1977
Enhancing Ultra-Low-Dose PET/MRI Using Deep Learning Method for Improved Interpretation1Department of Radiology, Harvard Medical School, Boston Children's Hospital, Boston, MA, United States, 2Institute of Neuroscience and Medicine (INM-2), Forschungszentrum Jülich, Jülich, Germany, 3Department of Circulation and Medical Imaging, Norwegian University of Science and Technology, Trondheim, Norway, 4Department of Nuclear Medicine, Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany, 5German Center for Neurodegenerative Diseases (DZNE), Bonn-Cologne, Germany, 6Institute of Aerospace Medicine, German Aerospace Center, Cologne, Germany, 7Institute for Occupational, Social and Environmental Medicine, RWTH Aachen University Hospital, Aachen, Germany, 8Institute of Zoology (Bio-II), Department of Neurophysiology,, RWTH Aachen University, Aachen, Germany, 9Institute of Pharmacology and Toxicology, University of Zurich, Zurich, Switzerland, 10Institute of Neuroscience and Medicine (INM-5), Forschungszentrum Jülich, Jülich, Germany, 11Department of Nuclear Chemistry, Faculty of Mathematics and Natural Sciences, University of Cologne, Cologne, Germany, 12Institute of Radiochemistry and Experimental Molecular Imaging, Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany, 13Division of Sleep Medicine, Harvard Medical School, Boston, MA, United States, 14Faculty of Medicine, Rheinische Friedrich-Wilhelms-Universität Bonn, Bonn-Cologne, Germany, 15Department of Neurology, Medical Faculty, Heinrich-Heine University Düsseldorf, Düsseldorf, Germany, 16Division of Medical Psychology, Rheinische Friedrich-Wilhelms-Universität Bonn, Bonn-Cologne, Germany
Synopsis
Keywords: Analysis/Processing, PET/MR, Low Dose PET/MR
Motivation: We developed a deep learning model to enhance the image quality of ultra-low dose brain PET.
Goal(s): Significantly reducing the injected dose not only minimizes radiation risk in subjects but also provides options for scanning protocols, and more follow-up studies.
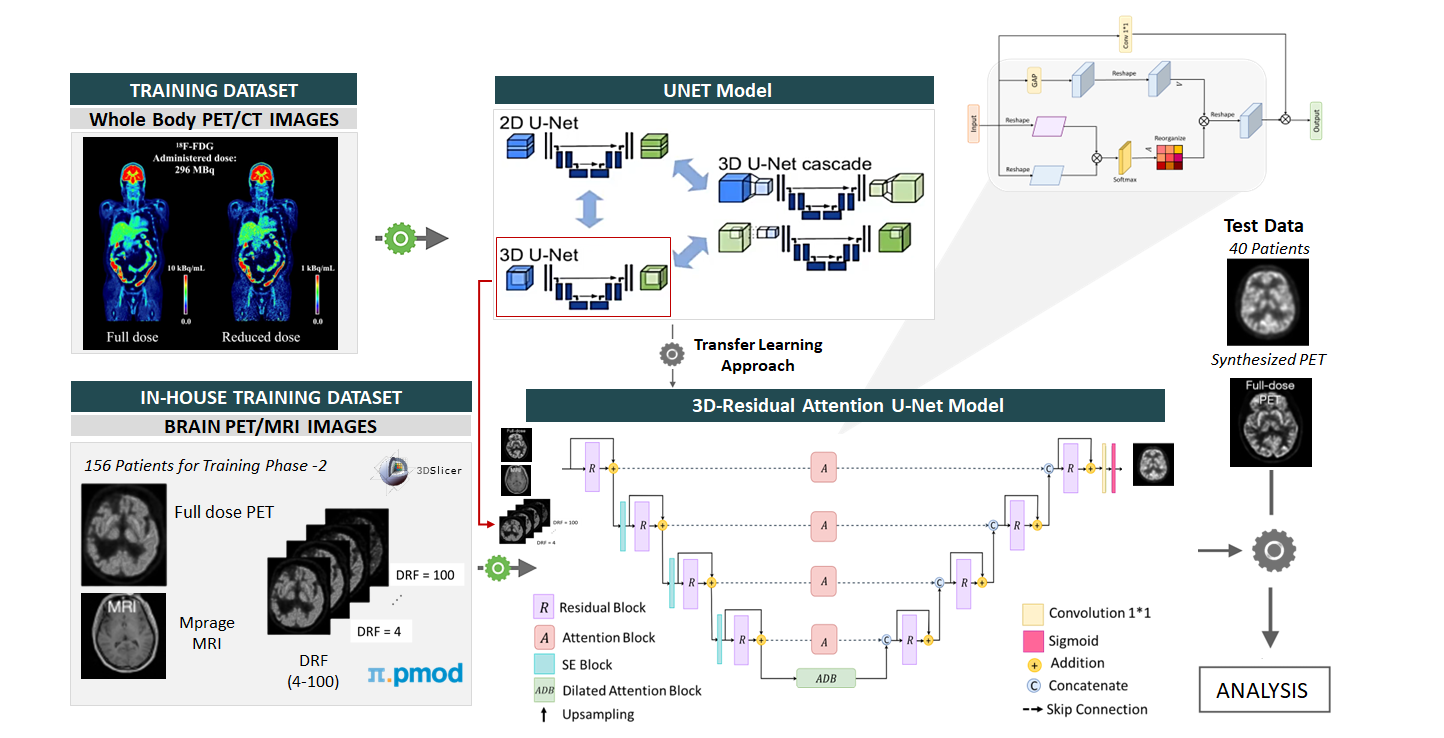
Approach: We proposed a 3D-Residual Attention U-Net model initially trained on whole-body [18F]FDG PET/MR images. We used transfer learning approach to fine-tune our proposed model on [18F]CPFPX PET/MRI inhouse dataset.
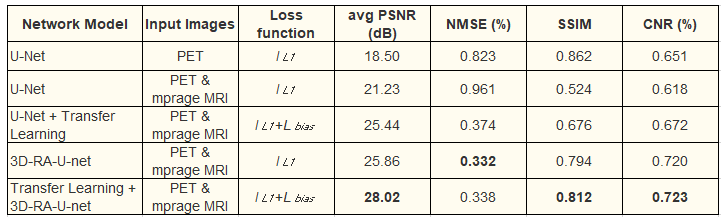
Results: We achieved improved metrics compared to U-Net model with average PSNR of 28.02 (U-Net: 21.23), SSIM of 0.81 (U-Net: 0.53), CNR of 0.72 (U-Net: 0.61) and NMSE of 0.33 (U-Net: 0.67).
Impact: Our model has potential to generate high-quality PET images from low-dose PET/MR, potentially contribute to implementation of kinetic modelling using PET/MR imaging. Our model is capable of enhancing both whole-body and brain datasets, making it valuable asset for diverse applications.
Introduction
Widespread clinical use and large-scale longitudinal imaging studies face limitations in radioactivity and cost. The expense of radiotracers restricts patient scanning and study participation, while radioactivity poses risks, deterring clinical trial enrollment. To enhance PET scalability, reducing injected radiotracer doses without compromising image quality is crucial [1].We investigated the potential power of deep learning to reduce radiation dose for PET/MR studies. We used ultra-low dose PET for our evaluation of deep learning enhancement. Significantly reducing the injected dose will not only reduce radiation risk in subjects but also provide breakthroughs in PET/MRI scanning protocols, thereby allowing for relatively frequent follow-ups of disease progression in comparison to the current protocols. To enhance the image quality of the ultra-low dose PET images, we propose a deep learning model.
Dataset
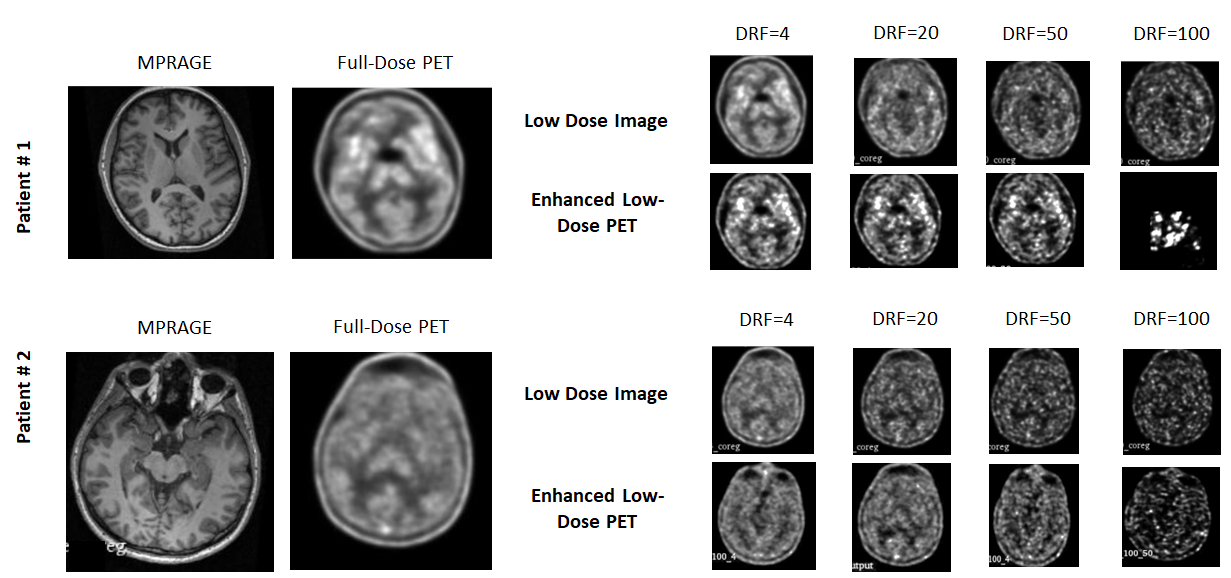
Our dataset comprises 196 brain PET/magnetic resonance (MRI) images (MPRAGE) of healthy volunteers of two sleep deprivation studies, scanned for 100 minutes each using the adenosine A1 receptor ligand [18F]CPFPX (mean injected activity: 179.5 MBq, 10 MBq SD) [2]. We used the baseline part of the sleep deprivation study to determine cerebral A1AR availability after subsequent exposure to rested (BS2), chronically sleep-restricted (CS5), and recovery (RN) conditions [3].Low-dose images from [18F]CPFPX PET scans with Dose Reduction Factor (DRF) of 4, 10, 20, 50, and 100 were corresponding to injected activities of 45, 18, 9, 3.5, and 1.8 MBq. Prompt and random events from the list-mode data were sampled randomly according to the intended dose reduction while keeping all other information like time stamps unchanged.
For improved results, we used an external dataset of 1447 subjects of whole-body 18F-FDG PET imaging, acquired from Siemens Biograph Vision Quadra (n=387) and United Imaging uEXPLORER (n=1060) [4] for initial training of our proposed model.
Methods
We propose a 3D-Residual Attention U-Net (3D-RA-UNet) Model. Our model uses U-Net [5] as a baseline model with residual connections, SE blocks, attention blocks, and dilated attention blocks. Short skip connections via residual blocks simplify network optimization, accelerate convergence, and boost accuracy by increasing model depth. Each attention block captures specific semantic responses, improving the model's representation ability by adjusting features at different levels. Attention blocks in skip connections eliminate irrelevant information, focusing on interdependent feature maps for refined segmentation predictions. The bottom layer is replaced with a dilated attention convolutional layer, connecting the encoder and decoder. Global Average Pooling in the attention block compresses original feature maps, extracting high-level semantic information for feature dimensionality reduction.We used the Transfer Learning approach for improved performance of our 3D-RA-UNet model. Firstly, we trained our model using an external dataset where each scan has low-dose images with DRF at 4, 10, 20, 50, and 100, as well as full-dose images. Fine-tuning was done using Siemens Biograph Vision Quadra (n=387) dataset.
For the second training phase on our in-house dataset, we used the 80:20 ratio for the training and testing. Out of 196, 40 patients were used for testing of our proposed model. For the evaluation of the proposed method, we used four metrics namely Peak Signal-to-Noise Ratio (PSNR), Structural Similarity (SSIM), Normalized Mean Squared Error (NMSE), and Contrast-to-Noise Ratio (CNR).
Results & Discussion
Predicted enhanced low-dose scans were highly perceptually similar to input scans with an average PSNR for the U-Net model was 21.23 dB whereas our proposed model coupled with the transfer learning approach resulted in 28.02 dB. Our proposed model achieved an SSIM of 0.81, CNR of 0.72, and NMSE of 0.33 whereas the U-Net model achieved an SSIM of 0.53, CNR of 0.61, and NMSE of 0.67. Our proposed model can synthesize enhanced low-dose images that have considerably reduced noise compared to the ultra-low-dose PET image and resemble the standard-dose PET image.Conclusion
Preliminary results highlight the potential of the proposed model for enhancing low-dose PET images using simultaneously acquired MR images and low-dose PET images. Moreover, with additional training datasets, we can improve the training model hyper-parameters and eventually create high-quality PET images from actual low-dose PET/MR images. The results of this work can potentially contribute to the implementation of kinetic modeling using PET/MR imaging. Furthermore, the proposed model can be used for both whole-body and brain datasets. This project can potentially increase the utilization of PET/MRI with less radiotracer amount, and thus replace the conventional PET/MR with ultra-low-dose PET/MR for patients who require frequent follow-ups and for study volunteers. Substantially decreasing the injected radiotracer dose for PET/MR scanning can create possibilities for research within safe radiation limits such as multiple PET scans for clinical trials, multi-tracer studies, and longitudinal investigations into disease progression.Acknowledgements
This work was supported by the HIDA Research Grant from Helmholtz Information and Data Science Academy (HIDA). Authors acknowledge Xue Song, Kuangyu Shi & Axel Rominger, Dept. of Nuclear Medicine of the University of Bern, Hanzhong Wang, Rui Guo & Biao Li, Ruijin Hospital, Shanghai Jiao Tong University as the source of the external dataset used for the training proposed model.References
[1] Chen, Kevin T., et al. "True ultra-low-dose amyloid PET/MRI enhanced with deep learning for clinical interpretation." European Journal of Nuclear Medicine and Molecular Imaging 48, (2021): 2416-2425.
[2] Bauer, A., et al. "Evaluation of 18F-CPFPX, a novel adenosine A1 receptor ligand: in vitro autoradiography and high-resolution small animal PET". Journal of Nuclear Medicine 44(10), (2003):1682–1689.
[3] Pierling, A.L., et al. "Cerebral a1 adenosine receptor availability in female and male participants and its relationship to sleep". NeuroImage 245 (2021): 118695.
[4] Xue S., et. al. "A cross-scanner and cross-tracer deep learning method for the recovery of standard-dose imaging quality from low-dose PET". European Journal of Nuclear Medicine and Molecular Imaging (2021): 1-14.
[5] Ronneberger, O., et al. "U-net: Convolutional networks for biomedical image segmentation". In: Medical Image Computing and Computer-AssistedIntervention–MICCAI 2015: 18th International Conference, Munich, Germany, October 5-9, Proceedings (2015): 234-241.
Figures
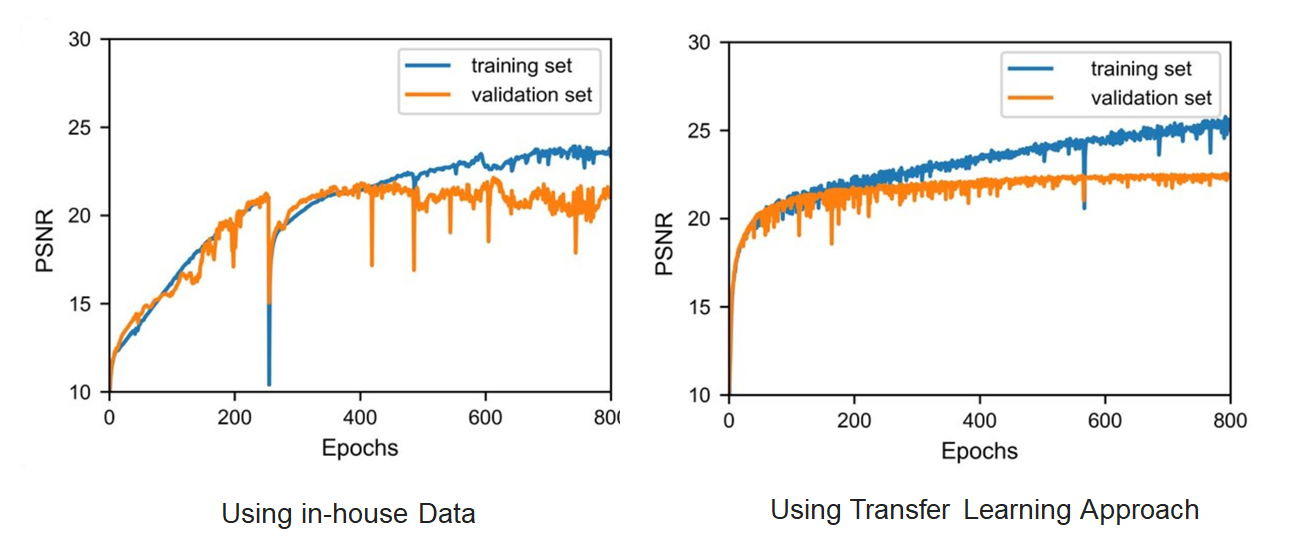
Experimental results on our in-house datasets show that our 3D-RA-UNet model coupled with the transfer learning approach (initial training on the external dataset) significantly improved the PSNR value.