1979
Angiogram-aware deep learning methods for artifact correction of contrast enhanced MR angiography1Korea Advanced Institute of Science and Technology, Daejeon, Korea, Republic of, 2Samsung medical center, Sungkyunkwan university college of medicine, Seoul, Korea, Republic of
Synopsis
Keywords: Analysis/Processing, Machine Learning/Artificial Intelligence, Angiography
Motivation: CE MRA data is susceptible to motion and noise artifact due to its longer acquisition time. Conventional intensity-based registration are often unreliable, necessitating better artifact correction methods.
Goal(s): To provide better artifact correction methods for CE MRA using generative deep learning and angiogram-aware loss function
Approach: two deep learning architectures were trained with/without angiogram-aware loss function. Network accuracy was evaluated based on CE MRA dynamic scans and angiogram.
Results: motion correction was successfully performed, resulting in angiograms with PSNR=37.9±4.3 and SSIM=0.97±0.04. angiogram-aware loss function improved the correction accuracy by up to 13 points in PSNR and 17 points in SSIM.
Impact: We developed accurate deep learning solutions for CE MRA artifact correction, potentially reducing the need for repeated MRA scans. We also showed that angiogram-aware loss function, which considers the last processing steps of CE MRA data, can improve correction accuracy.
Introduction
Contrast enhanced MR angiography (CE MRA) scans require longer acquisition time to fully reflect contrast agent bolus arrival and peak at the area of interest1. Due to this, many artifacts including motion and noise may affect the acquired CE MRA data. Conventional motion correction methods such as pairwise intensity-based registration often exhibit errors due to signal intensity changes caused by contrast agent arrival and motion itself2. Deep learning methods have shown good generative ability in the recent years3. However, precise correction of the CE MRA scans may not necessarily guarantee a high quality angiogram. In this study, we propose deep learning methods to correct motion and improve SNR on CE MRA data. Additionally we propose an angiogram-aware training approach to assure the accuracy of the resulting angiogram.Method
CE MRA data from 60 patients, split to 50:10 for training and test, with varying degree of ischemia were used in this study. The CE MRA data for carotid arteries were acquired using a head/neck coil with a 3D TWIST sequence and the following parameters: TR/TE = 2.62/0.95 msec, matrix = 320 x 240 x 144, field of view = 300 x 400 x 172.8 mm3, scan direction = coronal, and number of dynamic scans = 28. The brain area was isolated by cropping the CE MRA data to the size of 140 x 150 x 144 and changing the view to axial. Only the cropped CE MRA data were used throughout this study.Motion and noise corruptions were synthetically introduced to the CE MRA data. Two types of motion artifacts were introduced: translational and rotational. The translational motions were added by adding linear phase into central phase encoding lines (more often) or periphery (less often) to reflect the nature of TWIST-type keyhole acquisition. The rotational artifacts were introduced by rotating the CE MRA data at random time points at rotation angles between -5 to 5 degrees. The noise corruptions were added in random time points and the added Gaussian noise ranges from 0 to 10% of peak CE MRA signal.
The deep learning architectures used to perform correction were U-Net and U-Net + generative adversarial network (GAN). For both architectures, the input and output were modified to 28 channels reflecting the number of dynamic scans. Both architectures were trained twice, with and without the angiogram-aware loss function. The angiogram-aware loss function is specified as the difference between the maximum intensity projections (MIP) of the temporally subtracted CE MRA scans and the MIP of the temporally subtracted network output. The loss functions used in all training schemes were L1loss + optional angiogram-aware loss for U-Net and L1loss + optional angiogram-aware loss + binary cross entropy (BCE) loss for U-Net + GAN. Other training parameters were: batch size = 8, training epochs = 500, learning rate = 1e-4, and ADAM optimizer.
The correction accuracy was evaluated using peak signal to noise ratio (PSNR) and structural similarity (SSIM) of the CE MRA dynamic scans and the resulting final angiogram.
Results
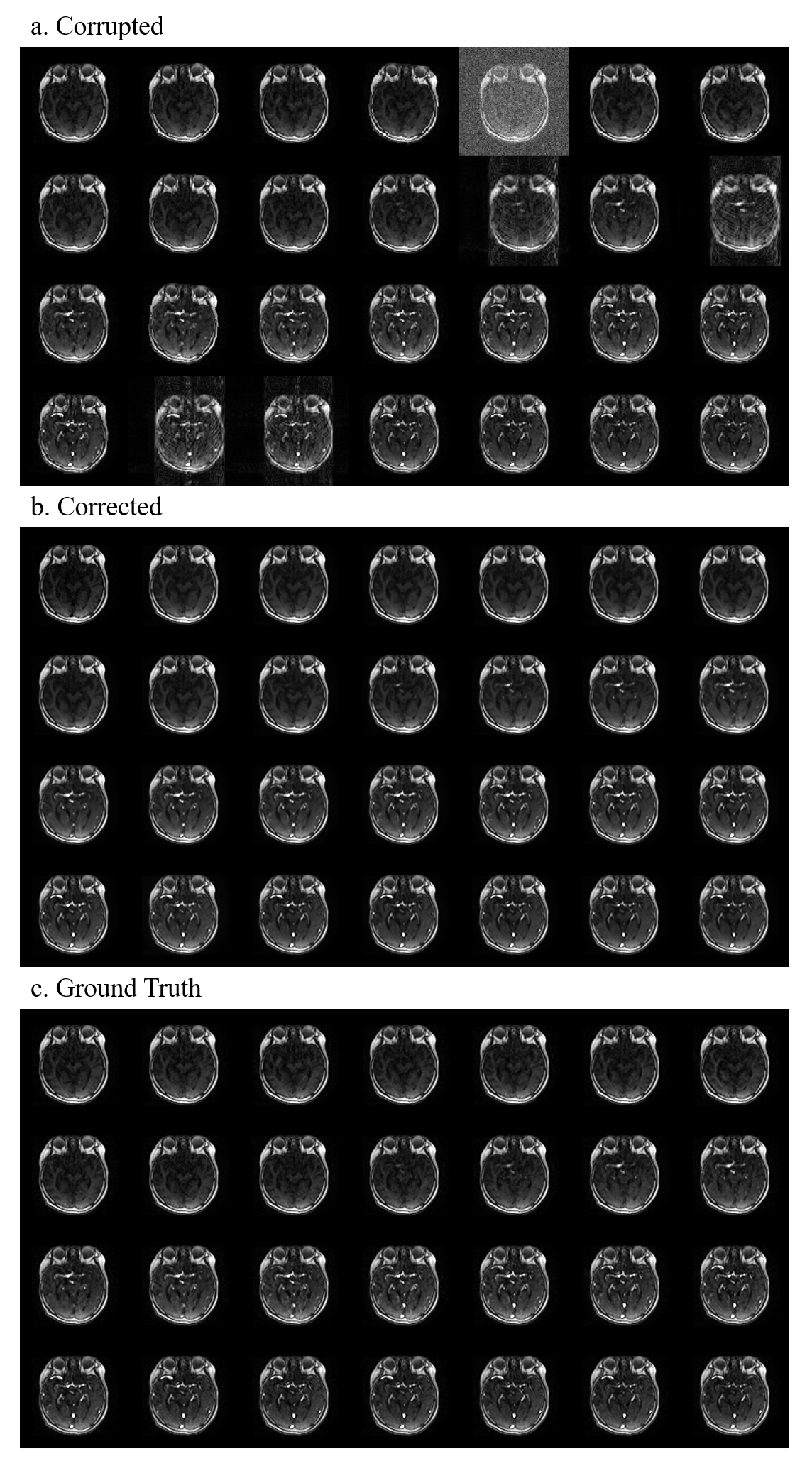
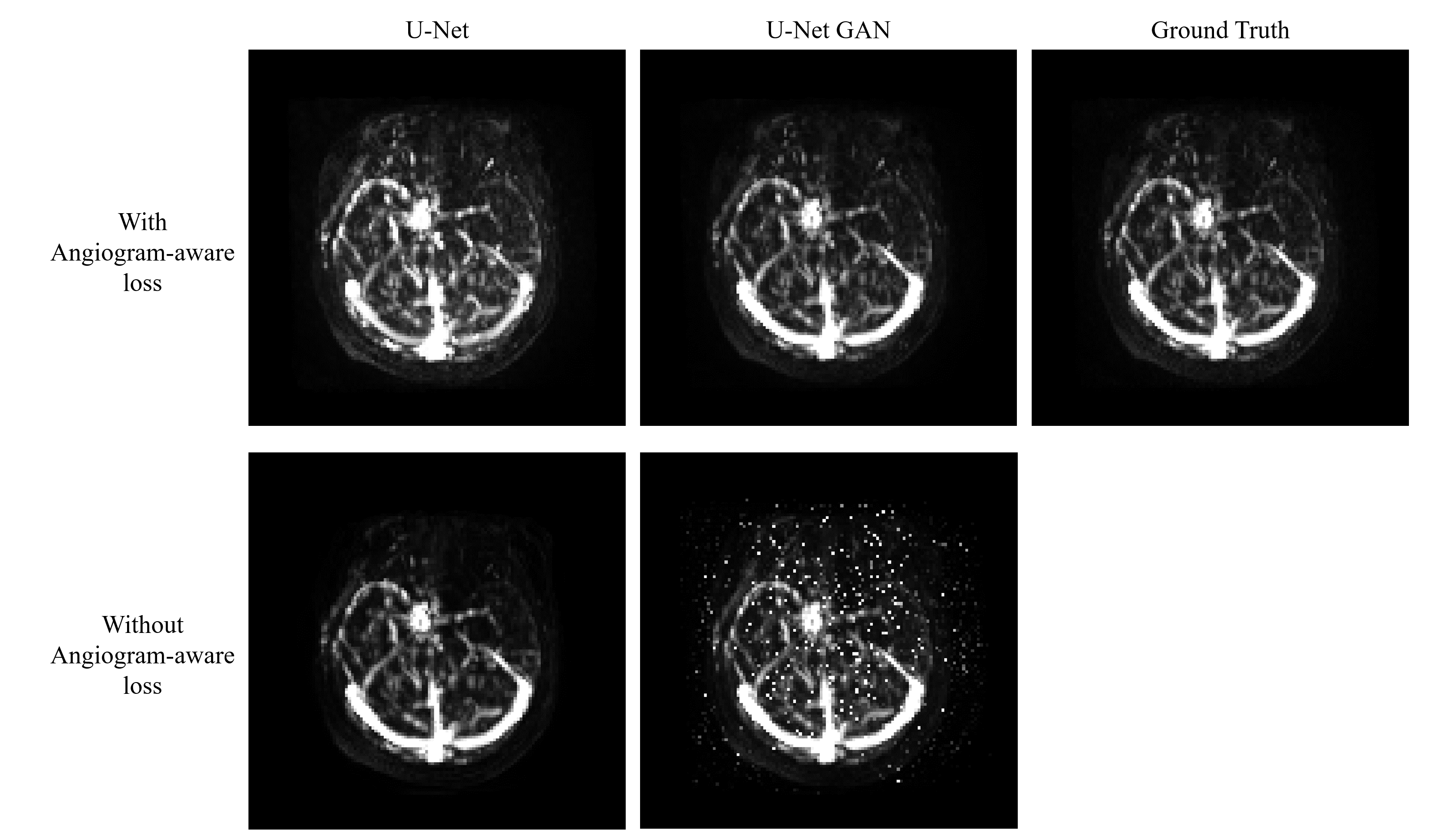
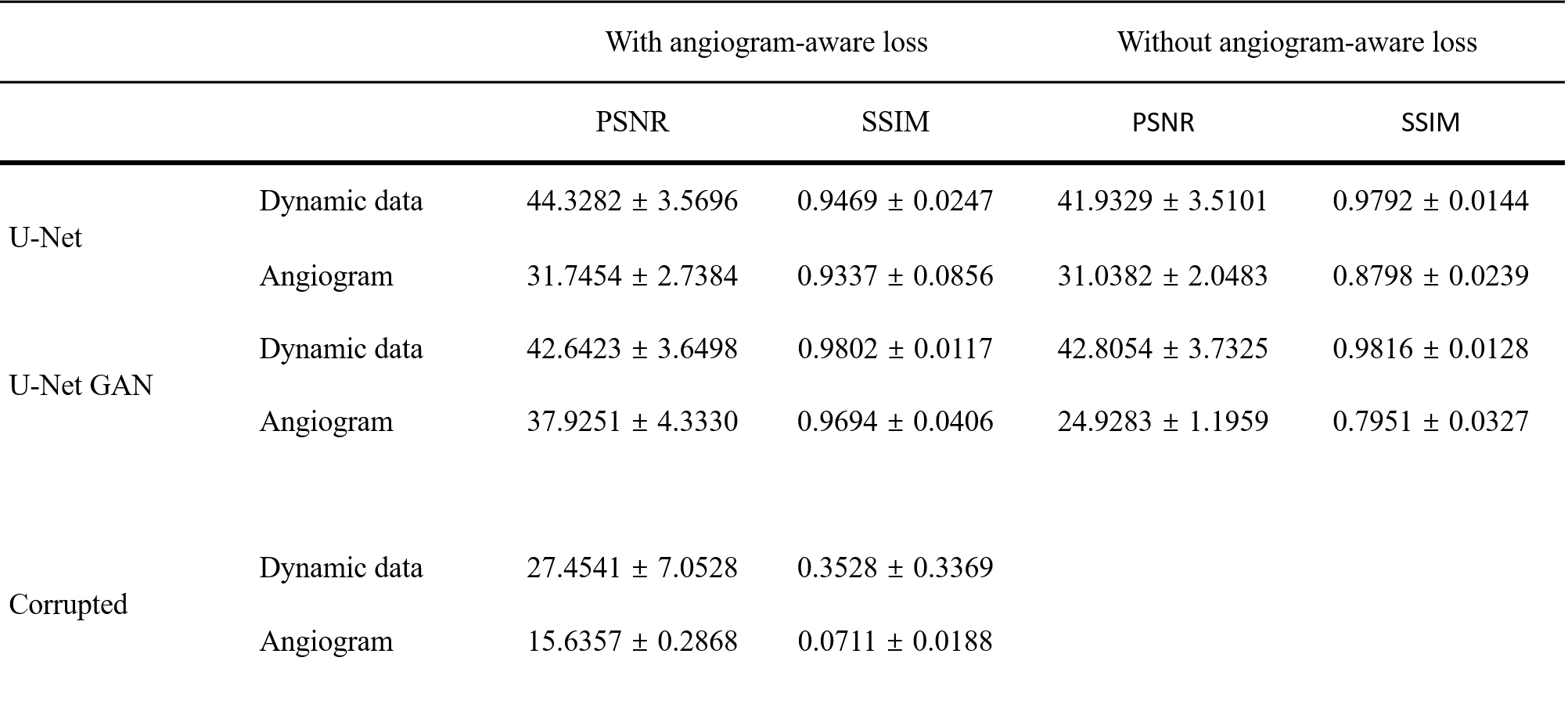
Sample CE MRA dynamic scans before and after deep learning based artifact correction showed successful correction of the dynamic scans and close similarity to the ground truth (Figure 1). The deep learning results also showed matching bolus arrival and bolus peak time, which may hold clinical relevance. Furthermore, deep learning networks trained with angiogram-aware loss showed better similarity in terms of the angiogram than those without angiogram-aware loss (Figure 2). This was consistent with quantitative analysis, showing the networks using angiogram-aware losses yielded improvement in angiogram for both U-Net and U-Net + GAN methods (Table 1). The angiogram-aware loss improved dynamic scans PSNR by up to 7% and angiogram SSIM by up to 17% when used in training.Discussion
The proposed deep learning methods have successfully corrected synthetic artifact corruptions in CE MRA data and produced accurate angiogram when trained with an additional angiogram-aware loss. The improvement in angiogram accuracy highlights the need to consider the final processing steps when performing artifact correction in a dynamic data. The corruption cases used in this study can be extended to reflect MRA-specific artifacts such as pseudo-stenosis, venous contamination, or ringing artifacts. Correction methods for all of these cases may reduce the need for repeated scans in CE MRA studies.Conclusion
In this work, we proposed deep learning methods to perform motion and noise correction in CE MRA data. Additionally, we proposed angiogram-aware loss that improves the accuracy of the corrected angiogram even further. We believe this approach can serve as a solution for correction of corrupted CE MRA data.Acknowledgements
No acknowledgement found.References
1. Riederer SJ, Haider CR, Borisch EA, Weavers PT, Young PM. Recent advances in 3D time-resolved contrast-enhanced MR angiography. J Magn Reson Imaging. 2015;42(1):3-22.
2. Jansen MJ, Kuijf HJ, Veldhuis WB, Wessels FJ, Van Leeuwen MS, Pluim JP. Evaluation of motion correction for clinical dynamic contrast enhanced MRI of the liver. Physics in Medicine & Biology. 2017 Sep 12;62(19):7556.
3. Yu B, Wang Y, Wang L, Shen D, Zhou L. Medical image synthesis via deep learning. Deep Learning in Medical Image Analysis: Challenges and Applications. 2020:23-44.
Figures