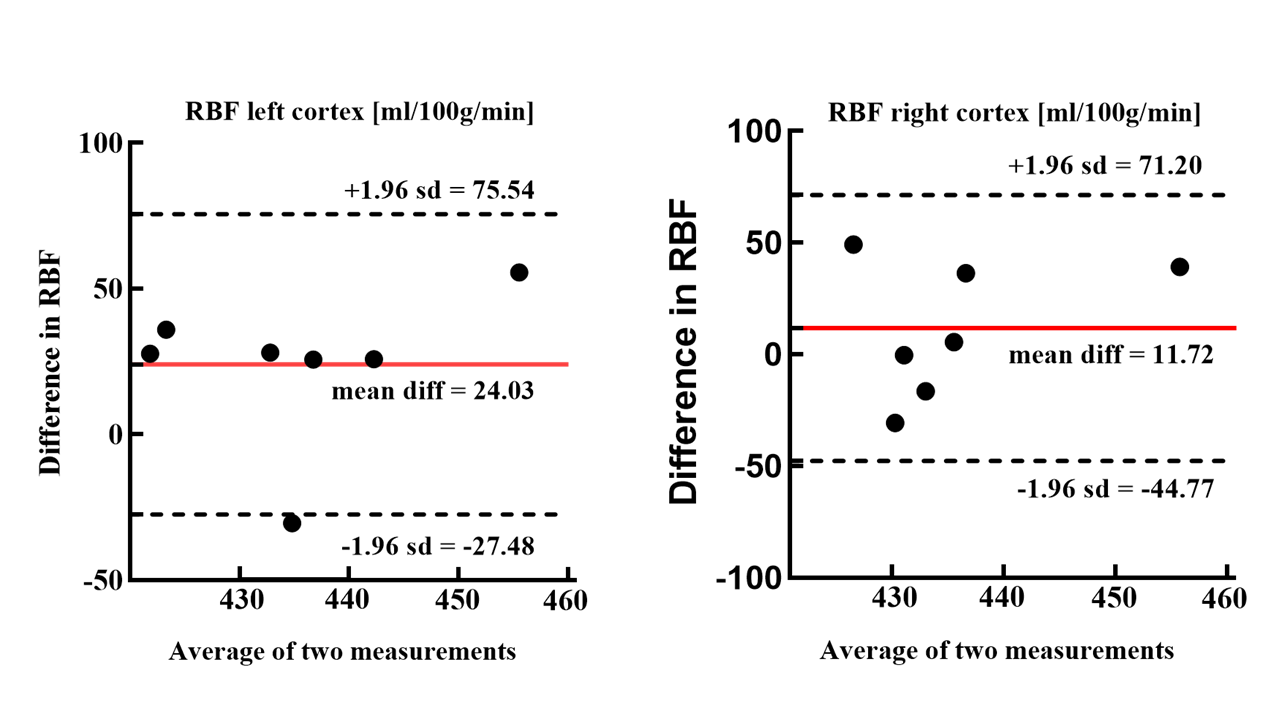
Statistical Analysis: The RBF value was expressed as mean ± standard deviation (SD). We used Bland-Altman to test the reproducibility, with confidence intervals set at 5%.
Results
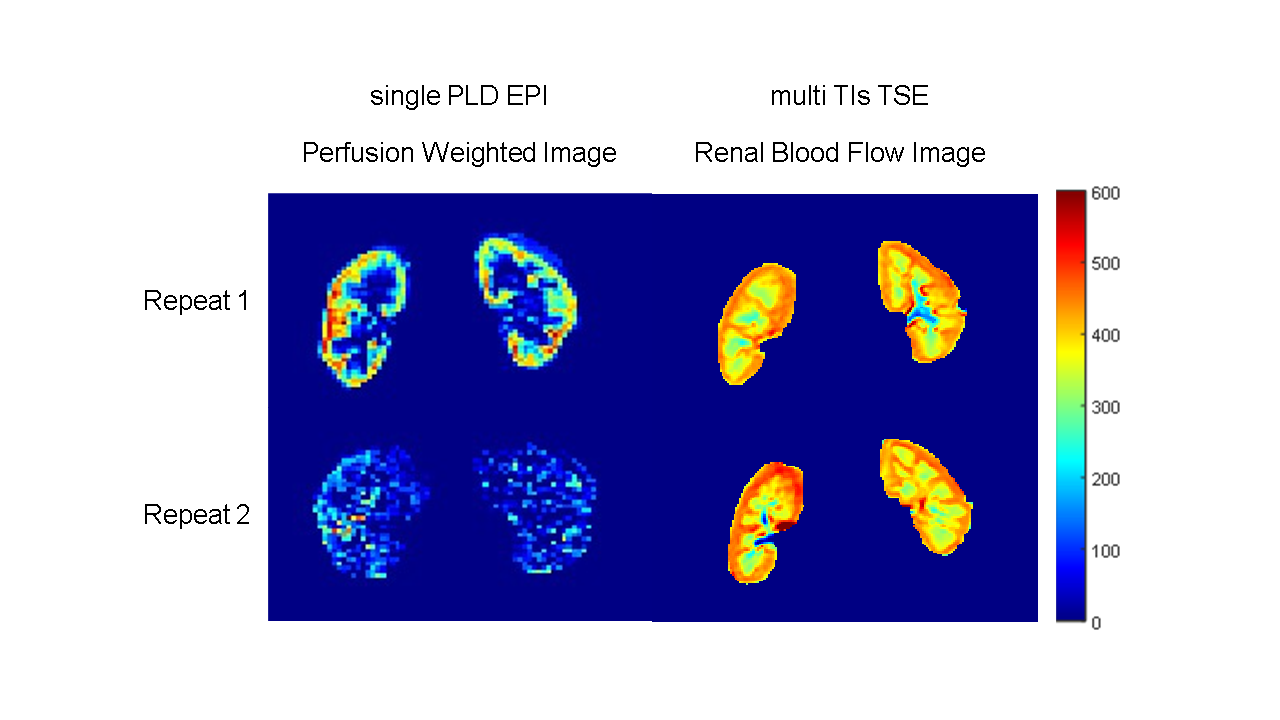
The cortical RBF of healthy subjects is 435.30 ± 20.895 mL/100 g/min for the left renal cortex and 432.08 ± 20.934 mL/100 g/min for the right kidney. Figure 2 shows the perfusion-weighted images and RBF maps imaged by single-PLD-EPI and multi-TI-TSE, respectively. The multi-TI-TSE approach produces a renal RBF image with a well-defined renal structure and distinct borders at two scanning, however, the perfusion-weighted images exhibited blurred boundaries and poor image quality at re-scan. The Bland-Altman analysis showed that the all volunteers’ RBF measured by multi-TI-TSE ASL are all within the 95% confidence interval (Figure 3), which indicates the high stability and repeatability of our sequence.Discussion
Renal blood flow (RBF) is a potential indicator for kidney disease detection. This study provided a stable and highly repeatable measurement approach, which is beneficial for clinical applications. However, there are some limitations to this study. The first is the problem of motion, which requires an accurate registration method. The second is that the model utilizes a single-compartment model, which only considers the inflow and outflow of blood flow, with no internal transformations. More investigations on model simulation and motion correction are needed.Conclusion
Our work validates the effectivity of multiple TI/PLD FAIR for RBF imaging. This sequence has been demonstrated that with great stability and repeatability in healthy volunteers.Acknowledgements
This study was supported by National Natural Science Foundation of China (U21A6005), Key-Area Research and Development Program of Guangdong Province (2018B030340001, 2018B030333001).References
1.Detre JA, Leigh JS, Williams DS, Koretsky AP. Perfusion imaging. Magn Reson Med. 1992 Jan;23(1):37-45.
2.Taso M, Aramendía-Vidaurreta V, Englund EK, Francis S, Franklin S, Madhuranthakam AJ, Martirosian P, Nayak KS, Qin Q, Shao X, Thomas DL, Zun Z, Fernández-Seara MA; ISMRM Perfusion Study Group. Update on state-of-the-art for arterial spin labeling (ASL) human perfusion imaging outside of the brain. Magn Reson Med. 2023 May;89(5):1754-1776.
3.Klein S, Staring M, Murphy K, Viergever MA, Pluim JP. elastix: a toolbox for intensity-based medical image registration. IEEE Trans Med Imaging. 2010 Jan;29(1):196-205.
4.Buxton RB, Frank LR, Wong EC, Siewert B, Warach S, Edelman RR. A general kinetic model for quantitative perfusion imaging with arterial spin labeling. Magn Reson Med. 1998 Sep;40(3):383-96.
Figures