1996
Labeling Strategies for Whole-kidney Non-contrast Perfusion-Weighted Imaging using 3D FAIR ASL1Department of Radiology, UT Southwestern Medical Center, Dallas, Texas, TX, United States, 2Advanced Imaging Research Center, UT Southwestern Medical Center, Dallas, Texas, TX, United States
Synopsis
Keywords: Arterial Spin Labelling, Perfusion, FAIR, whole-kidney coverage, quantitative imaging, biomarkers
Motivation: Flow-sensitive alternative inversion (FAIR) is one of the recommended arterial spin labeling (ASL) schemes for renal perfusion. Although FAIR can provide robust measurements, it suffers from partial-kidney coverage especially when aorta is close to or even at the same level of kidney in anterior-posterior (A/P) direction.
Goal(s): To obtain whole-kidney perfusion measurements using 3D FAIR despite anatomy differences within population.
Approach: Two additional labeling strategies of 3D FAIR were proposed and tested in healthy volunteers.
Results: Both strategies generated robust and high-quality perfusion maps with whole-kidney coverage within a feasible clinical scan time, which is challenging for existing 3D FAIR and pCASL implementations.
Impact: Our labeling strategies in 3D FAIR ASL could be valuable for early detection, diagnosis, differentiation, and management of renal diseases, including chronic kidney disease and acute kidney injury, despite individual anatomy differences between patients.
INTRODUCTION
While contrast enhancement methods such as dynamic contrast enhanced (DCE) can be used to measure perfusion in kidney, it is not recommended in patients with impaired renal function [1, 2]. Among all imaging techniques, arterial spin labeling (ASL) is the only method that can be performed without the administration of an exogenous contrast agent. Pseudo-continuous ASL (pCASL) and flow-sensitive alternating inversion recovery (FAIR) are the recommended ASL methods for renal perfusion imaging in the recent consensus [3].3D pCASL has the potential to achieve whole-kidney coverage; however, its labeling efficiency is not robust, which can lead to reduced SNR or complete signal loss [4], especially in areas with increased susceptibility. On the other hand, the labeling of FAIR is more robust, but whole-kidney perfusion of 3D FAIR in coronal acquisition remains challenging due to the proximity of the aorta to the kidneys in anterior-posterior (A/P) direction. This constrains the labeling slab coverage, thus field-of-view coverage, as the labeling slab must avoid covering the aorta in the slice orientation. In this study, we aimed to achieve whole-kidney perfusion measurements with two newly proposed labeling strategies using 3D FAIR within a clinical feasible scan time.
METHODS
METHODS (304 words)Subjects: With IRB approval, four healthy volunteers (mean age, 32 ± 3.9 years) were scanned on a 3T MRI scanner (Ingenia, Philips Healthcare) with supine, feet‐first position. A 16‐channel anterior torso coil and respiratory bellows were used for kidney imaging.
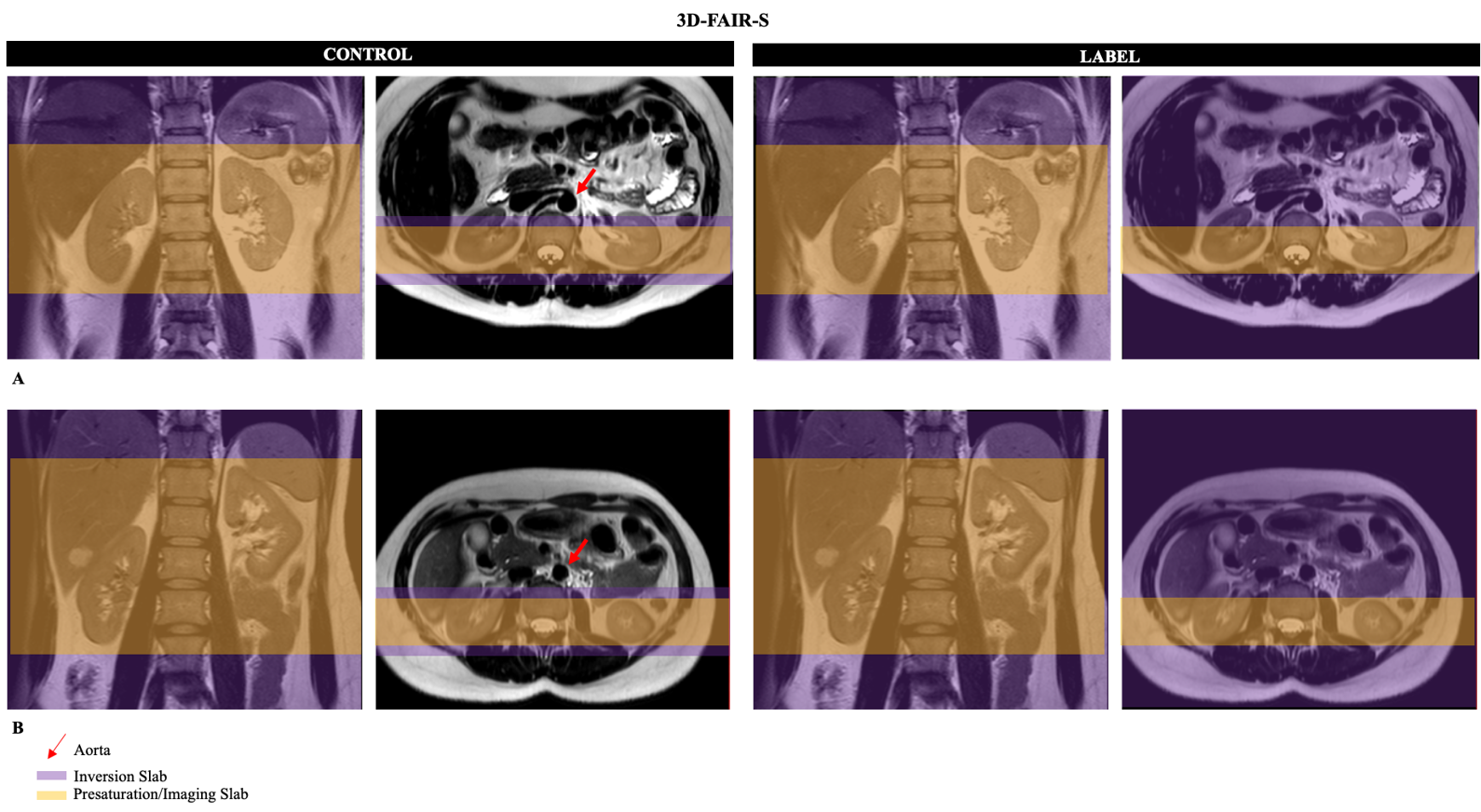
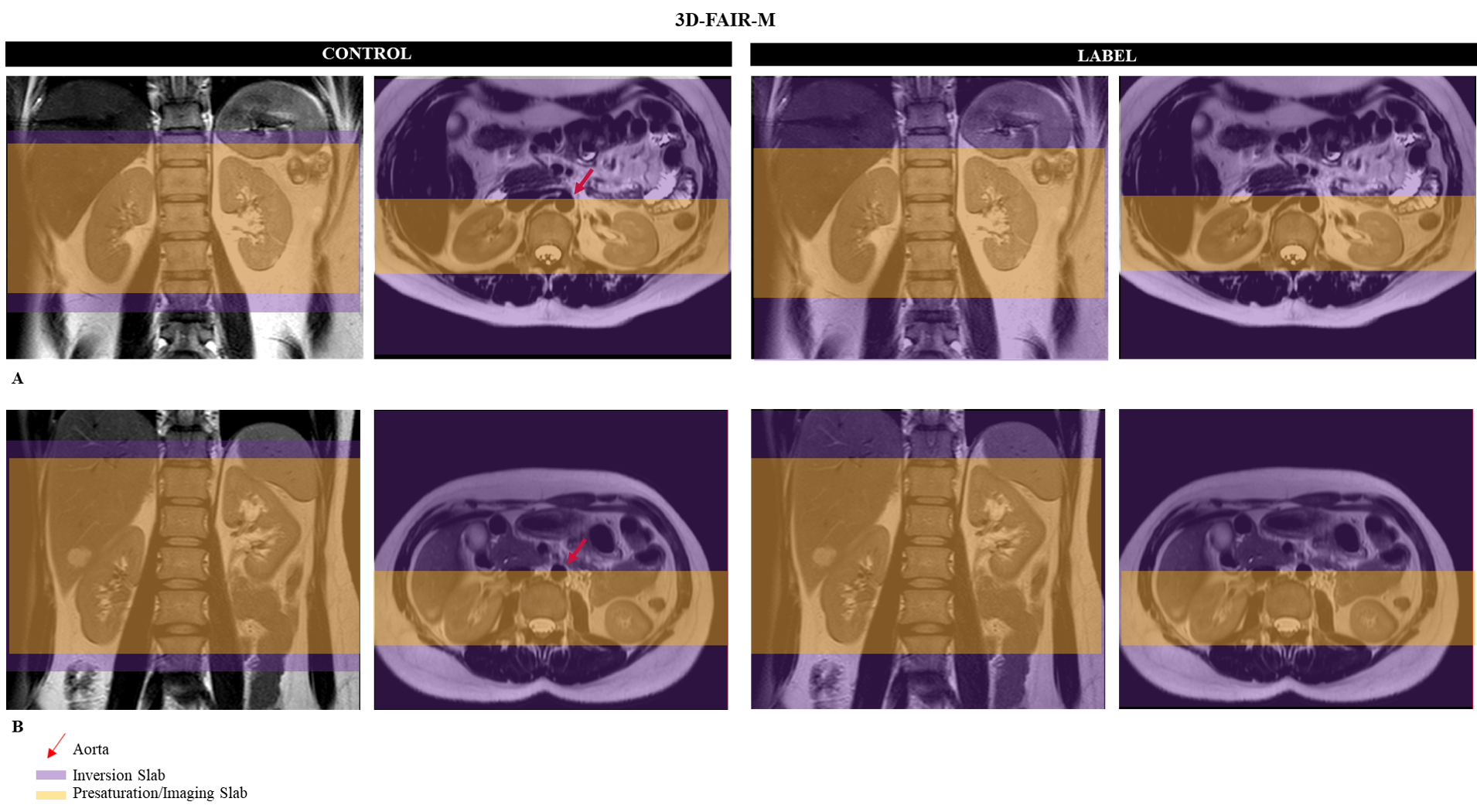
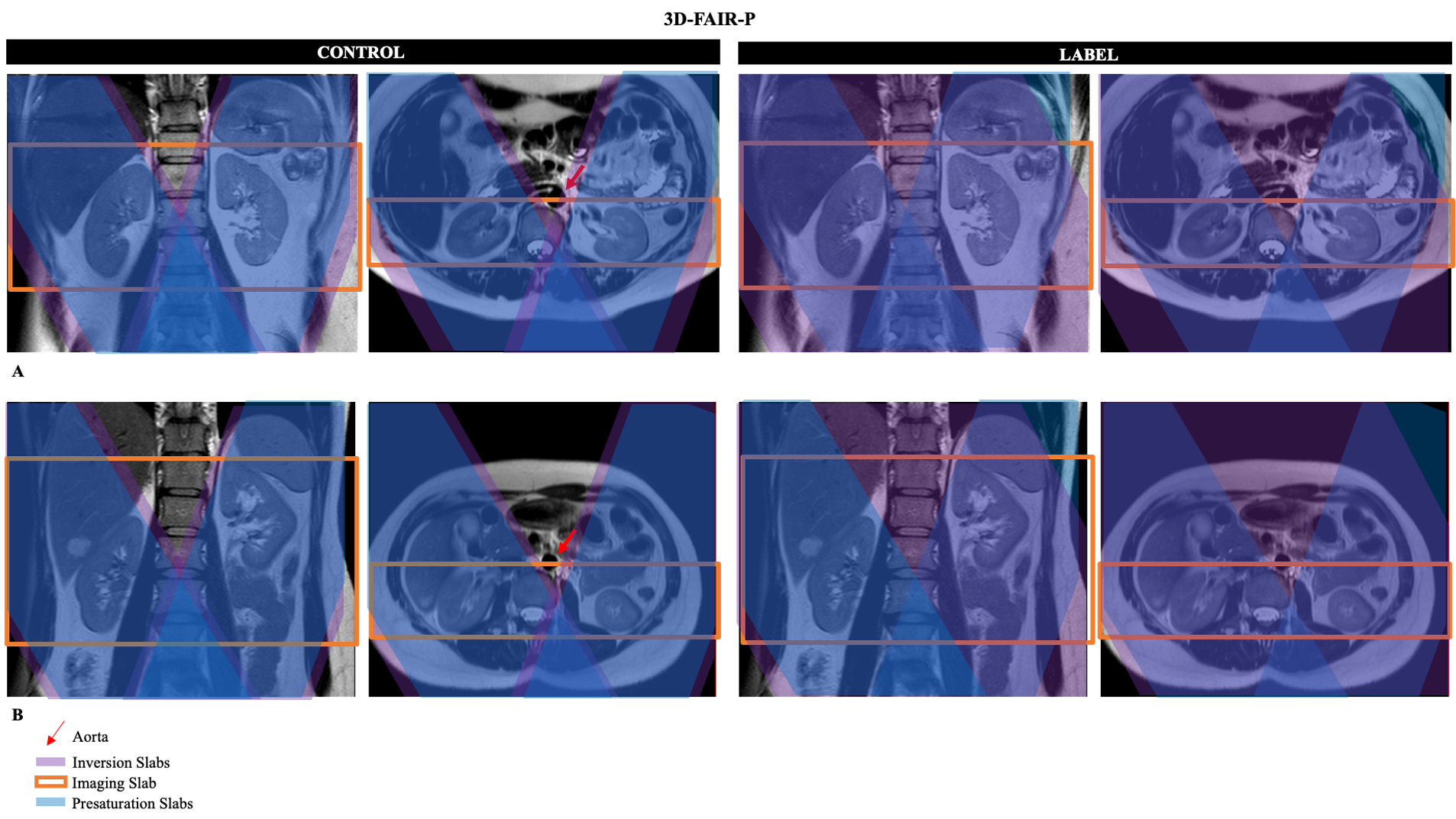
Pulse sequence design: In addition to the existing sequence design where the labeling direction of 3D-FAIR aligns with the slice acquisition direction (3D-FAIR-S for short (Figure 1)), two novel labeling approaches, 3D-FAIR-M (Figure 2) and 3D-FAIR-P (Figure 3) were proposed and implemented. Like the definition of 3D-FAIR-S, the M and P refers to the labeling direction in frequency-encoding (M) and phase-encoding (P), respectively.
Image acquisition: 3D-FAIR sequences with coronal acquisition were performed using three different labeling strategies. Prior to labeling, a series of pre-saturation pulses were performed. Then hyperbolic secant RF pulses were used for inversion/labeling in coronal, axial, and sagittal orientations for 3D-FAIR-S, 3D FAIR-M, and 3D-FAIR-P, respectively. Labeling in sagittal (3D-FAIR-P) used two slabs to selectively label each kidney. Labeling was followed by four background suppression pulses and inflow saturation.
3D TSE based readout with CASPR view reordering [5] was used for FAIR and pCASL with the following imaging parameters: Acquired resolution = 3x3x6mm3, TR/TE = 6500/14 ms, ETL = 120, echo-spacing = 2.8 ms, shot duration = 347 ms; for 3D-FAIR-S, post-label delay = 1.8 s, FOV = 223x372x 40mm3, matrix = 76x124 with 16 slices, acquisition time = 4:07 minutes; for 3D-FAIR-M and 3D-FAIR-P, FOV = 223x372x72 mm3, matrix = 76x124 with 24 slices, acquisition time = 5:25 minutes. 3D-pCASL with coronal acquisition was acquired for comparison with the following parameters: label duration = 1.5 s, post-label delay = 1.5 s, FOV = 223x376x72mm3, matrix = 76x124 with 24 slices, and acquisition time = 5:25 minutes. 3D M0 images with the same parameters were obtained for both FAIR and pCASL.
RESULTS AND DISCUSSIONS
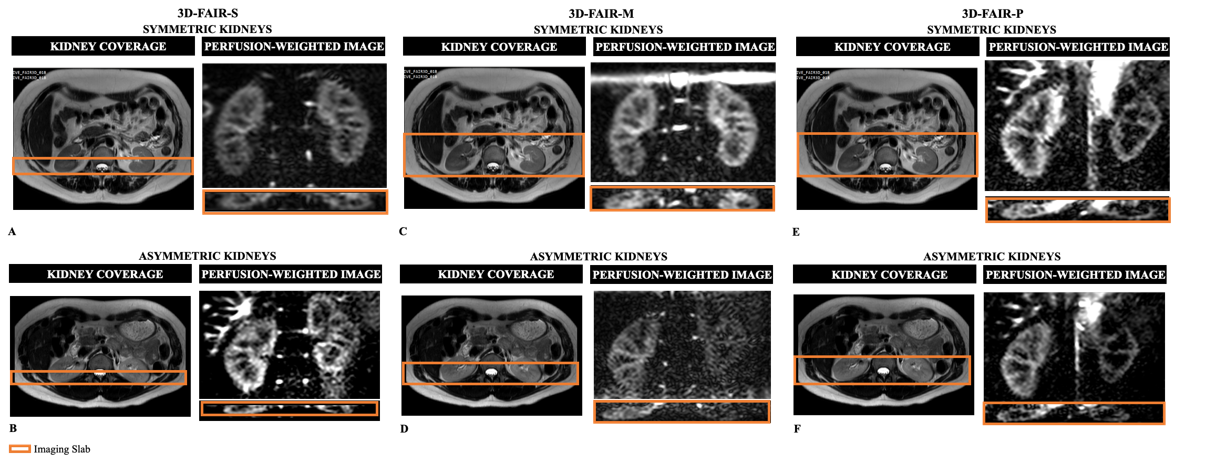
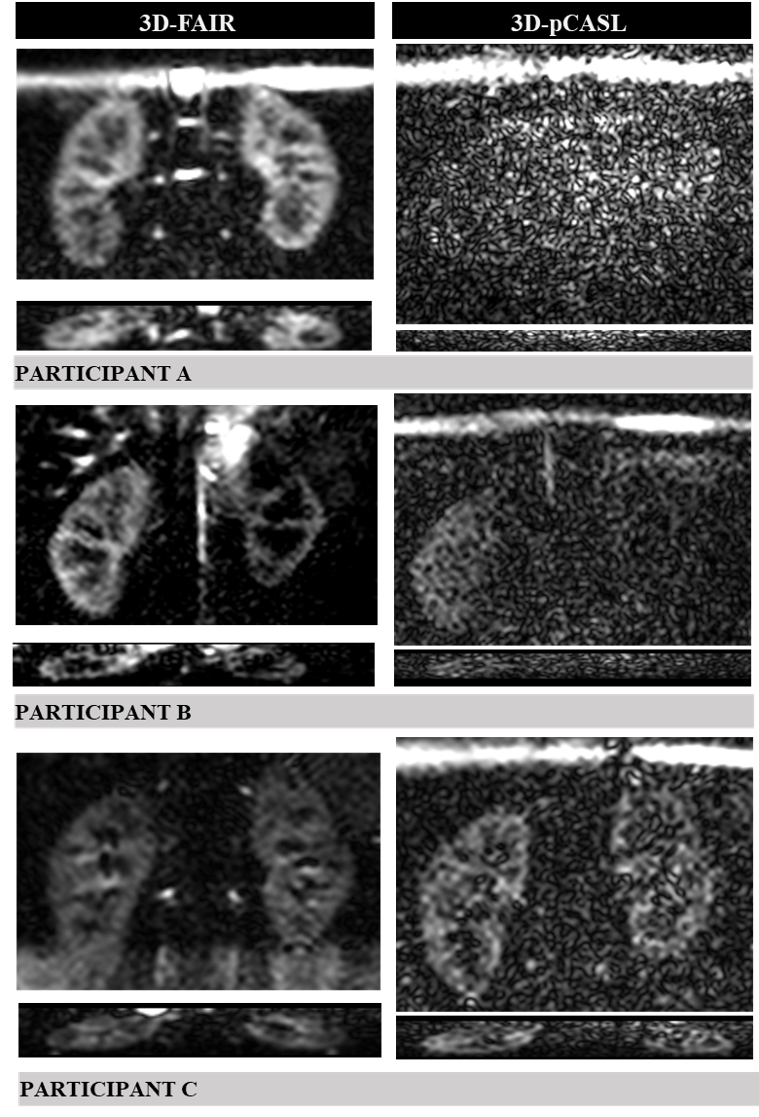
Perfusion maps with good image quality was achieved with 3D-FAIR-S in coronal acquisition (Figure 4A & 4B), yet whole kidney coverage remains challenging, as aorta must be kept outside the inversion slab. The whole kidney coverage became feasible with 3D-FAIR-M, when the kidneys were relatively symmetrical to each other (Figure 4C), since the labeling was applied in axial plane with no constrains of covering the aorta. However, this method began to fail (lower SNR) when the distance between the two kidneys was too large in the foot-head (FH) direction (Figure 4D). For this condition, 3D-FAIR-P served as a good alternative as each kidney was labeled independently in the sagittal plan (Figure 4E & 4F). The labeling slabs were carefully placed, such that they did not cover the aorta during the control acquisition. A slight drawback of 3D-FAIR-P was the poor performance at the edges of the labeling slabs. Future work will use FOCI pulses to achieve slab profiles with sharper edges [6]. Moreover, a consistent higher labeling efficiency was observed with 3D-FAIR among different individuals when compared with 3D-pCASL, probably due to the poor labeling efficiency of the pCASL labeling plane (Figure 5).CONCLUSION
The two novel labeling strategies were able to overcome the partial-kidney coverage challenge presented by the existing implementation of 3D-FAIR. This allowed robust and quantitative measurements of whole-kidney perfusion, which could be valuable for early detection, diagnosis, differentiation, and management of renal diseases.Acknowledgements
This work was partly supported by the NIH/NCI grant U01CA207091. The authors would like to thank all healthy volunteers for their participation in this study. The authors also thank Abey Thomas, RT(MR), Courtney Dawson, RT(MR) and the clinical research office (CRO) for their help in human imaging.
References
REFERENCES
1. Grenier, N., et al., Perfusion imaging in renal diseases. Diagn Interv Imaging, 2013. 94(12): p. 1313-22.
2. Lyske, J., et al., Multimodality imaging review of focal renal lesions. Egyptian Journal of Radiology and Nuclear Medicine, 2021. 52(1): p. 14.
3. Nery, F., et al., Consensus-based technical recommendations for clinical translation of renal ASL MRI. MAGMA, 2020. 33(1): p. 141-161.
4. Greer, J.S., et al., Pseudo-continuous arterial spin labeled renal perfusion imaging at 3T with improved robustness to off-resonance, in International Society for Magnetic Resonance in Medicine (ISMRM). 2019: Montreal, Quebec, Canada.
5. Wang, Y., et al., Volumetric Renal ASL MRI using 3D TSE Cartesian Acquisition with Variable Density Sampling (VD-CASPR), in International Society for Magentic Resonance in Medicine (ISMRM). 2021: online.
6. Yongbi, M.N., C.A. Branch, and J.A. Helpern, Perfusion imaging using FOCI RF pulses. Magnetic Resonance in Medicine, 1998. 40(6): p. 938-943.
Figures