1993
Zero-Shot lung segmentation of Phase-Resolved Functional Lung (PREFUL) MRI from adults and children with pulmonary diseases1Institute of Diagnostic and Interventional Radiology, Hannover Medical School, Hannover, Germany, 2Biomedical Research in Endstage and Obstructive Lung Disease Hannover (BREATH), German Center for Lung Research (DZL), Hannover, Germany
Synopsis
Keywords: AI/ML Software, Segmentation
Motivation: PREFUL MRI relies on accurate lung segmentation. Automating lung segmentation using supervised machine learning requires the laborious creation of training data. Therefore, an alternative independent of availability and peculiarities of training data may be useful.
Goal(s): Investigate feasibility and limits of lung segmentation in PREFUL MRI across different vendors, acquisition parameters, age groups and pulmonary diseases without training data.
Approach: Segment Anything Model (SAM) using different point grids and seedpoint-based prompts was evaluated in overall 14 different configurations.
Results: Comparison with ground truth showed median Dice Similarity Coefficient (DSC) of 0.82 without training data.
Impact: Lung segmentation of PREFUL MRI of child and adult patients with different pulmonary diseases appears feasible without training data. The construction of supervised trained segmentation models may be not mandatory for projects when a median DSC of 0.82 is sufficient.
Introduction
Phase-Resolved–functional–Lung (PREFUL) MRI enables a free-breathing assessment of pulmonary ventilation and perfusion without contrast agents1. A crucial factor for the accuracy of this method is the correct segmentation of the lung parenchyma. Currently, the segmentation is automatized by a supervised trained nnU-Net2. However, supervised Machine Learning of a segmentation task requires the laborious creation of training data. Furthermore, the resulting model may overfit to the training data and fail for image data e.g. depicting pathologies that were underrepresented in the training dataset3.A concurrent strategy to detach the dependencies on availability and peculiarities of training data is Zero-Shot-Segmentation (ZSS). ZSS means the segmentation of image content that the segmentation model was not trained on and relies on a foundation model. Recently Meta AI introduced the Segment Anything Model (SAM), a foundation model for image segmentation4.
Our study assesses the potential of SAM-based ZSS of lung parenchyma in PREFUL MRI across various acquisition settings in adults and children with pulmonary diseases.
Method
Segmentation from 14 different SAM-configurations were compared with a given ground truth (GT) to 2045 PREFUL-MRI images.Datasets
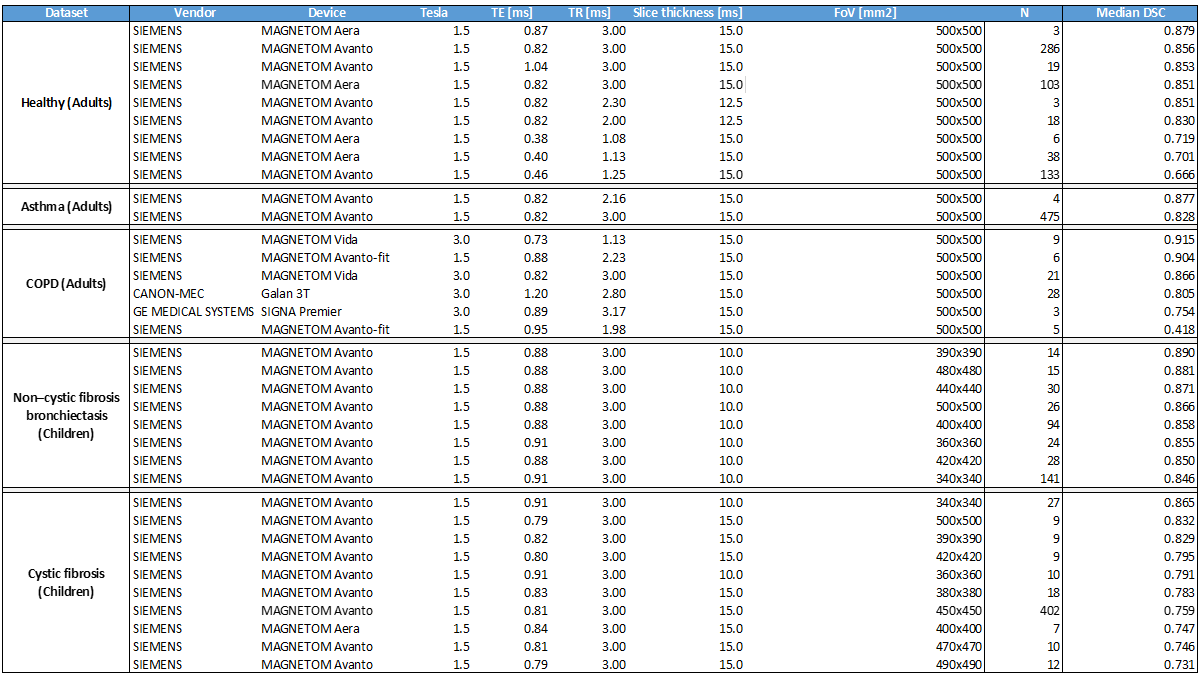
The retrospective analysis encompassed image data acquired using different devices and sequence parameters (see Table2). The data was categorized into two groups of children with pulmonary diseases (Cystic fibrosis, non-CF bronchiectasis), two groups of adults with pulmonary diseases (Asthma, COPD) and one cohort of adult healthy volunteers.
Registration
Next, every series of 200-250 images is registered as described by Voskrebenzev et al.5 Finally, the mean image of the resulting series is the input of the segmentation step.
Segmentation Ground Truth
GT was defined by manually corrected segmentations from the currently used nnU-Net.
SAM configurations
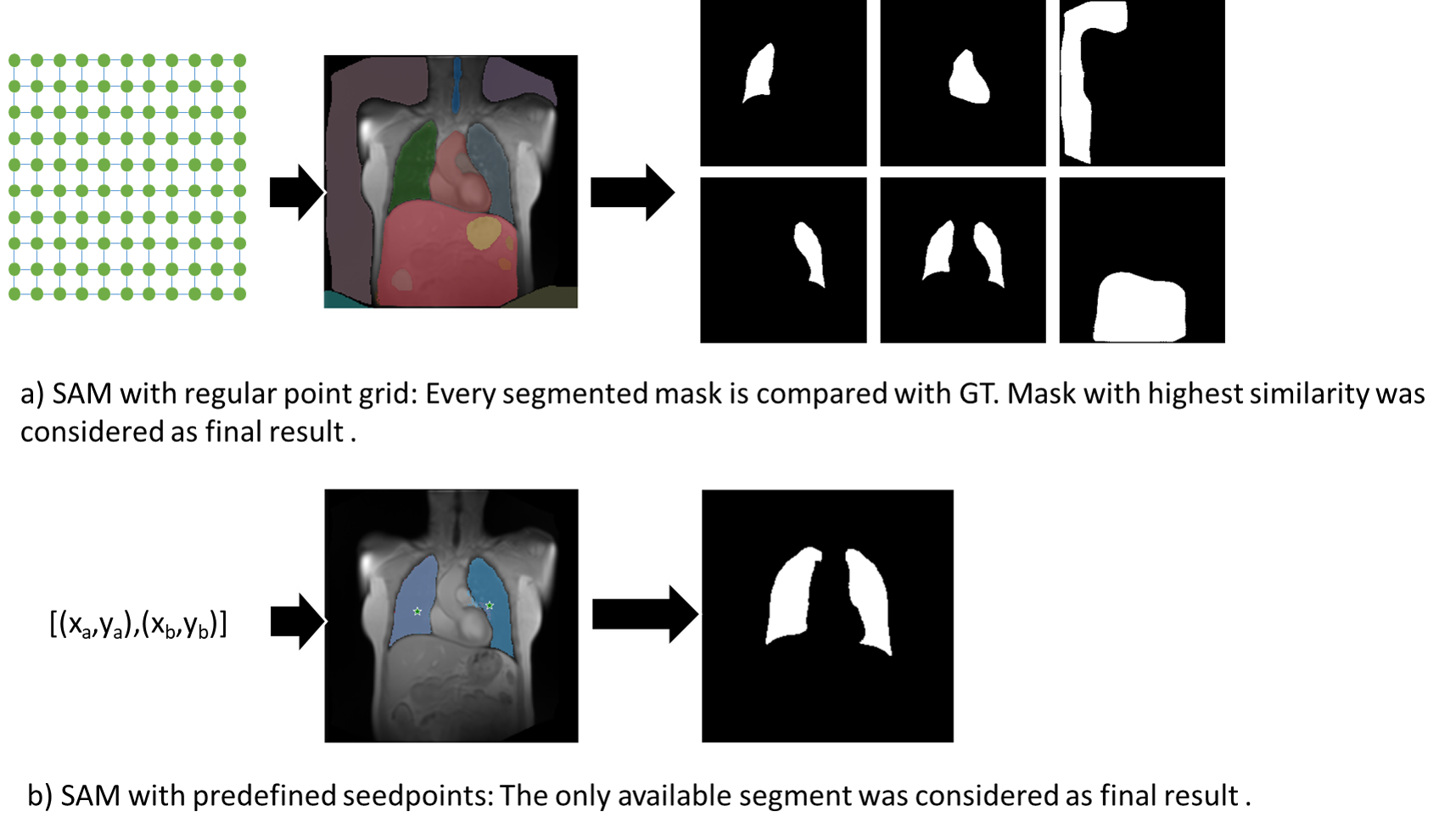
12 regular point grids, automatically defined using four different values for the configuration parameter Points_per_Side (PPS)4 and three different values for Crop_n_Layers (CnL)4 were evaluated as segmentation prompts.
Additionally, one respective two seedpoints within the lung represent a further investigated prompt-definition. To prevent interactive definition for every single image, we used the same seedpoints for every image of the dataset. The coordinates of these seedpoints were previously calculated by averaging the centroid coordinates of left and right lung segment from the corresponding GT of the dataset.
Determining the lung segmentation
Since the automatic variant provides multiple segments, only the segment with the highest Dice Similarity Coefficient (DSC) to the GT was considered as the final segmentation result. For the seedpoint-based variants, no distinction was necessary. Figure1 illustrates this process.
Statistical analysis
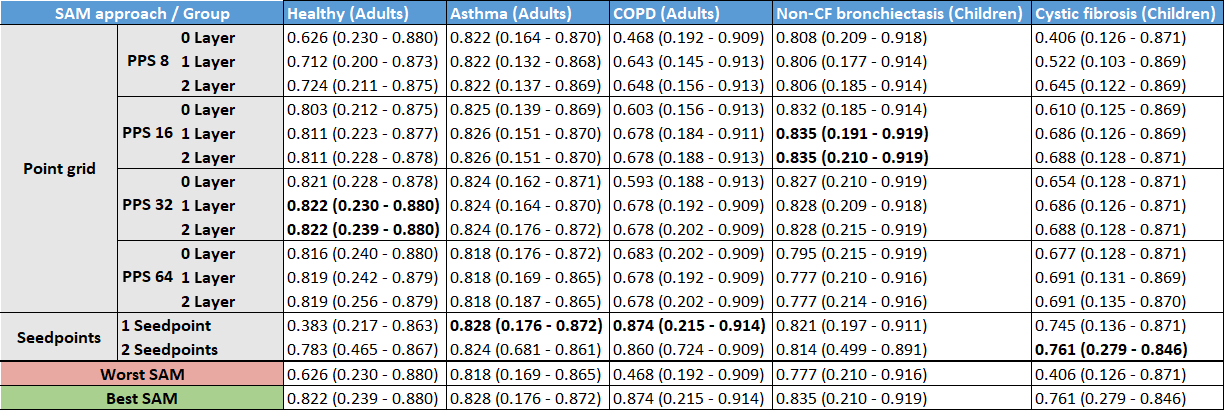
The best performing ZSS was determined by the median DSC per dataset. ANOVA analysis was used to quantify the DSC differences among the 14 ZSS modes. To assess various MRI setups, we divided each dataset into subgroups defined by combinations of devices and sequence parameters. Finally, the DSC of the SAM approach best performing for the whole dataset (identified using Table1) was calculated for each subgroup in Table2.
Results
As summarized in Table1, SAM provides lung segmentation with a median DSC higher 0.8 in 4/5 groups. The highest median DSC was measured for adult COPD patients and the lowest median DSC for children with cystic fibrosis. In 3/5 groups, seedpoint-based prompts improved the DSC.ANOVA analysis stated a significant (p<0.001) difference between examined SAM variants, however, there is no decisive impact of vendor or sequence parameter as documented in Table2 and demonstrated in Figure2.
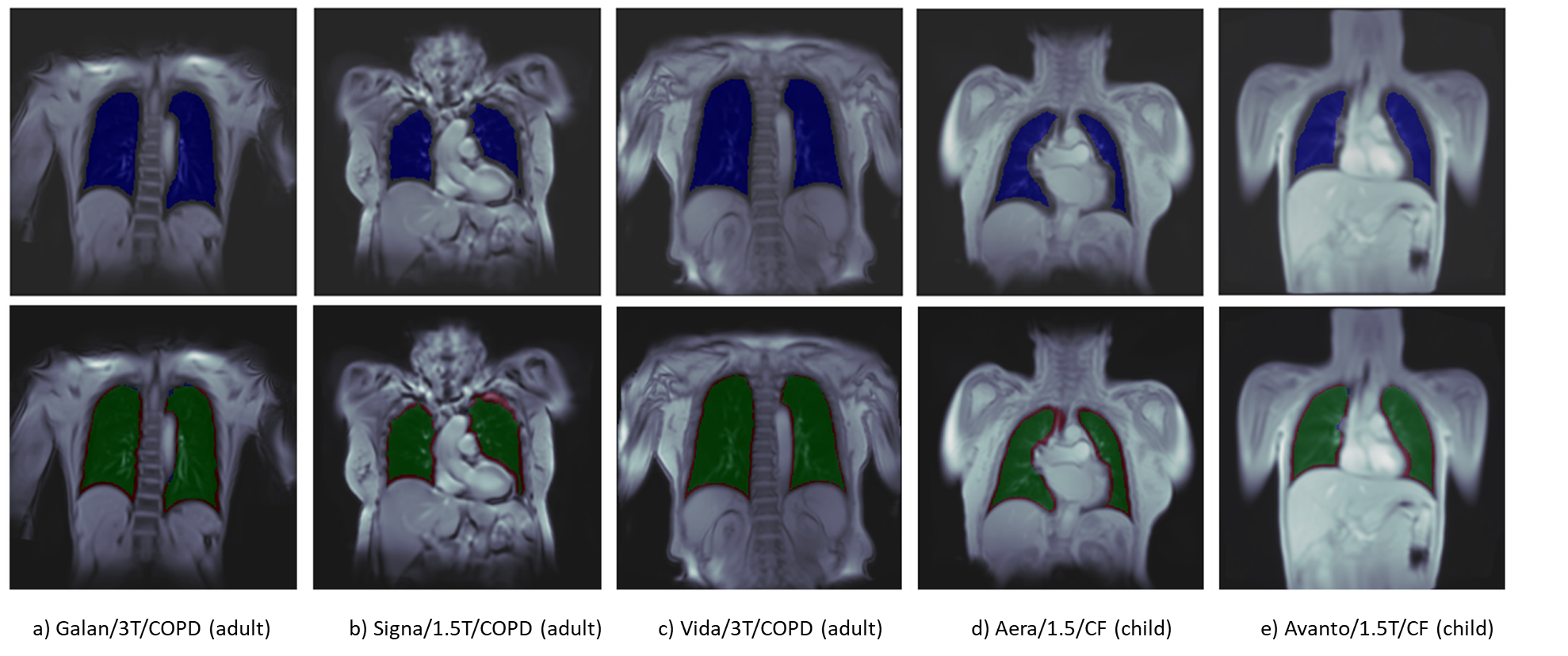
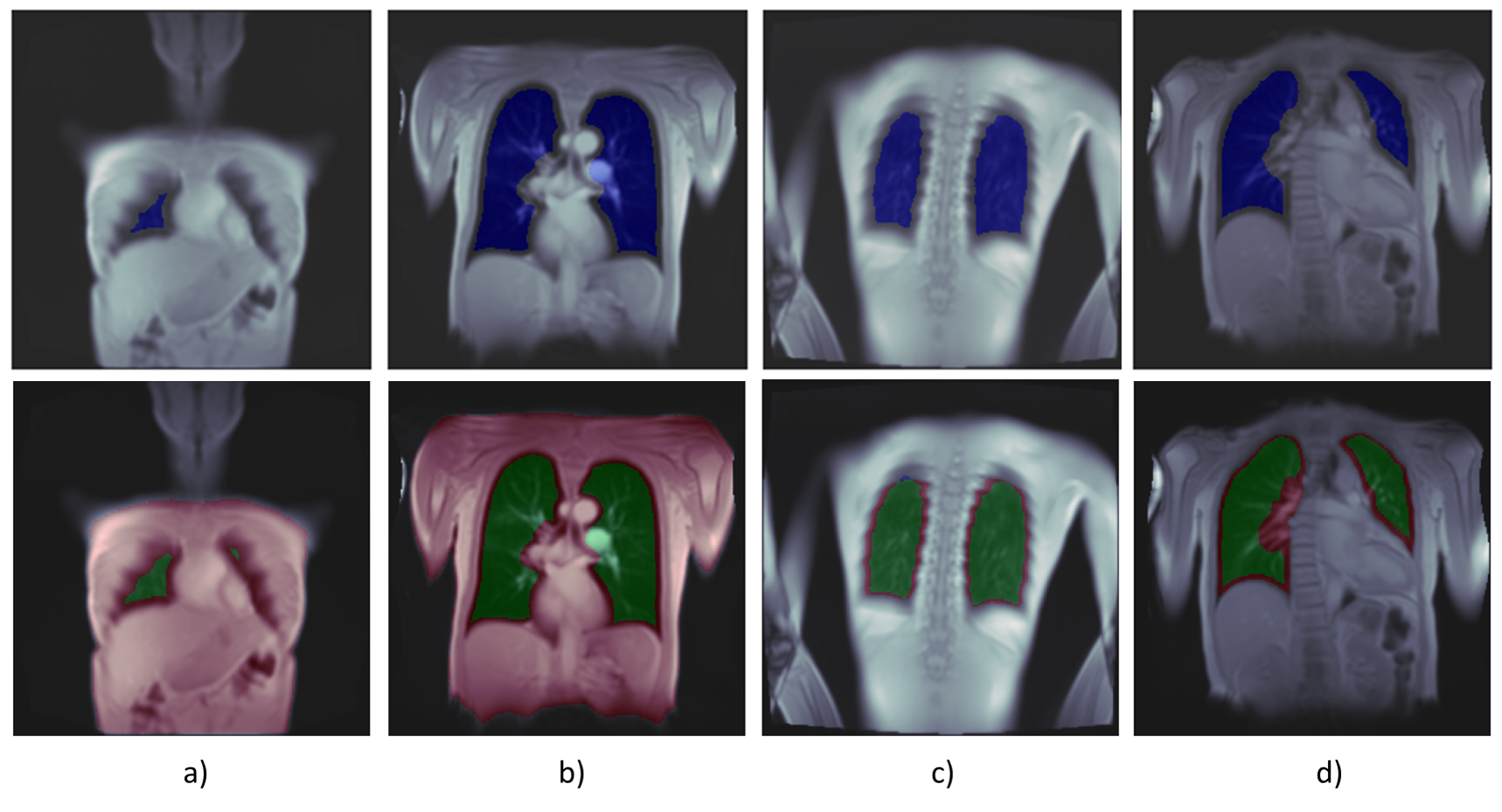
Two kinds of errors could be observed: In some cases, SAM is unable to recognize the lung parenchyma as a separate segment and segments the entire thorax (Figure 3a-b). The second error observed is the insufficient differentiation of the lung from surrounding tissue or vessels (Figure 3c-d).
Discussion
SAM needs no training data to provide a DSC up to 0.87. However, Table1 shows huge differences between SAM configurations for the same data. Furthermore, there is no common best configuration for the examined datasets. This causes an effort to determine the best working approach for a new dataset. A further issue is the recognition of the aimed segment, as SAM may provide not only the segment of interest. Seedpoints can prevent the need for segment recognition but necessitates the definition of suitable coordinates. Nevertheless, it can be assumed that solving these issues is less laborious than manually segmenting sufficient training data.On the other hand, PREFUL requires a specific segmentation that avoids partial volume effects at the lung boundaries. Such specific requirements are hard to recognize by ZSS. Few-shot segmentation could be a solution and should be evaluated in the future.
Conclusion
Zero-Shot lung segmentation in PREFUL MRI from adults and children with pulmonary diseases is feasible.Acknowledgements
No acknowledgement found.References
Voskrebenzev A, Gutberlet M, Klimeš F, Kaireit TF, Schönfeld C, Rotärmel A, Wacker F, Vogel-Claussen J. Feasibility of quantitative regional ventilation and perfusion mapping with phase-resolved functional lung (PREFUL) MRI in healthy volunteers and COPD, CTEPH, and CF patients. Magn Reson Med. 2018 Apr;79(4):2306-2314. doi: 10.1002/mrm.26893. Epub 2017 Aug 30. PMID: 28856715.
Isensee F, Jaeger PF, Kohl SAA, Petersen J, Maier-Hein KH. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nat Methods. 2021 Feb;18(2):203-211. doi: 10.1038/s41592-020-01008-z. Epub 2020 Dec 7. PMID: 33288961
Crisosto C, Voskrebenzev A, Gutberlet M, Klimeš F, Kaireit TF, Pöhler G, Moher T, Behrendt L, Müller R, Zubke M, Wacker F, Vogel-Claussen J. Artificially-generated consolidations and balanced augmentation increase performance of U-net for lung parenchyma segmentation on MR images. PLoS One. 2023 May 9;18(5):e0285378. doi: 10.1371/journal.pone.0285378. PMID: 37159468; PMCID: PMC10168553.
Kirillov A, Mintun E, Ravi N, Mao H, Rolland C, Gustafson L, ... & Girshick R. Segment anything. arXiv preprint. 2023 Apr. arXiv:2304.02643. doi: 10.48550/arXiv.2304.02643.
Voskrebenzev A, Gutberlet M, Kaireit TF, Wacker F, Vogel-Claussen J. Low-pass imaging of dynamic acquisitions (LIDA) with a group-oriented registration (GOREG) for proton MR imaging of lung ventilation. Magn Reson Med. 2017 Oct;78(4):1496-1505. doi: 10.1002/mrm.26526. Epub 2016 Nov 18. PMID: 27859552.
Figures