1989
Fast CUBE imaging of pediatric pituitary with deep learning reconstruction algorithm at 3T1Radiology Department, The First Affiliated Hospital ,Zhejiang University School of Medicine, Hangzhou, China, 2MR Research, GE Healthcare, Beijing, China
Synopsis
Keywords: AI/ML Image Reconstruction, Normal development, Pituitary
Motivation: 3D CUBE imaging of pediatric pituitary is time-consuming, and thus presents difficulties for children with limited patience and cooperation. A vendor-provided deep learning reconstruction (DLR) algorithm, proposed for high image SNR, may allow for MR imaging with shortened scan time.
Goal(s): Explore if DLR allowed for rapid CUBE imaging in pediatric pituitary while maintaining the image quality and precise measurement of pituitary height.
Approach: The imaging quality, scan time, and pituitary height measured were compared between DLR-CUBE and conventional CUBE.
Results: Relative to conventional CUBE, DLR-CUBE showed improved SNR, comparable image quality, accurate measurement of pituitary height, and only half the scan time.
Impact: DLR-CUBE can dramatically shorten the acquisition time while maintaining the image quality and accurate measurement for pituitary height, demonstrating the potential of DLR-CUBE in clinical examinations of pediatric pituitary.
Introduction
Accurate measurement of pituitary in size and shape is of importance in the assessment of children's growth and development 1. The height of pituitary is often used to evaluate the normality of growth hormone in adolescents. 2 A vendor-provided fast-spin-echo (FSE) based CUBE 3 imaging has been routinely applied for pediatric pituitary examinations in clinic. While three-dimensional high resolution imaging can be obtained, CUBE imaging usually requires relatively long acquisition time, posing challenges especially for children with limited ability in motion control during MRI examination. The resultant motion artifacts usually affect the image quality and further the accurate diagnosis in clinic. Recently, a vendor provided deep learning (DL) reconstruction algorithm 4 (DLR, AIRTM Recon DL, GE Healthcare) has been proposed for MR imaging application, allowing for fast image acquisition without compromising on image quality 5,6. Thus, in this study, we aimed to evaluate the impact of DLR on CUBE imaging of pediatric pituitary in aspects of acquisition time, image quality, and the quantitative measurements of pituitary height, by comparing with conventional CUBE imaging.Methods
Imaging:14 children (short stature; 10 girls, 4 boys; mean age of 9 years; range 6~14 years) were enrolled in this study with each signed written informed consent. All MRI images were acquired on a 3T scanner (SIGNA Architect, GE Healthcare) with a 24-channel brain coil. A conventional sagittal T1WI CUBE with NEX of 2 (Con-CUBE-NEX2) was acquired with the following parameters: TR=47ms; TE=13ms; FOV=16×16 mm2; matrix=288×256; voxel size=0.6×0.6mm2; slice thickness=2mm; acceleration factor=2. A separate sagittal T1WI CUBE was also performed with the same parameters as for Con-CUBE-NEX2, except with NEX=1. The resultant raw data were separately reconstructed with DLR (DL-CUBE-NEX1) and conventionally (Con-CUBE-NEX1).Data processing: One senior radiologist was employed to evaluate the image quality, and calculate the SNR of pituitary gland, and CNR between pituitary gland and normal brain tissue. The qualitative image scores, including edge sharpness, artifacts, structure conspicuity, and overall image quality, were also assessed based on a 5-point Likert scale7. In addition, the height of pituitary gland was measured and the image acquisition time was recorded.
Statistical analysis: All statistical analyses were performed using SPSS (IBM, v27). One-way ANOVA was used to compare the scores rated for image quality, SNR, and CNR among the three datasets. The Bonferroni post hoc test was used to adjust for all significant pairwise comparisons. Paired t-test was separately used to compare the measured pituitary height and image acquisition time between the DL-CUBE-NEX1 and Con-CUBE-NEX2. P < 0.05 was considered statistically significant.
Results
As shown in Fig. 1 and Table 1, the SNR of DL-CUBE-NEX1 (66.92±5.75) was significantly higher than that of Con-CUBE-NEX2 (56.34±4.72) and Con-CUBE-NEX1 (43.36±3.14) (P<0.05). Without DL, the CNR of Con-CUBE-NEX1 was only 3.93±0.60, significantly decreased compared with that of DL-CUBE-NEX1 (7.67±1.42, P<0.05). The CNR of DL-CUBE-NEX1 (7.67±1.42) was higher than that of Con-CUBE-NEX2 (7.12±0.90), although the difference was not significant. There was no significant difference between Con-CUBE-NEX2 and DL-CUBE-NEX1 in all indicators for qualitative evaluation (edge sharpness, artifacts, Structure conspicuity and overall image quality). In comparison, the quality scores of Con-CUBE-NEX1 without DL were significantly lower than those of Con-CUBE-NEX2 (P<0.05) (Table 2 and Fig. 2). In addition, the height measured on DL-CUBE-NEX1 (6.47±0.58mm) was consistent with the height measured on Con-CUBE-NEX2 (6.49±0.55mm, P=0.83), and the scan time of DL CUBE was nearly twice as short as that of Con-CUBE-NEX2 (1min09s vs. 2min13s, P < 0.01) (Table 3).Discussion
In our study, even if comparing with conventional CUBE imaging with NEX of 2, fast DL-CUBE imaging with 1 NEX offered excellent image quality, higher SNR and CNR, and clear depiction of pituitary structure, but only required half the scan time. These findings indicate great potential in clinical applications for pediatric examination. However, the conventional CUBE imaging with NEX of 1 was found with severely degraded image quality if compared with the conventional CUBE imaging with twice the NEX. Moreover, comparable measurement for pituitary height was shown between DL-CUBE-NEX1 and Con-CUBE-NEX2, further validating the image quality of DL-CUBE-NEX1. We however, will proceed with data collection to conduct a more extensive large-sample validation for DL CUBE in pediatric pituitary examinations.Conclusion
DL CUBE has been demonstrated to shorten the acquisition time without sacrificing image quality for pediatric pituitary, and might thus be considered a surrogate to conventional CUBE imaging with long scan time in routine clinical pediatric pituitary examination.Acknowledgements
No acknowledgement found.References
1. Yadav, P., Singhal, S., Chauhan, S., et al. MRI evaluation of size and shape of normal pituitary gland: age and sex related changes. J Clin Diagn Res. 2017; 11(12): 1-4.2. Nagel, B. H. P., Palmbach, M., Petersen, D., et al. Magnetic resonance images of 91 children with different causes of short stature: pituitary size reflects growth hormone secretion. European journal of pediatrics, 1991, 156, 758-763.
3. Lien, R. J., Corcuera-Solano, I., Pawha, P. S., et al. Three-tesla imaging of the pituitary and parasellar region: T1-weighted 3-dimensional fast spin echo cube outperforms conventional 2-dimensional magnetic resonance imaging. Journal of Computer Assisted Tomography. 2015; 39(3): 329-333.
4. Lebel RM. Performance characterization of a novel deep learning-based MR image reconstruction pipeline. arxiv.org/abs/2008.06559.
5. Shanbhogue, K., Tong, A., Smereka, P., et al. Accelerated single-shot T2-weighted fat-suppressed (FS) MRI of the liver with deep learning–based image reconstruction: qualitative and quantitative comparison of image quality with conventional T2-weighted FS sequence. European radiology. 2021; 31(11): 8447-8457.
6. Park, J. C., Park, K. J., Park, et al. Fast T2‐Weighted Imaging with Deep Learning‐Based Reconstruction: Evaluation of Image Quality and Diagnostic Performance in Patients Undergoing Radical Prostatectomy. Journal of Magnetic Resonance Imaging. 2022; 55(6): 1735-1744.Figures
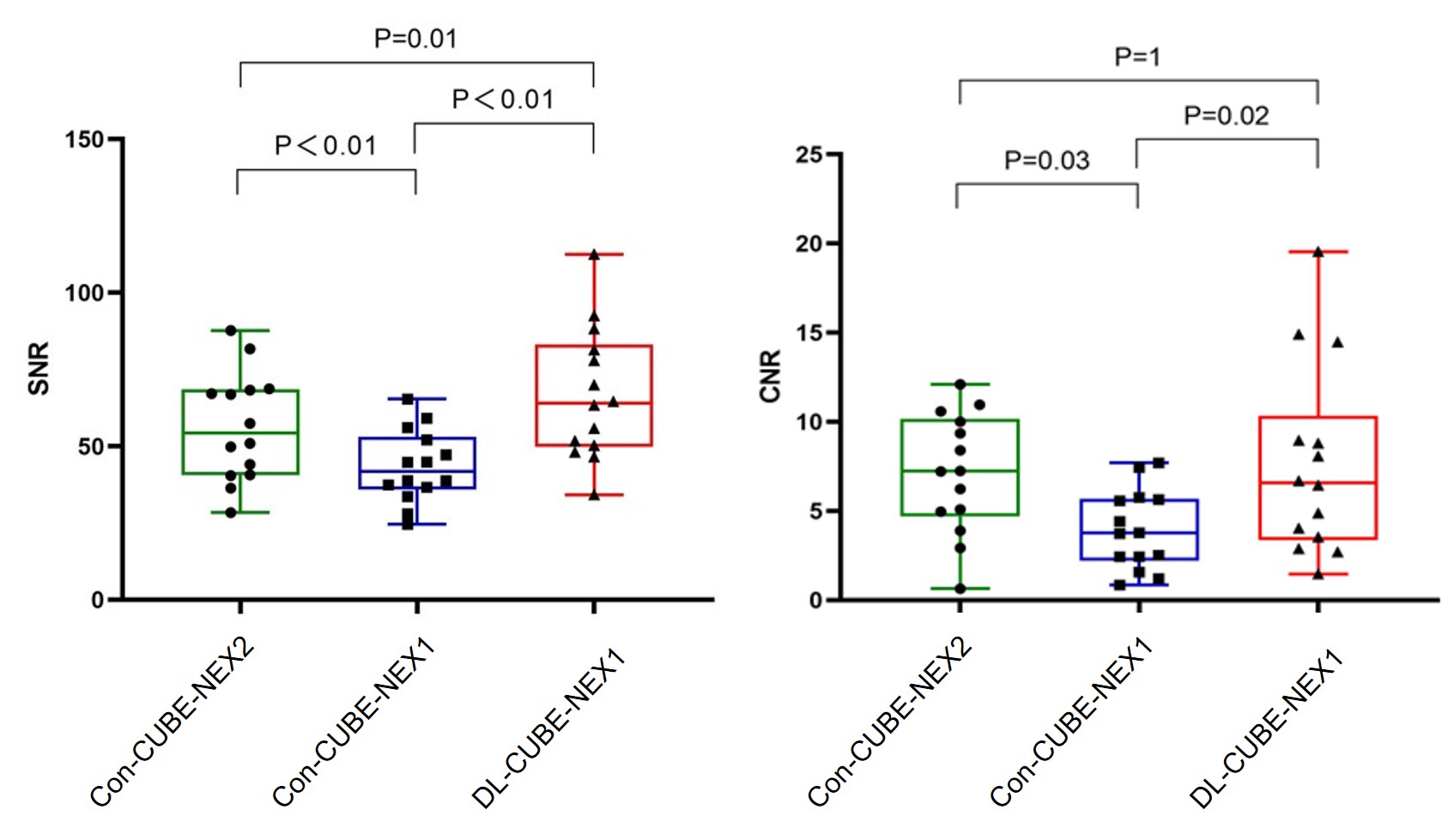
Figure 1. Box plots of SNR and CNR for conventional CUBE with NEX =2 (Con-CUBE-NEX2), conventional CUBE with NEX = 1 (Con-CUBE-NEX1), and CUBE combined deep learning reconstruction with NEX = 1 (DL-CUBE-NEX1).
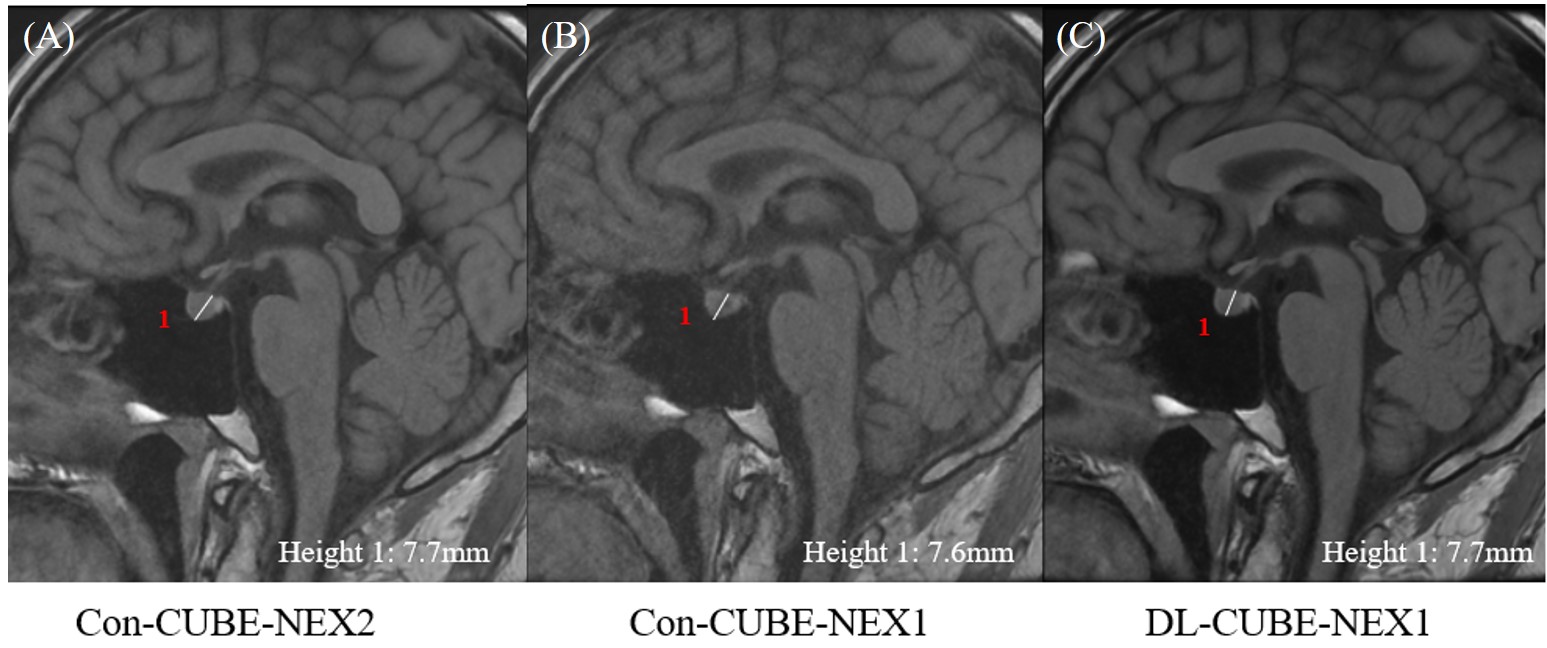
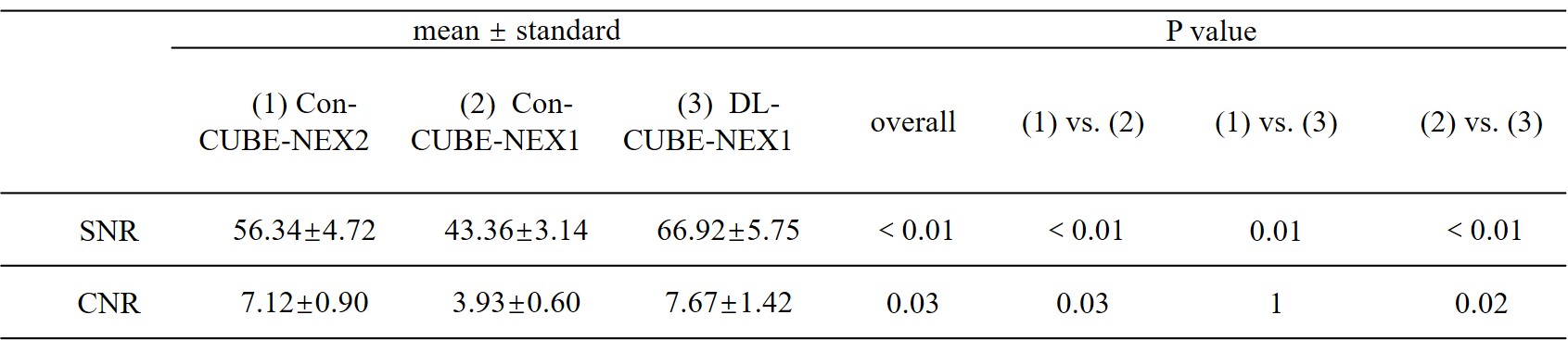
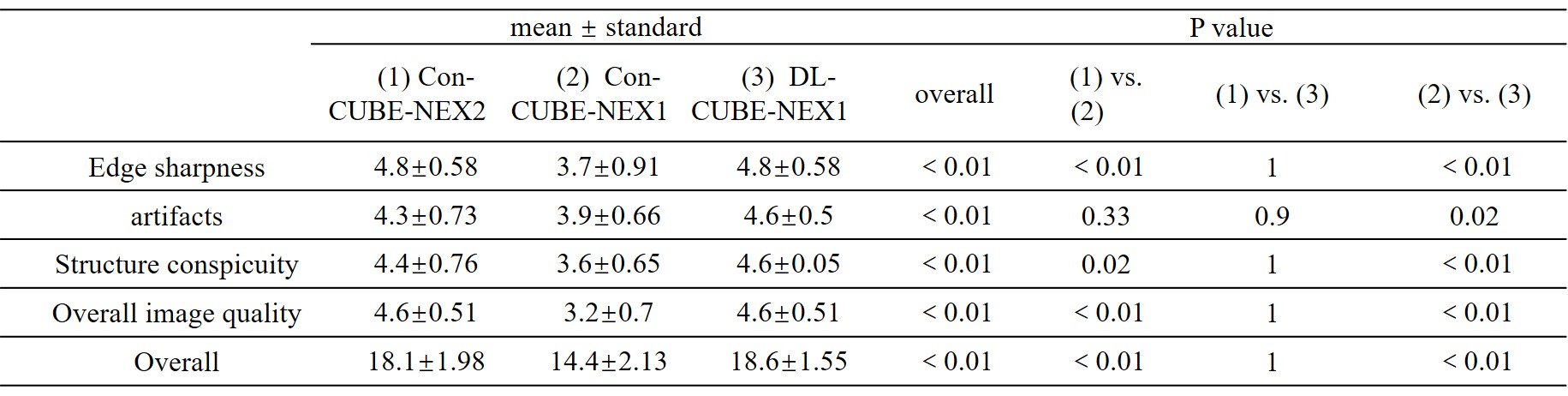
Table 2. Qualitative image quality scores of the three groups. Con-CUBE-NEX2, conventional CUBE with NEX =2; Con-CUBE-NEX1, conventional CUBE with NEX = 1; DL-CUBE-NEX1, CUBE combined deep learning reconstruction with NEX = 1. Data are mean ± standard deviations.
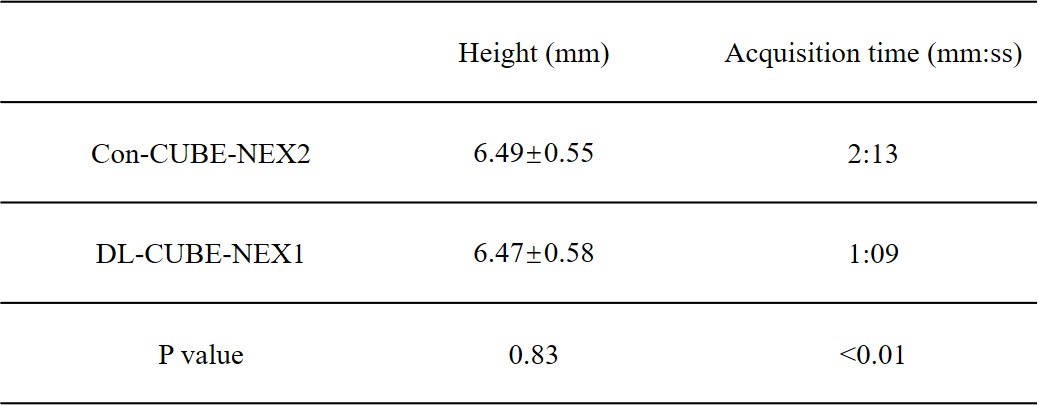
Table 3. Comparison of acquisition time and pituitary height measured by the fast CUBE with deep learning reconstruction (DL-CUBE-NEX1) and the conventional CUBE (Con-CUBE-NEX2).