1992
Automatic AI based Intensity harmonization of MRI prostate images.1Quibim S.L, Valencia, Spain
Synopsis
Keywords: AI/ML Image Reconstruction, Image Reconstruction, Image Harmonization
Motivation: In multi-centric, multi-scanner datasets differences between images caused by different acquisition protocols and reconstruction techniques are found. These differences introduce biases when developing AI-based solutions that limit their generalization.
Goal(s): To develop an algorithm to harmonize intensities on MR medical images independently of the source and artifacts that may be introducing a bias.
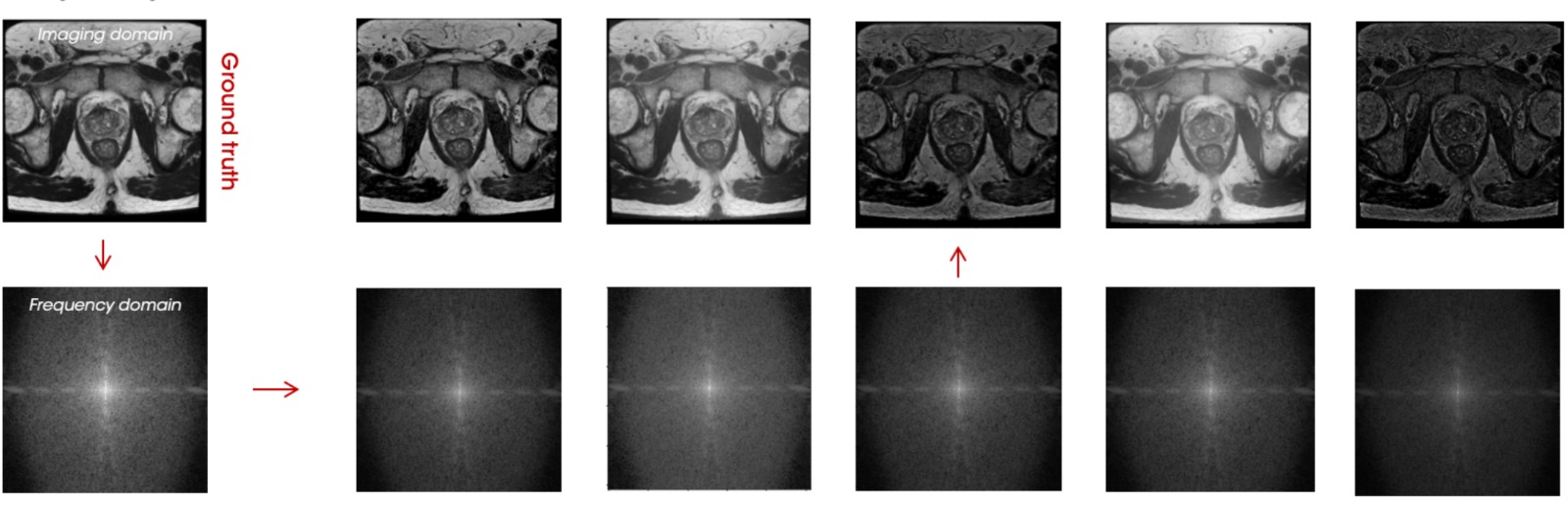
Approach: Use of the MRI frequency domain to synthetically generate realistic intensity variations simulating differences in acquisition protocols. Image-to-image CNN-based solution to reconstruct any image to a reference dataset.
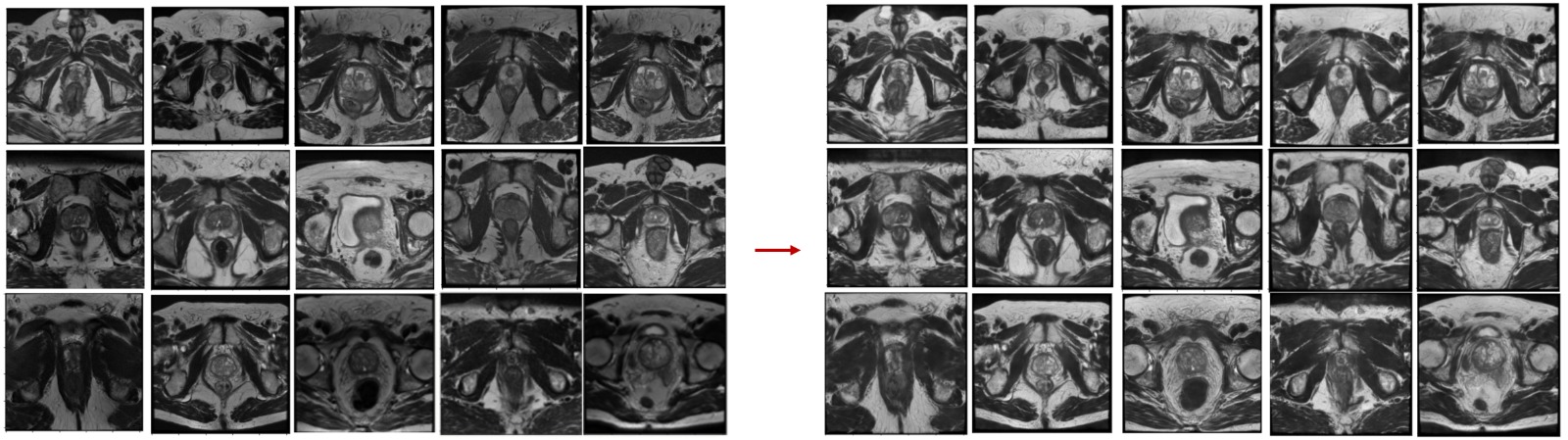
Results: Harmonization of prostate T2w MRI showed a qualitative harmonization of the images and an improvement in AI-based segmentation task.
Impact: This methodology helps the harmonization of medical MRI images, enhancing accuracy and efficiency in MRI AI based task. By standardizing image quality and reducing variations, this innovation ensures consistent interpretations across healthcare institutions, improving collaboration among medical and AI professionals.
Introduction
It has been shown that even when care is taken to standardize acquisitions, any changes in hardware, software, or protocol design can lead to differences in quantitative results. This deeply impacts the use and utility of MRI in multi-site or long-term studies when working with AI or digital driven analysis methods, where consistency is often valued over image quality. We propose a method of intensity harmonization, which uses the frequency domain to generate realistic contrast alterations of already quality and homogenous samples to later use the resultant paired slices to train a deep learning architecture to produce images with consistent contrast.Materials and methods
The algorithm was trained with 10 original and high-quality prostate T2w MRI studies, from which 50,000 paired contrast altered-original samples were generated. 35,000 images were used for training while the remaining 15,000 samples were used for validation.The process of generating these alterations was broken down into steps. First, the image was transformed into the frequency domain, allowing us to obtain both the phase and module information. Next, a mask was generated to guide the alterations. This mask consisted of two components. The first component was the proper module of the image, which was normalized to a range of 0 to 1. The second component was a round mask with a radius of 2-6% of the original image size, positioned at the center of the frequency domain where the low frequencies are, corresponding with more “subtle” features such as contrast. Values of 0 and 1.5 [a1] were assigned to this area to simulate different contrasts. Finally, to create the final mask, the two masks generated in the previous step were added and normalized together. The result was a realistic non-linear increase or decrease in contrast.With the mask in place, several operations, primarily additions and subtractions, were applied randomly to the module by a factor determined by this final mask previously obtained.Architecture. (figure 1)
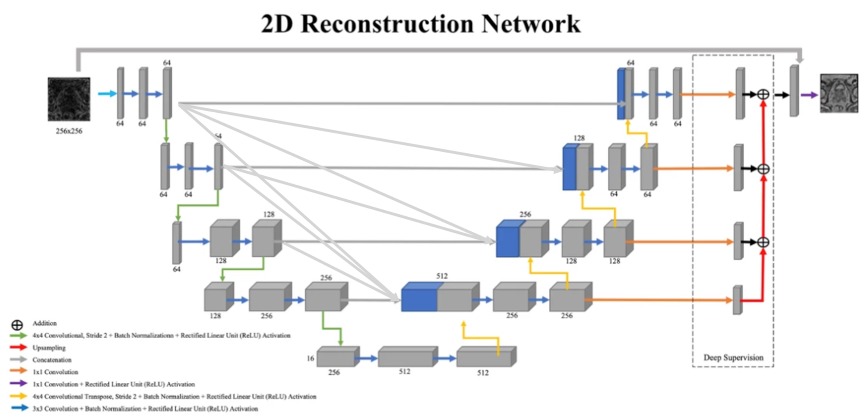
A variation of the UNet architecture, known as UNet3+, was used. This architecture has the particularity of a total connection between all the encoder blocks with all the decoder blocks, to which a deep supervision block was added at the end of each of the decoder blocks and another extra connection between the input, prior to the first convolutional layer, and the last concatenation layer after deep supervision.
The added connections that bring the UNet3+ architecture helps the decoder to reconstruct a more realistic synthetic image, the extra information flowing from encoder to decoder blocks is key in the transference of contrast, allowing to retain information that may be useful before each encoder’s down sampling block.The extra skip connection at the beginning boosts shape recognition by reconstructing itself as many inputs are very similar to the original and paired output.
Validation.
To validate the proposed methodology, we evaluated the performance of two prostate automatic segmentation algorithms, on trained with original images and a second one trained with the harmonized ones. A UNet-based architecture was trained, in both cases with 200 T2w MR studies, using 80% for training and the remaining 20% to test. The training was repeated several times with different data on train-test split.To further validate the harmonization method, a subset of 50 T2w MR studies with endorectal coil were segmented with the previous segmentation methods before and after harmonization.Segmentation performance was analyzed through the Dice Score Coefficient (DSC).
Results
The automatic prostate segmentation showed a DSC of 0.86 in the model trained with the original images, while it increased to 0.91 with the harmonized synthetic images. (figure 4)
Finally, when segmenting the MR studies with endorectal coil, a mean DSC of 0.31 was obtained while it increased to 0.66 after harmonization. (figure 2)
Discussion and Conclusion
Discussion. Harmonization is crucial step to minimize differences when quantitative information is extracted from MRI or AI solutions are delivered. We propose a novel methodology for prostate MRI harmonization. This method has shown an improvement in automatic prostate segmentation, especially in cases with significant differences in terms of image intensity and contrast. Additionally, this methodology has shown promising results that are worth to be applied to other organs and MR sequences.Conclusion. The use of the frequency domain for synthetic image generation in MR studies has shown promising results in image harmonization. In multi-centric studies this method can be applied to minimize the differences across scanners facilitating the development of generalizable and robust AI models to be used in different clinical environments.
Acknowledgements
No acknowledgement found.References
No reference found.Figures
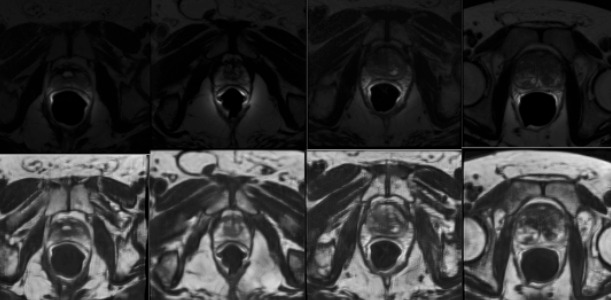
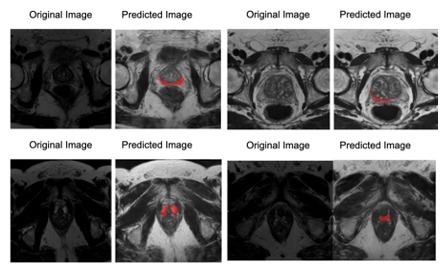
Segmentation on prostate T2 peripheral region for outliers cases before (no segmentation at all) and after harmonization.