2001
Arterial spin labeling in assessment of interstitial fibrosis in renal allografts1The First Affiliated Hospital of Soochow University, Suzhou, China, 2Philips Healthcare, Shanghai, China
Synopsis
Keywords: Arterial Spin Labelling, Arterial spin labelling, renal transplantation
Motivation: Renal interstitial fibrosis, a prevalent, irreversible, progressive chronic kidney injury, emerges as a crucial prognostic determinant for kidney transplantation.
Goal(s): To explore the feasibility and performance of arterial spin labeling (ASL) in evaluating the degree of renal fibrosis after renal transplantation.
Approach: ASL was performed on 64 renal transplantation recipients. ASL parameters were obtained and analyzed.
Results: The study revealed a noteworthy negative correlation between the measured renal blood flow values, obtained through ASL, and the degree of interstitial fibrosis in transplanted kidneys. ASL can effectively differentiate various degrees of fibrosis in transplanted kidneys.
Impact: Using ASL technology, it is possible to non-invasively assess the degree of fibrotic changes in transplanted kidneys and the progression of kidney function, thereby achieving early detection, diagnosis, and treatment.
Introduction
Chronic kidney injury limits the lifespan of transplanted kidneys and frequently results in graft dysfunction or failure [1]. Interstitial fibrosis (IF) is a prevalent type of chronic kidney injury in transplanted kidneys. Renal allograft biopsy currently serves as the gold standard for assessing fibrosis degree in transplanted kidneys. However, its invasive nature and sampling limitations of biopsy specimens pose constraints. Additionally, fibrosis exhibits non-uniform distribution within the transplanted kidney, and the obtained biopsy sample may not accurately represent the overall extent of renal fibrosis [2].In recent years, the application of functional magnetic resonance imaging (MRI) in transplanted kidneys has provided new opportunities for integrating anatomical imaging with multi-parametric functional information [3]. Arterial spin labeling (ASL), using blood as an endogenous contrast agent, allows for perfusion measurement without the use of exogenous contrast agents. Previous studies have demonstrated the comparable values of measured renal blood flow (RBF) using ASL to the gold standard [4]. This study aims to explore the feasibility and performance of ASL in evaluating the extent of interstitial fibrosis in transplanted kidneys.Methods
We prospectively enrolled 60 renal transplant recipients with indications for renal allograft biopsy from December 2021 to December 2022. Based on the Banff fibrosis score (ci score) results, all participants were divided into four groups: ci0 group with a fibrosis score of ci=0, 11 patients; ci1 group with a fibrosis score of ci=1, 21 patients; ci2 group with a fibrosis score of ci=2, 20 patients; and ci3 group with a fibrosis score of ci=3, 8 patients. MRI was performed using a Philips 1.5T MRI scanner (Ingenia Ambition, Philips Healthcare, Best, the Netherlands) equipped with a 28-channel phased array body coil. The scanning sequence includes ASL, T1-weighted (T1WI), and T2-weighted (T2WI) imaging sequences. The imaging parameters of ASL were as follows: TR=3963 ms; TE=15 ms; voxel size=3.75×3.75×8 mm3; FOV=240×240×88 mm3; TSE factor=20; EPI factor=15; eight dynamics. The renal cortical RBF values were obtained through the workstation (Philips Healthcare Intellispace Portal v10 workstation) by two senior radiologists. Statistical analysis was performed using SPSS 25.0 software. One-way analysis of variance was used to compare the differences in cortical RBF values between different groups. Spearman correlation analysis was used to determine the correlation between RBF values and the transplanted kidney's interstitial fibrosis scores. Receiver operating characteristic curve analysis was performed to assess the diagnostic value of MRI parameters in differentiating the degree of fibrosis in transplanted kidneys. P<0.05 indicated statistical significance.Results
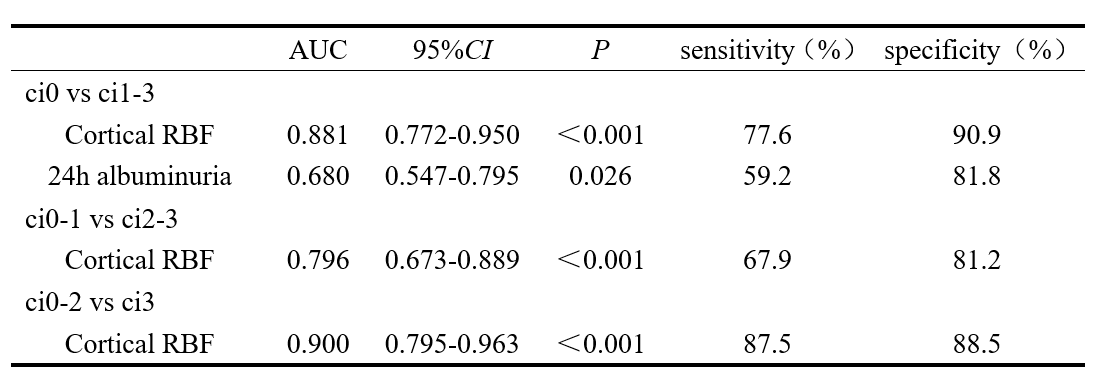
The RBF values tended to decrease with the severity of renal fibrosis (Figure 1,2). The RBF values were moderately inversely correlated with the Banff fibrosis scores (r=-0.644). The AUCs of RBF and 24-hour albuminuria for distinguishing between ci0 and ci1-3 were 0.881 and 0.680, respectively. The AUC of RBF was higher than that of 24-hour albuminuria. RBF could diagnose renal allograft fibrosis ci2-3 and ci3 with AUC of 0.796 (95%CI, 0.673 to 0.889) and 0.900 (95%CI, 0.795 to 0.963), respectively (Table 1).Discussion
The findings in the study are consistent with those of Yu YM et al. [5], who compared the value of ASL and IVIM in evaluating the degree of fibrosis in transplanted kidneys. They found that ASL was more sensitive to fibrotic changes than IVIM. This suggests that changes in perfusion were more significant than water diffusion restriction caused by fibrous matrix deposition in the process of fibrosis. Interstitial fibrosis is a common finding in transplanted kidneys and is often associated with renal dysfunction [6]. In our study, we found a significant reduction in the estimated glomerular filtration rate (eGFR) in the severe fibrosis group (ci3) compared to the progressive fibrosis group (ci0-2). However, despite the correlation between eGFR and interstitial fibrosis, several studies have reported the occurrence of interstitial fibrosis in transplanted kidneys with normal renal function [7]. Additionally, Wang W et al. [8] found a significant decrease in cortical RBF values in transplanted kidneys with underlying pathological changes compared to histologically normal transplanted kidneys. Notably, there was no significant difference in eGFR between the two groups. It indicated that RBF was more sensitive than eGFR in detecting renal dysfunction in transplanted kidneys, including subclinical lesions. Hence, ASL may have advantages over eGFR for assessing renal fibrosis.Conclusion
ASL can be applied for non-invasive evaluation of renal graft fibrosis and thus can be used as an important supplementary examination before transplantation.Acknowledgements
No acknowledgement found.References
[1] Solez K, Colvin RB, Racusen LC, et al. Banff '05 Meeting Report: differential diagnosis of chronic allograft injury and elimination of chronic allograft nephropathy ('CAN'). Am J Transplant, 2007, 7(3): 518-526. DOI: 10.1111/j.1600-6143.2006.01688.x.
[2] Kirpalani A, Hashim E, Leung G, et al. Magnetic Resonance Elastography to Assess Fibrosis in Kidney Allografts. Clin J Am Soc Nephrol, 2017, 12(10): 1671-1679. DOI: 10.2215/CJN.01830217.
[3] Friedli I, Crowe LA, Berchtold L, et al. New magnetic resonance imaging index for renal fibrosis assessment: A comparison between diffusion weighted imaging and T1 mapping with histological validation. Sci Rep, 2016, 6: 30088. DOI: 10.1038/srep30088.
[4] Cai YZ, Li ZC, Zuo PL, et al. Diagnostic value of renal perfusion in patients with chronic kidney disease using 3D arterial spin labeling. J Magn Reson Imaging, 2017, 46(2): 589-594. DOI: 10.1002/jmri.25601.
[5] Yu YM, Wang W, Wen J, et al. Detection of renal allograft fibrosis with MRI: arterial spin labeling outperforms reduced field-of-view IVIM. Eur Radiol, 2021, 31(9): 6696-6707. DOI: 10.1007/s00330-021-07818-9.
[6] Rodríguez-Iturbe B, Johnson RJ, Herrera-Acosta J. Tubulointerstitial damage and progression of renal failure. Kidney Int Suppl, 2005, 99: S82-S86. DOI: 10.1111/j.1523-1755.2005.09915.x.
[7] Ix JH, Katz R, Bansal N, et al. Urine Fibrosis Markers and Risk of Allograft Failure in Kidney Transplant Recipients: A Case-Cohort Ancillary Study of the FAVORIT Trial. Am J Kidney Dis, 2017, 69(3): 410-419. DOI: 10.1053/j.ajkd.2016.10.019.
[8] Wang W, Yu Y, Li X, et al. Early detection of subclinical pathology in patients with stable kidney graft function by arterial spin labeling. Eur Radiol, 2021, 31(5): 2687-2695. DOI: 10.1007/s00330-020-07369-5.
Figures
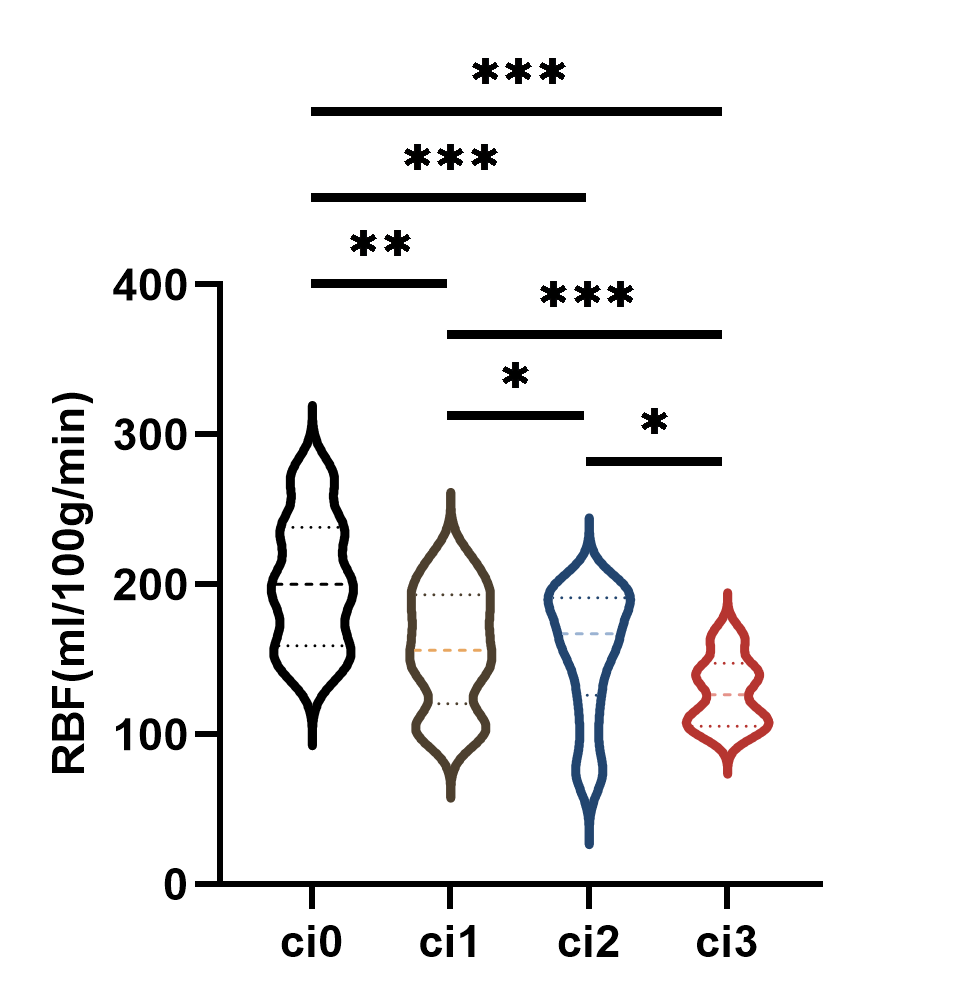
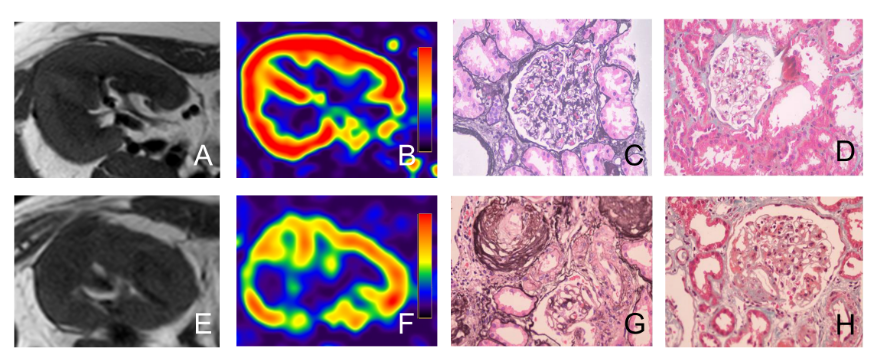
Figure 2. Comparison of MRI and pathologic findings
A-D: male, 39Y, ci score=1, eGFR=86.4ml/min/1.73 m2; E-H: male, 55Y, ci score=3, eGFR=13.9 ml/min/1.73 m2. A, E: T1WI; B, F: cortical RBF maps; C, G: PASM×400; D, H: Masson×400.