1946
Synthetic-based histogram analysis associated with depth of invasion predicted progression-free survival in nasopharyngeal carcinoma1Department of Diagnostic Radiology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, China, Beijing, China, 2GE Healthcare, MR Research China, Beijing, Beijing, China
Synopsis
Keywords: Head & Neck/ENT, Head & Neck/ENT, Nasopharyngeal carcinoma; Depth of Invasion; Synthetic MRI
Motivation: Deeply infiltrating tumors have a poor prognosis and need close follow-up. Whether the depth of invasion could serve as a quantitative prognostic indicator in NPC. The prognostic assessment value of synthetic MRI (SyMRI) needs further analysis.
Goal(s): To explore the value of two quantitative methods in prognostic assessment in NPC, including depth of invasion and SyMRI.
Approach: This study prospectively included NPC patients, and utilized multiple statistical methods to construct and validate two methods.
Results: Depth of invasion and SyMRI are important quantitative methods.
Impact: Tumor invasion depth is an unignorable metric, and combining it with SyMRI may provide a quantitative and objective approach for clinical treatment.
Introduction
Nasopharyngeal carcinoma (NPC) is an aggressive head and neck cancer. Concurrent chemoradiotherapy with or without induction chemotherapy is the mainstay of treatment for NPC. Patients at the same stage may exhibit different clinical responses and outcomes after receiving similar treatments1. Appropriately 10-30% of NPC patients would suffer treatment failure, including locoregional relapse and distant metastasis. Synthetic MRI (SyMRI) not only generate multiple contrast images in single scan, but also longitudinal and transverse relaxation times (T1 and T2) as well as proton density (PD) of tissues. Previous study2 demonstrated that SyMRI could non-invasively evaluate the status of several prognostic factors in NPC. According to the 8th edition of AJCC staging system, tumors confined to the nasal cavity are classified as stage T1, whereas tumors are classified as high T stage when they invade deeper sites, for example, beyond the lateral margin of lateral pterygoid muscle. Whether the depth of invasion (DOI), a quantitative factor, could serve as a prognostic factor in NPC has not been exploited before. Therefore, based on the concept of quantitative and objective assessment, we explored the prognostic value of DOI in NPC and the combined effect of incorporating SyMRI.Methods
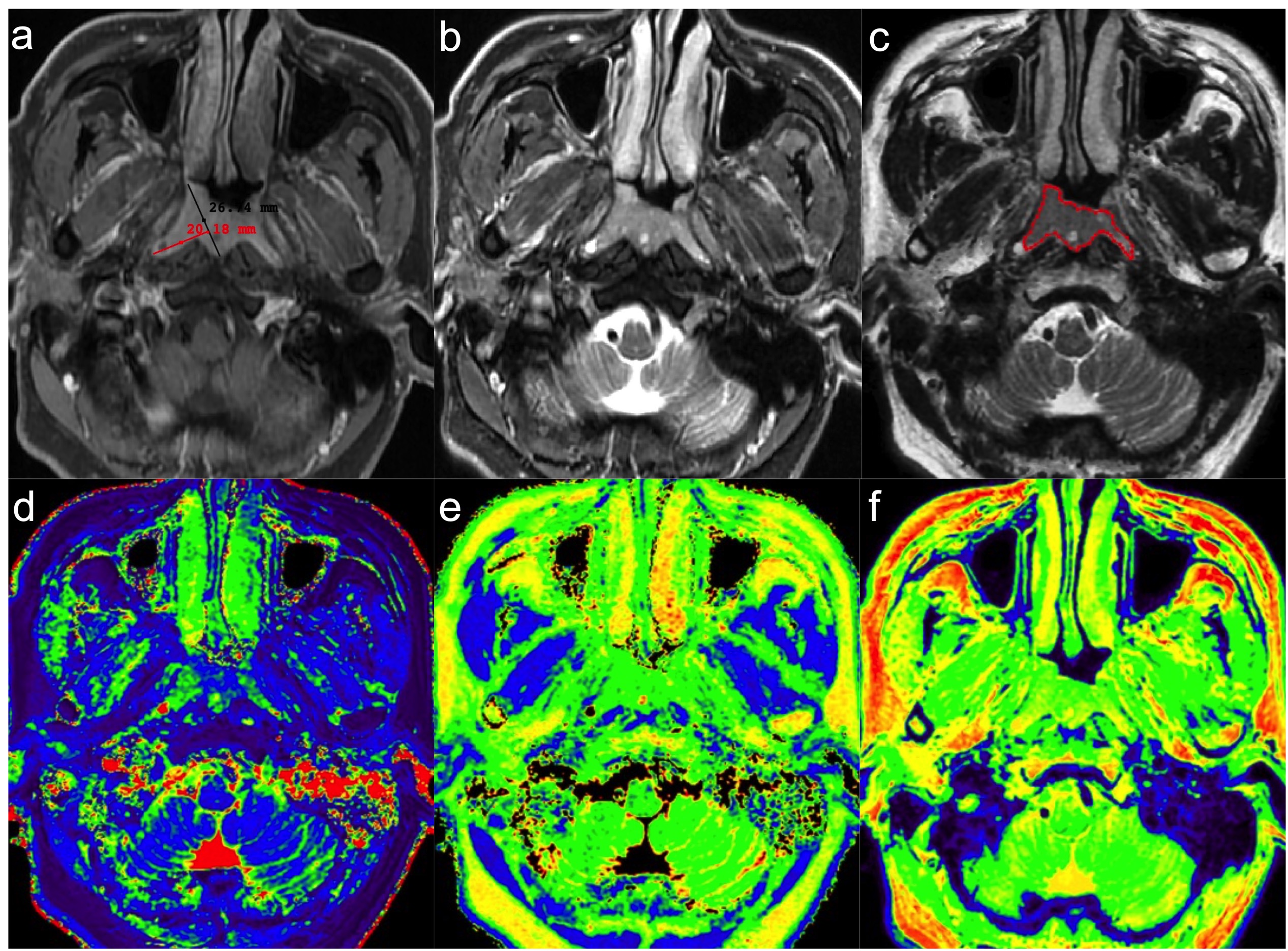
This study prospectively included 53 NPC patients who underwent conventional MRI and SyMRI scans from August 2018 to May 2019. Two radiologists manually delineated the volume of primary tumor, excluding any visible necrosis and cyst areas (Fig.1). Four histogram parameters (10th Percentile, Mean, Kurtosis and Skewness) were obtained from T1, T2, and PD maps through Pyradiomics. Fifty-three patients invaded bilateral posterior nasopharyngeal wall more or less in radiologic imaging. The DOI (Fig.1) was defined as the length of tumor perpendicular to the reference line towards the medial side of the tissue. The reference line was connected the center of posterior nasopharyngeal wall (between bilateral longus capitis muscle) and the front of lateral nasopharyngeal wall (or the front of tumor when it not extent beyond lateral nasopharyngeal wall). Two radiologists independently measured the depth on contrast-enhanced T1WI3. The average value between two radiologists were further evaluated.All patients underwent standard treatment and follow-up. Imaging examination (CT, MRI, US, PET-CT and bone scan) and/or biopsy was used. Progression-free survival (PFS) was defined as the time from the start of treatment to the date of disease progression (local-regional or distant), death, or last follow-up, whichever occurred first. The last follow-up set for July 30, 2022.
The two-way random interclass correlation was used to evaluate the interobserver consistency. Univariate Cox proportional hazards regression analysis was performed to assess the correlation of DOI and SyMRI parameters with PFS. Significant parameters were further entered in multivariate Cox regression analysis. The C-index and 95% confidence interval (95% CI) were obtained by bootstrap (n = 1000). The optimal threshold values were obtained using R studio. The survival rate was calculated by using Kaplan–Meier analysis and differences were compared using log-rank test.
Results
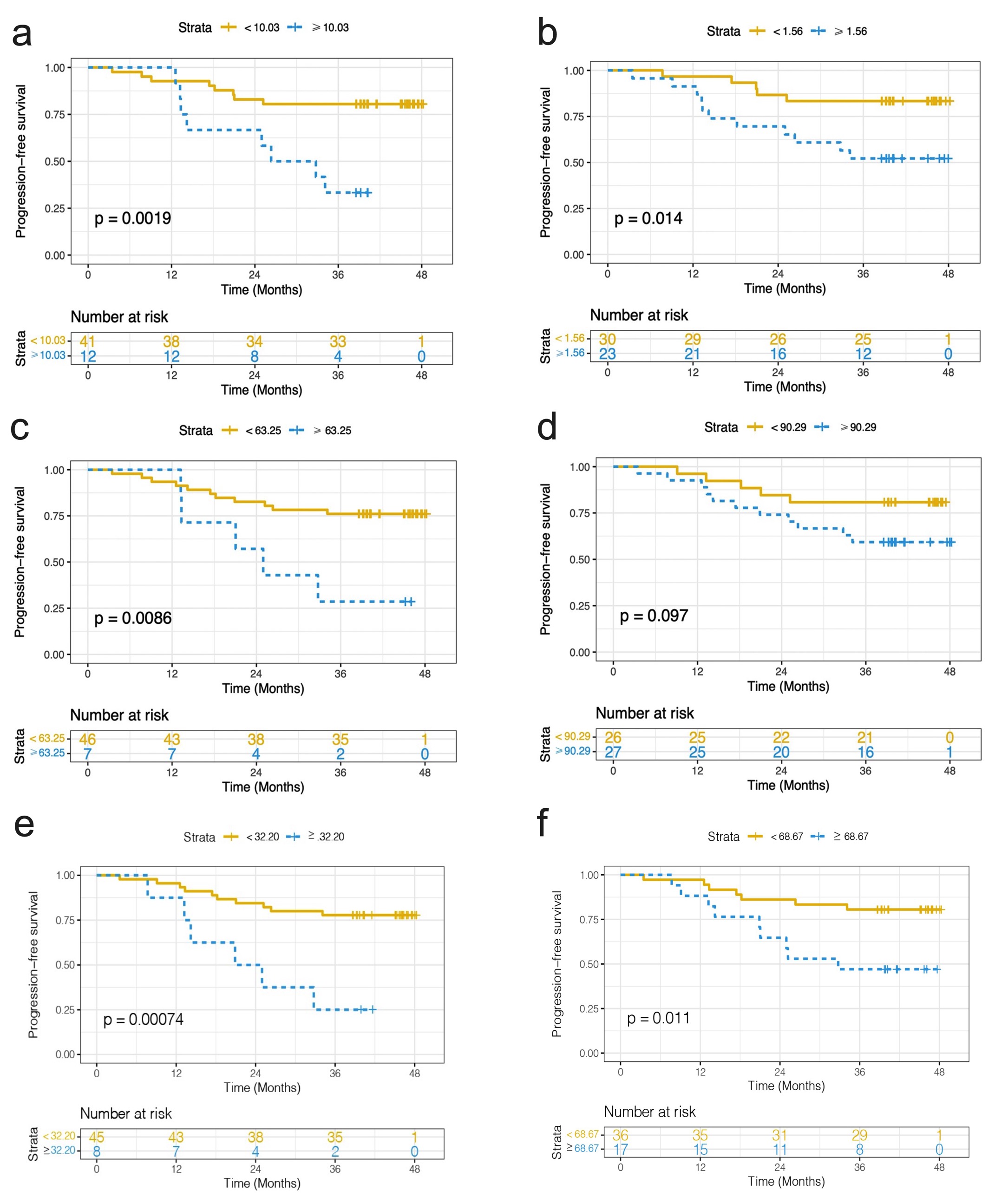
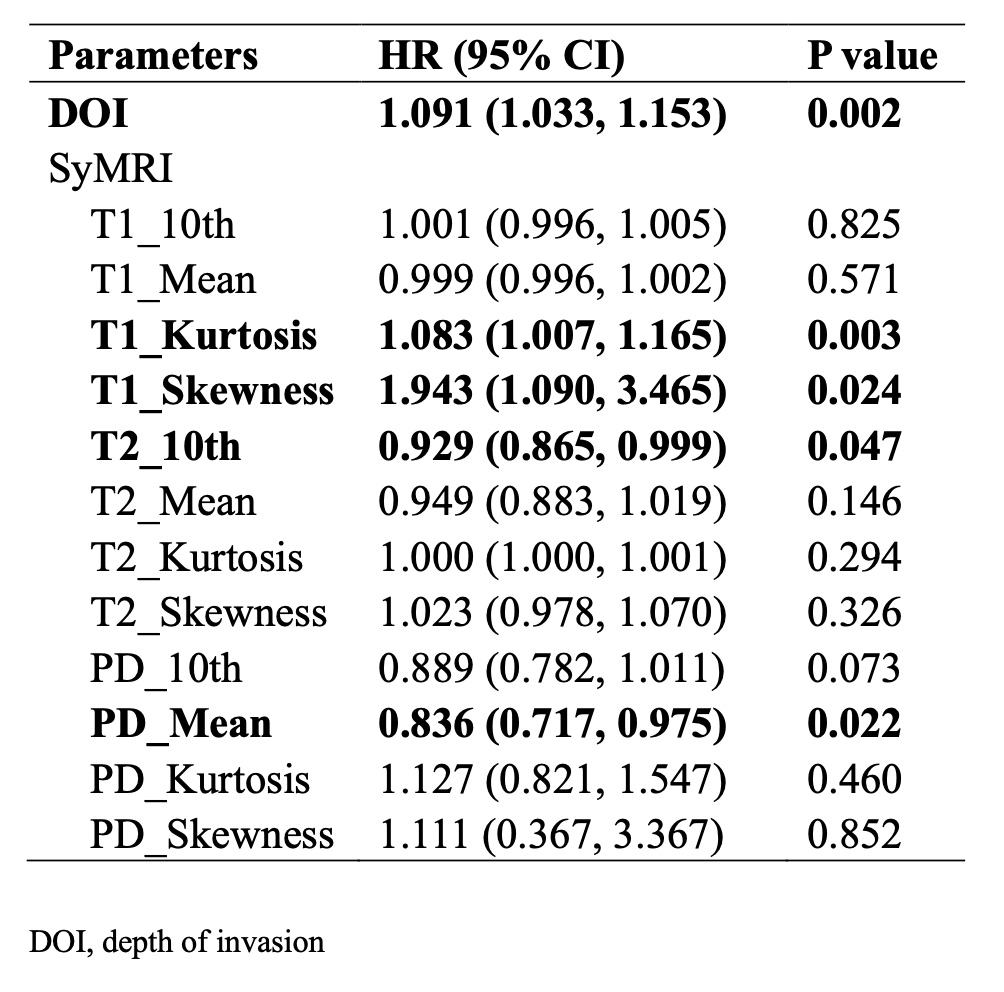
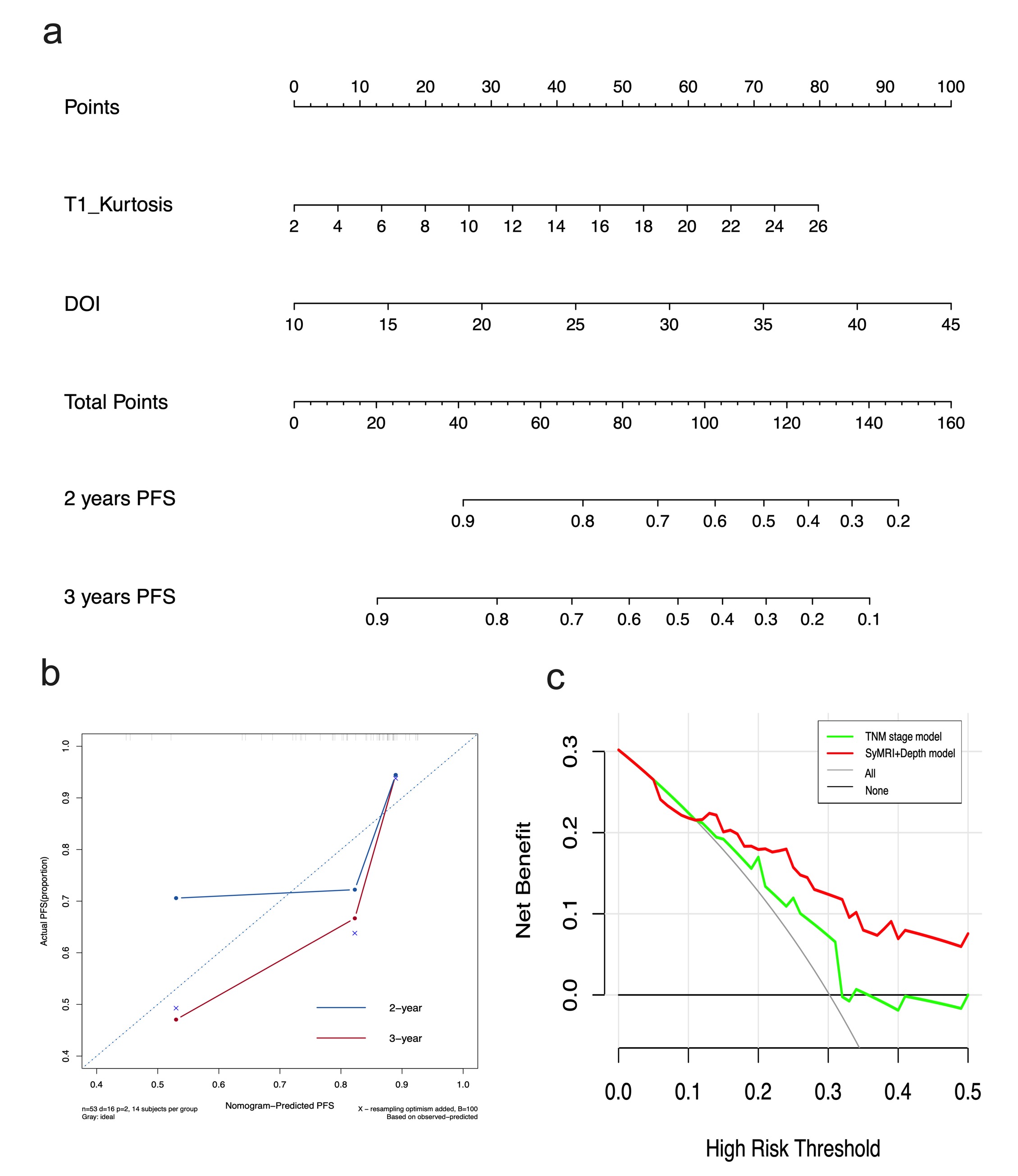
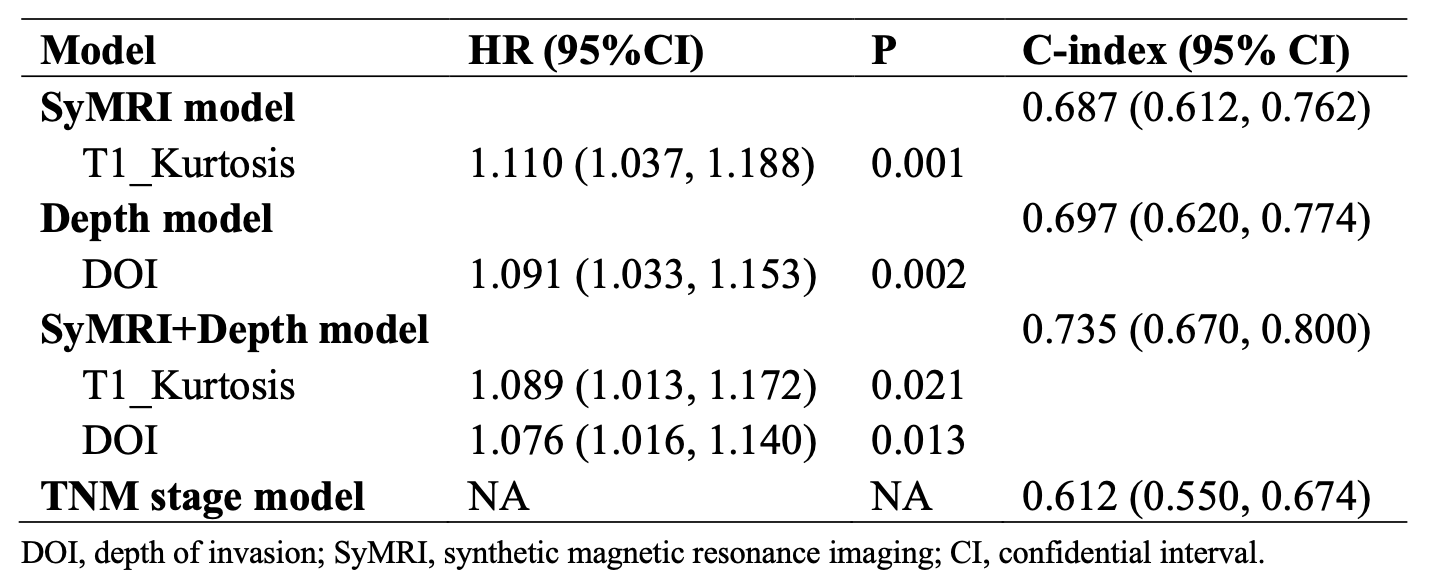
16/53 (30.2%) patients were diagnosed with disease progression and the median follow-up duration for all patients was 39.6 (3.5, 48.2) months. All parameters showed excellent inter-rater consistency (all ICC ≥ 0.891). Several parameters were significantly correlated with PFS (Fig.2 and Fig.3) and T1_Kurtosis was finally selected to construct SyMRI model after multivariate Cox regression analysis.T1_Kurtosis (HR=1.089, P=0.021) and DOI (HR=1.076, P=0.013) were selected to construct SyMRI + Depth model, and the nomogram and calibration curves are shown in Fig.4. The C-index of SyMRI + Depth model (0.735) was higher than that of TNM stage model (0.612) and the decision curve analysis was shown in Fig.4. The C-index of models are shown in Fig.5.
Discussion
Deeply infiltrating tumors, which are defined as high T stage, have poor prognosis. The complexity of the peri-nasopharyngeal anatomy and subtle infiltration may cause diagnostic difficulties. This study provided an objective assessment method (DOI), using reference line to eliminate individual differences as much as possible. Moreover, the value of SyMRI could not be ignored. A large sample research is being conducted at our institution to eliminate small-sample deficiencies.Conclusion
In NPC, quantification of tumor infiltration is a well-performing prognostic predictor. Combining two quantitative methods could provide an objective method in prognostic assessment.Acknowledgements
No acknowledgement found.References
1, Zhang L, Huang Y, Hong S, et al. Gemcitabine plus cisplatin versus fluorouracil plus cisplatin in recurrent or metastatic nasopharyngeal carcinoma: a multicentre, randomised, open-label, phase 3 trial. Lancet 2016;388(10054):1883-1892.
2, Yang F, Li X, Li Y, et al. Histogram analysis of quantitative parameters from synthetic MRI: correlations with prognostic factors in nasopharyngeal carcinoma. Eur Radiol 2023.
3, Baba A, Masuda K, Hashimoto K, et al. Correlation between the magnetic resonance imaging features of squamous cell carcinoma of the buccal mucosa and pathologic depth of invasion. Oral Surg Oral Med Oral Pathol Oral Radiol 2021;131(5):582-590.
Figures