1970
Compressed sense acquisition with artificial intelligence based denoising: evaluation in ultra-high field high resolution resting-state fMRI1Advanced Imaging Research Center, University of Texas Southwestern Medical Center, Dallas, TX, United States, 2Philips Healthcare, Cambridge, MA, United States, 3Philips Healthcare, Best, Netherlands
Synopsis
Keywords: AI/ML Image Reconstruction, Brain Connectivity, Analysis/Processing, AI/ML Image Reconstruction
Motivation: Compressed Sense (CS) acquisition in combination with novel deep learning-based reconstructions has been shown as a viable acceleration technique that brings about additional artificial intelligence (AI) based denoising.
Goal(s): Here, we investigate the impact of CS-AI acceleration and denoising on high-resolution resting-state (rs)-fMRI analysis.
Approach: CS was performed, and different reconstruction methods were compared: (i) conventional CS, (ii) CS with moderate SmartSpeed AI based denoising and (iii) CS with strong SmartSpeed AI based denoising.
Results: Our preliminary results indicate that the underlying reconstruction CS nets do not introduce “artificial” noise or bias and are capable of generating the expected neuronal networks.
Impact: Increasing the rs-fMRI resolution, without sacrificing fidelity in functional connectivity maps, via the application of CS-AI, will lead to higher confidence in human brain mapping, thus reducing the number of participants needed to detect differences between healthy and clinical populations.
Introduction
Ultra-high field resting state (rs)-fMRI takes advantage of the additional SNR afforded by the higher spin populations. This increased SNR is often spent for increased spatial resolution. Accelerated imaging is desirable in such settings as higher acquisition matrices may reduce the temporal resolution, thereby reducing the power to detect underlying connectivity maps. Prolonged scanning sessions leading to motion artifacts and reduced patient comfort are additional limitations. Traditional acceleration techniques such as SENSE and GRAPPA are being superseded by Compressed SENSE (CS) acquisitions to overcome such barriers. CS in combination with novel deep learning-based reconstructions has emerged as a viable acceleration technique that brings about additional artificial intelligence (AI) based denoising[1]. Here, we investigate the impact of CS-AI acceleration and denoising on high-resolution rs-fMRI analysis.Methods
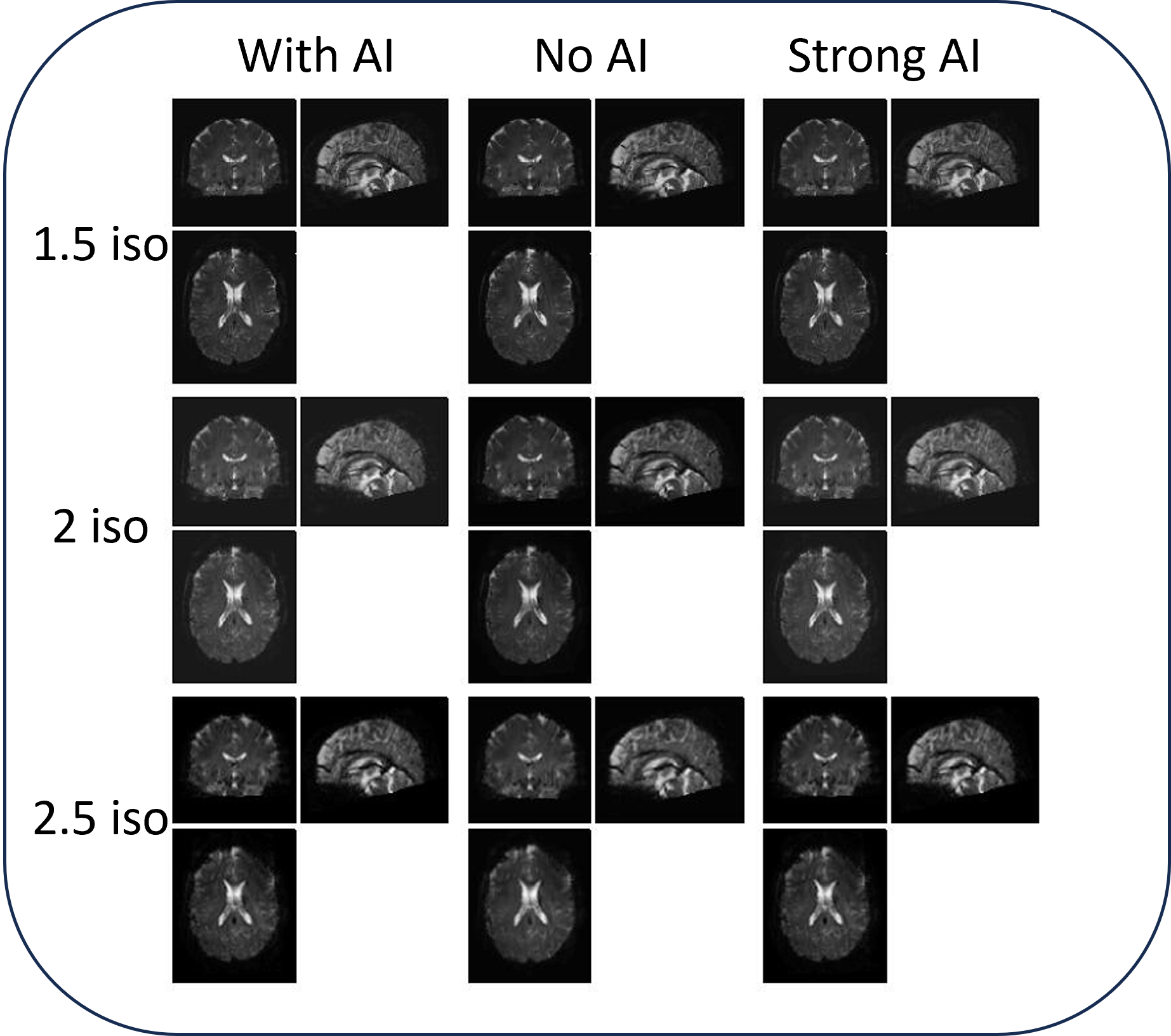
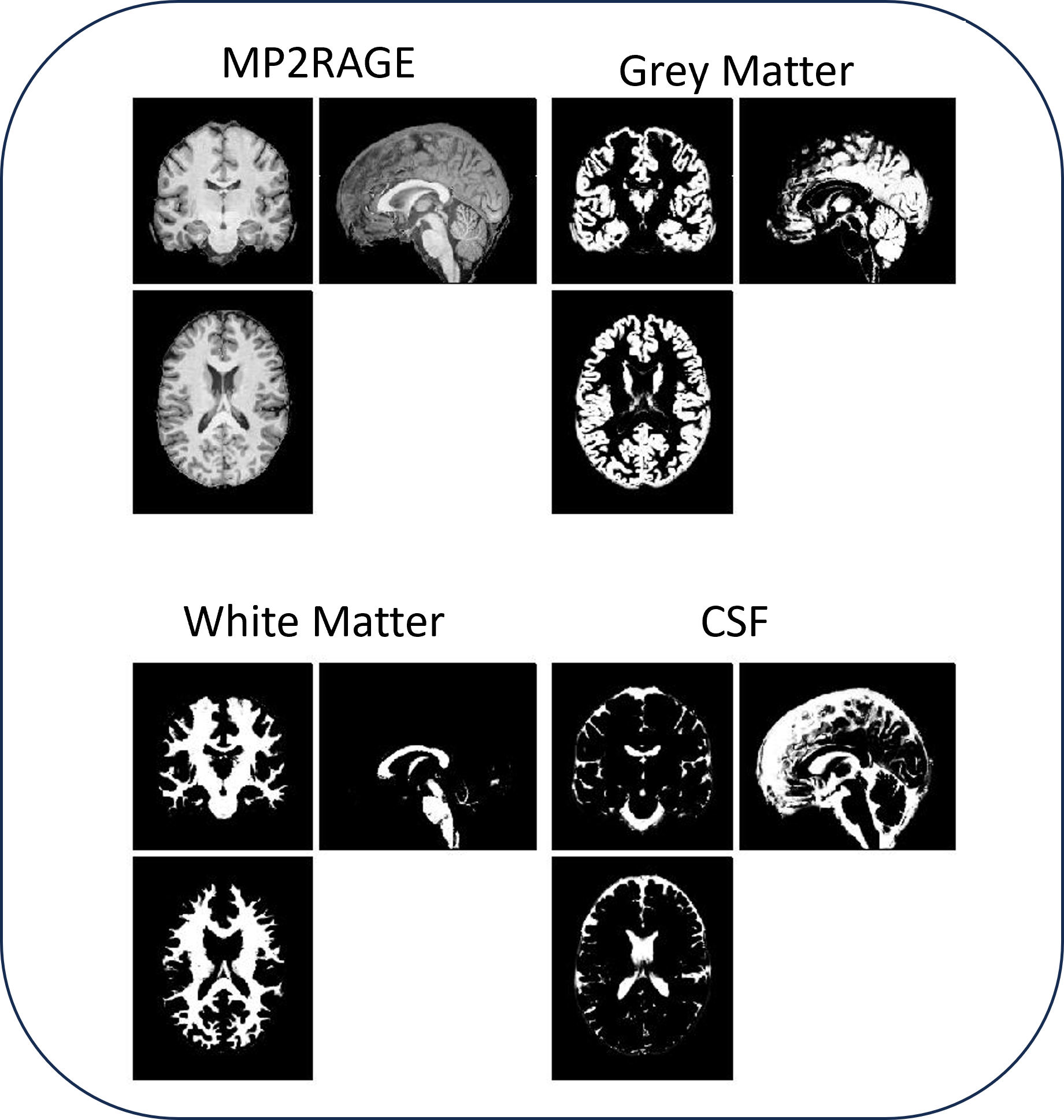
Data Acquisition: 7T whole body MRI scanner (dSync, Philips Healthcare) using a 2-ch transmit, 32-ch receive head coil (Nova Medical). CS acceleration was performed, and different reconstruction methods were compared: (i) conventional CS (“no AI”), (ii) CS with moderate SmartSpeed AI based denoising (“AI”) and (iii) CS with strong SmartSpeed AI based denoising (“strong AI”). SmartSpeed AI uses an iterative CS reconstruction from under sampled k-space acquisition with subsequent AI based denoising[2,3]. MP2RAGE was acquired with 0.8 mm isotropic resolution, acceleration and denoising using CS-AI ×8, 2-channel phase RF shimming (scan duration: 4’:13”). The rs-fMRI scans were acquired with a 10-minute EPI acquisition with various isotropic resolutions, 2.5 mm, 2.0 mm, and 1.5 mm, all using CS-AI ×3, TR 2 s (two shots per image for a 4-s dynamic time), SPIR fat suppressed, foot-to-head coverage of 10 cm. Images reconstructed with AI were compared to the same acquisition but without AI, or with AI with strong denoising[2]. Due to the different resolutions, the EPI train-lengths were 25/31/41 ms for the 2.5/2.0/1.5 mm resolutions, leading to slightly increased distortions for the longer EPI trains.Preprocessing: Resting-state fMRI data from one participant were preprocessed in SPM12 with realignment with respect to the first volume and normalization to MNI space with respect to the EPI template (Fig.1). MP2RAGE data were normalized into standard MNI space, segmented into grey matter, white matter, and CSF tissue classes, and resampled to 2 mm isotropic voxels following a direct normalization procedure using SPM unified segmentation and normalization algorithm[4] (Fig.2). CONN Toolbox[5] was used for additional preprocessing steps such as bandpass filtering (0.008-0.09 Hz). CompCor[6] noise components within white matter and CSF were estimated by computing the average BOLD signal as well as the largest principal components orthogonal to the BOLD average, motion parameters, and outlier scans (identified using ART[7] as acquisitions with framewise displacement>0.5 mm or global BOLD signal changes>3 standard deviations).
Analysis: Connectivity maps were estimated using a representative seed region of interest (ROI) provided with CONN[5]. Functional connectivity strength was represented by Fisher-transformed bivariate correlation coefficients from a weighted general linear model, defined separately for each pair of seed ROI and target areas, modeling the association between their BOLD signal timeseries.
Results
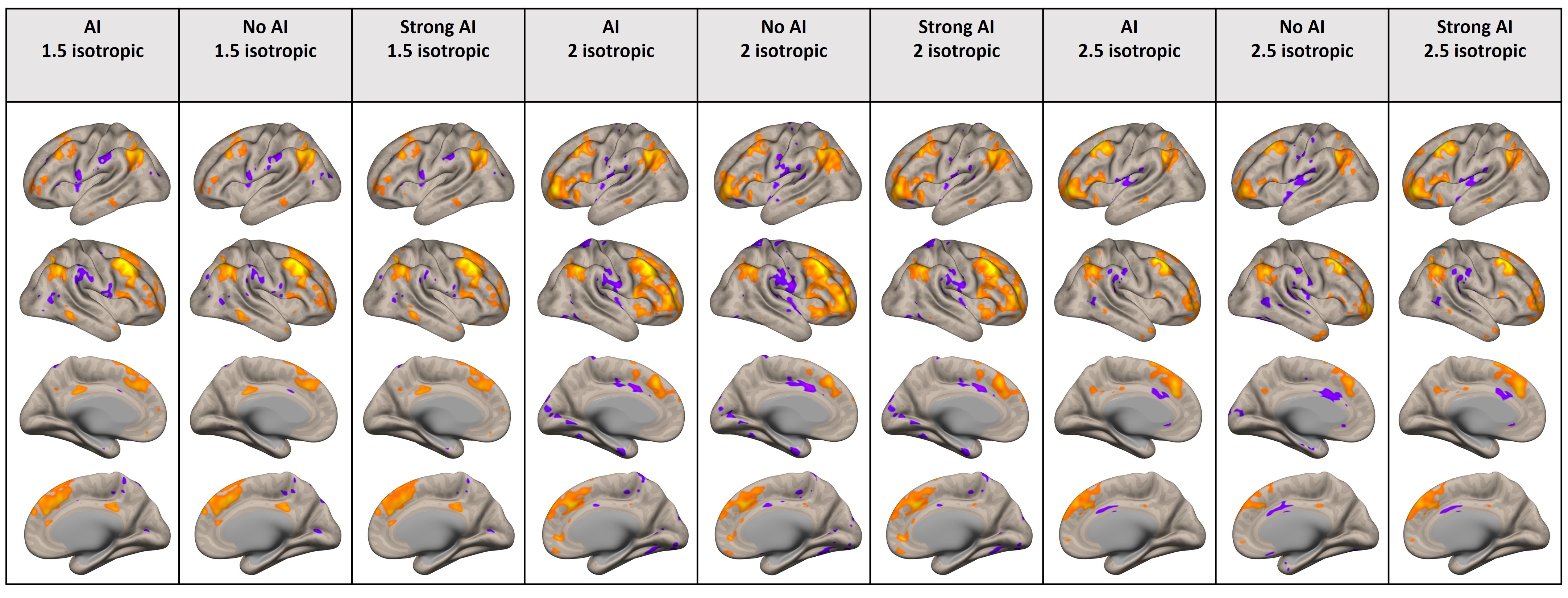
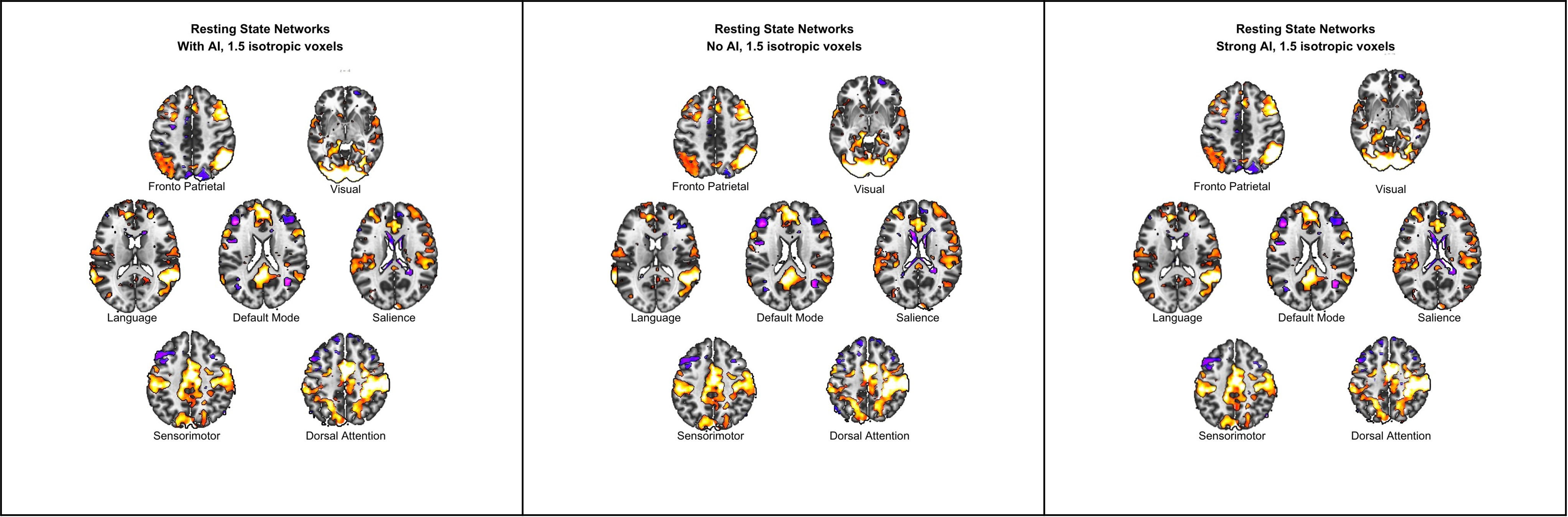
Fig.3 shows a comparison of the reconstruction with the vendor-default AI, without any AI, or with strong AI reconstruction, for the different resting-state networks from the 1.5 mm isotropic resolution. These three comparisons were generated based on the same EPI acquisition, with the AI being applied post-acquisition. Importantly, while allowing for the acceleration of the acquisition (and thus higher resolution), the application of AI-denoising does not result in neither altering nor removing the underlying physiological neural signal that guides the construction of the connectivity maps. Fig.4 shows a comparison of the default mode network (DMN), for the three different resolutions, with and without the application of AI-based reconstruction. These results confirm that AI denoising does not bias the resting state networks. Although the voxels acquired with 1.5 mm isotropic resolutions are 5 times (volume-wise) smaller than the corresponding 2.5 mm voxels, the retention of the underlying physiological neuronal activity signals also results in faithful reconstruction of the DMN. Fig.5 shows similar comparisons for the fronto-parietal network.Discussion
This preliminary study of the application of CS-AI acceleration for the purposes of increasing the acquisition resolution of rs-FMRI indicates that the underlying reconstruction CS nets do not result in the introduction of “artificial” noise or bias and are capable of generating the expected neuronal networks. Since this is a feasibility study, no statistical conclusions can be drawn. Further studies to increase the number of participants is in consideration.Conclusion
Preliminary data suggests that CS-AI acceleration allows for increased spatial resolution of rs-fMRI at 7T such that resting-state networks can be reconstructed with adequate confidence.Acknowledgements
The authors would like to thank the Advanced Imaging Research Center, University of Texas Southwestern Medical Center for the technical support.References
- Iuga AI, Rauen PS, Siedek F, Große-Hokamp N, Sonnabend K, Maintz D, Lennartz S, Bratke G. A deep learning-based reconstruction approach for accelerated magnetic resonance image of the knee with compressed sense: evaluation in healthy volunteers. Br J Radiol. 2023 Jun 1;96(1146):20220074. doi: 10.1259/bjr.20220074. Epub 2023 Apr 22. PMID: 37086077; PMCID: PMC10230385.
- N. Pezzotti et al., "An Adaptive Intelligence Algorithm for Undersampled Knee MRI Reconstruction," in IEEE Access, vol. 8, pp. 204825-204838, 2020, doi: 10.1109/ACCESS.2020.3034287.
- Pezzotti, Nicola et al. “Adaptive-CS-Net: FastMRI with Adaptive Intelligence.” arXiv: Image and Video Processing (2019).
- Ashburner, J. (2007). A fast diffeomorphic image registration algorithm. Neuroimage, 38(1), 95-113.
- Nieto-Castanon, A. & Whitfield-Gabrieli, S. (2022). CONN functional connectivity toolbox: RRID SCR_009550, release 22. doi:10.56441/hilbertpress.2246.5840.
- Behzadi, Y., Restom, K., Liau, J., & Liu, T. T. (2007). A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. Neuroimage, 37(1), 90-101.
- Whitfield-Gabrieli, S., Nieto-Castanon, A., & Ghosh, S. (2011).
Artifact detection tools (ART). Cambridge, MA. Release Version, 7(19), 11.
Figures
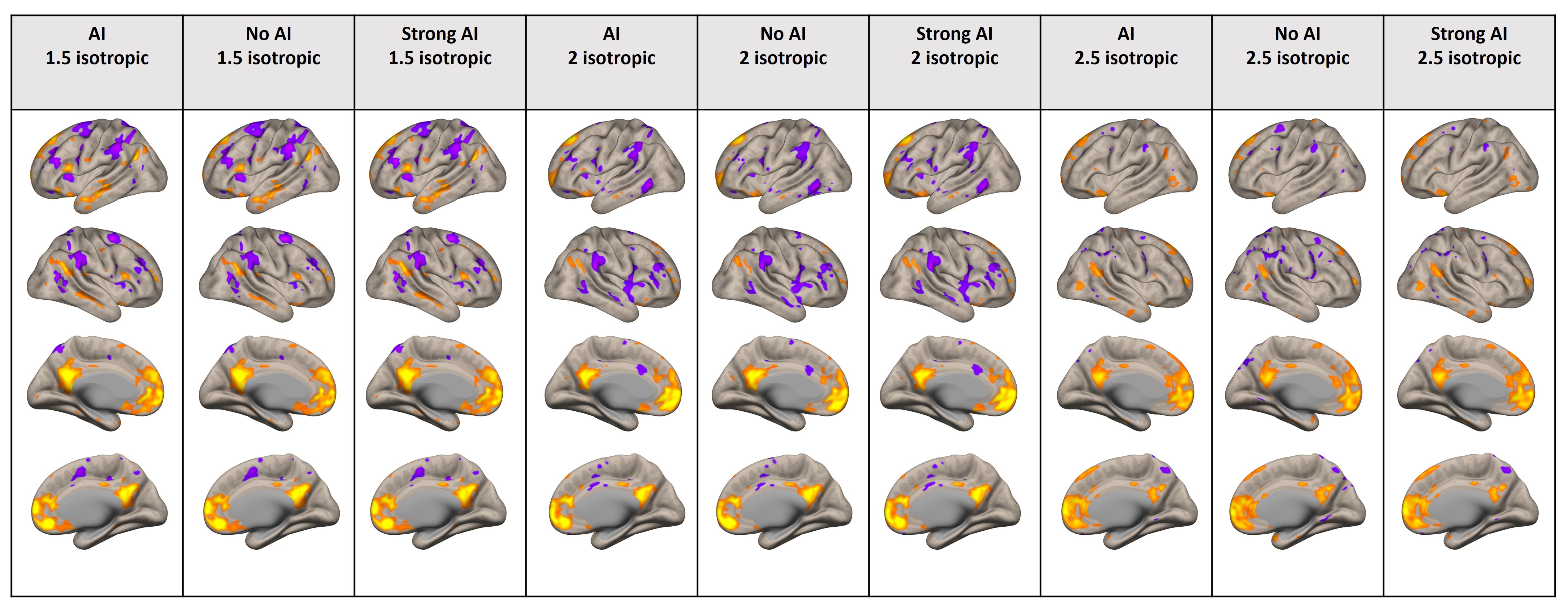
Comparison of the default mode network, for the three different resolutions, with and without the application of AI-based reconstruction. AI = Compressed Sense (CS) reconstruction with moderate SmartSpeed AI based denoising. No AI = Conventional CS reconstruction. Strong AI=CS reconstruction with strong SmartSpeed AI based denoising.