1936
Vascular Involvement Associated with Hypertension in Trigeminal Neuralgia Patients1Heibei General Hospital, Shijiazhuang, China, 2GE Healthcare, Beijing, China
Synopsis
Keywords: Head & Neck/ENT, Nerves
Motivation: Trigeminal neuralgia is characterized by vascular compression of the trigeminal nerve, while neurogenic hypertension results from vascular compression in the medulla oblongata.
Goal(s): To investigate the pathogenesis of TN in conjunction with hypertension and identify the vessels responsible,
Approach: we conducted a retrospective population-based study including 457 TN patients,
Results: and found a significant link between neurovascular conflict and hypertension. Specifically, arteries near the root entry zone, such as the anterior inferior cerebellar artery, vertebrobasilar artery, and superior cerebellar artery, were more associated with hypertension, especially when pain localized in the V2,3 area. Conversely, the posterior inferior cerebellar artery displayed an opposing trend.
Impact: Patients with TN combined with neurogenic hypertension are recommended to take microvascular decompression (MVD) operation, who have these conditions in our study, will show potential improvements in their hypertension.
Introduction
Trigeminal neuralgia (TN) is a chronic neuropathic pain condition resulting from neurovascular conflict, while neurogenic hypertension primarily arises from elevated blood pressure due to vessel compression in the medulla oblongata. The causal connection between hypertension and TN has been a subject of debate. Our study aimed to examine the onset of TN and hypertension by analyzing the association between conflicting blood vessels and hypertension.Methods
To explore the relationship between hypertension and neurovascular conflict (NVC), we conducted a retrospective population-based study. We gathered data from 484 cases of TN patients admitted for neurosurgery at our hospital between October 2019 and November 2022. Ultimately, 457 patients were included in our final analysis. Based on MRI imaging, we categorized the conflicting vessels into several groups, including the superior cerebellar artery (SCA), anterior inferior cerebellar artery (AICA), posterior inferior cerebellar artery (PICA), vertebrobasilar artery (VBA), unidentified vessels (e.g., arteries like internal carotid artery branches, veins like petrosal vein), and cases without NVC. Additionally, we determined whether these conflicting vessels were located in the root exit zone (REZ) or not. We defined resistant hypertension as office BP≥140/90 mm Hg, even when managed with appropriate lifestyle modifications along with a diuretic and two other antihypertensive drugs.1 We employed Fisher's exact tests and a multivariate logistic regression model, building upon single-factor analysis, to identify independent risk factors. Statistical significance for the odds ratios tables was determined using a χ2 test.Results
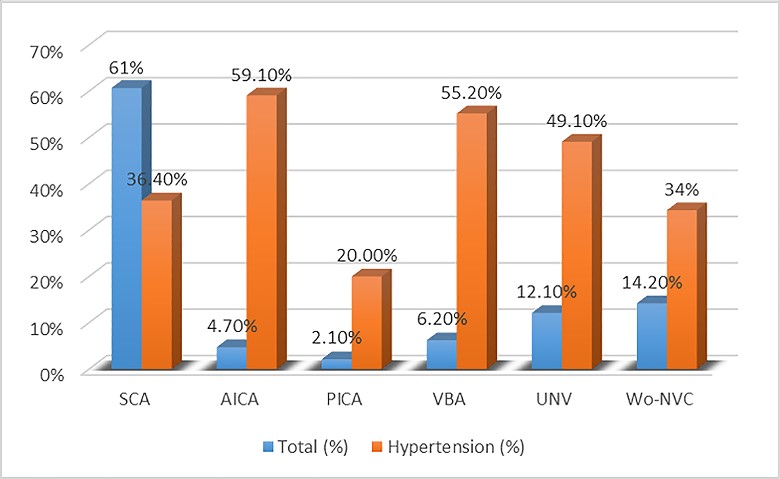
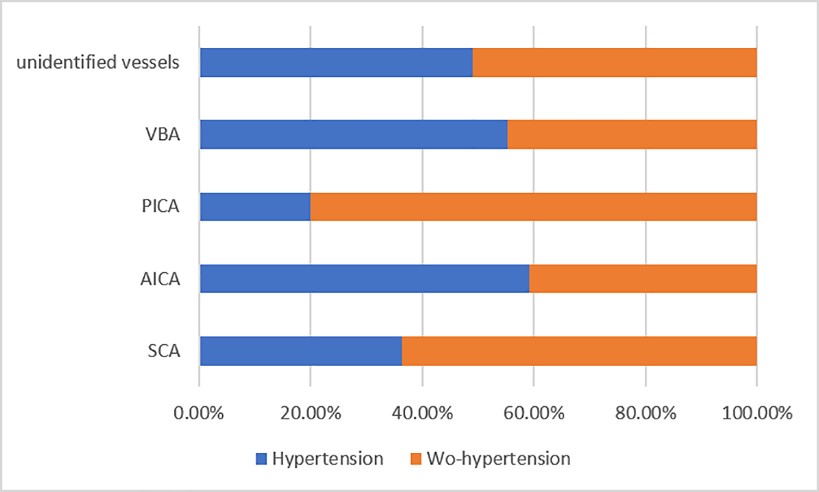
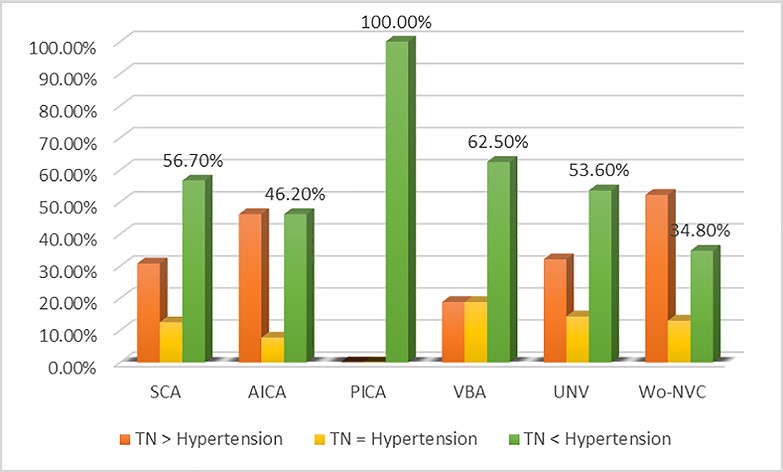
Hypertension occurred in 40% of the cases, with varying rates among different vessels: 36.4% (104/286) in cases with SCA involvement, 59.1% (13/22) in AICA cases, 55.2% (16/29) in VBA cases, 49.1% (28/57) in cases with unidentified vessels, and 20% (2/10) in PICA cases (Figure 1). Among the vascular conflicts leading to TN, SCA was responsible for 60% (286/471) of cases, while 15.5% (69/471) showed no evidence of NVC, and only 2.1% (10/471) were attributed to PICA. Notably, patients with AICA, VBA, and unidentified vessels who had hypertension exhibited the highest incidence of hypertension, collectively accounting for half of the hypertension cases (Figure 2). AICA, VBA, and unidentified vessels were associated with a higher likelihood of hypertension (OR 2.768, 2.360, and 1.848, respectively), while PICA was less likely to be linked to hypertension (OR 0.479, CI 0.252-0.909, p = 0.024). SCA in the REZ area was typically associated with hypertension, with an odds ratio of 2.857. Regarding onset timing, TN occurring before hypertension was the most prevalent scenario (106 cases), followed by TN onset after the onset of hypertension (60 cases), and simultaneous onset of TN and hypertension (16 cases) (Figure 3). The V2,3 distribution areas accounted for the highest proportion (29.7%) and were more likely to be associated with hypertension (OR 1.749, CI 1.147-2.667, p = 0.009).Discussion
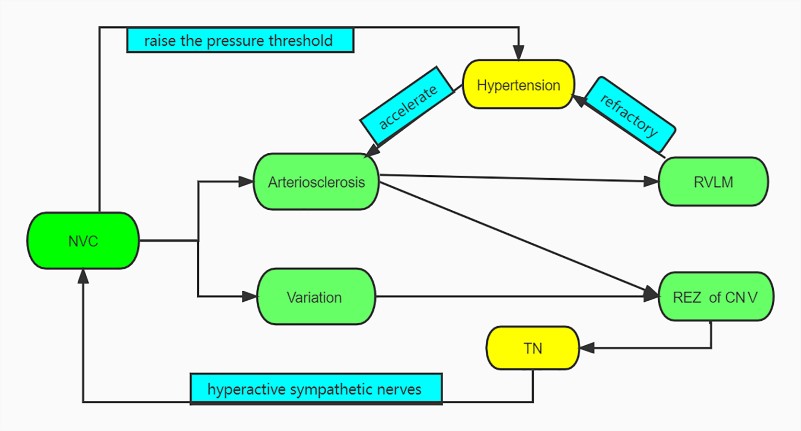
To the best of our knowledge, our study boasts the largest sample size among population studies focusing on TN patients with hypertension.2 Several studies suggest that elevated blood pressure can accelerate arteriosclerosis and vessel distortion, potentially leading to trigeminal nerve compression and TN.3-7 The origin and course of SCA make it prone to trigeminal nerve compression through arteriosclerosis. Trigeminal nerve fibers enter the pons via the REZ, influencing the cardiac sympathetic excitatory reflex in the medulla oblongata.8, 9 Our findings highlight SCA's presence in the REZ as an independent risk factor for TN with hypertension. Most studies emphasize neurogenic hypertension resulting from RVLM compression. RVLM vascular decompression can lower blood pressure. 10-14Neuronal aggregates near the human VLM's surface may affect cardiovascular function (Figure 4). Our study revealed that half of the medulla's compressing vessels were AICA, increasing the risk of CN III compression. VBA courses through the medulla oblongata, potentially compressing both it and the trigeminal nerve. 5 Thus, MVD is preferred for VBA cases due to the elevated risk of complex hypertension.4, 5, 15, 16 PICA is less likely to be the conflicting vessel in hypertension cases since it's farther from RVLM during CN III compression, reducing the hypertension risk.17 Furthermore, our study unveiled a stronger association between pain distribution in the V2,3 areas and hypertension. These two compressed regions are adjacent to the caudal pons, which has been identified as a potential target for neuromodulation in the treatment of hypertension.18Conclusion
In this study, we conducted a comprehensive analysis of the relationship between hypertension and the location, type, and pain distribution associated with neurovascular conflict (NVC) in TN patients. Our findings aim to enhance the screening process for identifying TN patients with coexisting neurogenic hypertension.Acknowledgements
No acknowledgement found.References
1. Mancia G, Fagard R, Narkiewicz K, Redon J. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 34:2159-2219.2013 2. Sandell T, Holmen J, Eide PK. Hypertension in patients with cranial nerve vascular compression syndromes and comparison with a population-based cohort. J Neurosurg 119:1302-1308.2013 3. El-Ghandour NM. Microvascular decompression in the treatment of trigeminal neuralgia caused by vertebrobasilar ectasia. Neurosurgery 67:330-337.2010 4. Sun S, Jiang W, Wang J, et al. Clinical analysis and surgical treatment of trigeminal neuralgia caused by vertebrobasilar dolichoectasia: A retrospective study. Int J Surg 41:183-189.2017 5. Ma X, Sun X, Yao J, et al. Clinical analysis of trigeminal neuralgia caused by vertebrobasilar dolichoectasia. Neurosurg Rev 36:573-577; discussion 577-578.2013 6. Leonardo D. Oliveira M, Francisco Cardoso, MD, PhD, and Antonio P. Vargas, MD. Hemifacial Spasm and Arterial Hypertension. Movement Disorders 14:832–835.1999 7. Coakham SLaHB. Trigeminal neuralgia Pathology and pathogenesis. Brain 124:2347–2360.2001 8. Burkett DJ, Garst JR, Hill JP, Kam A, Anderson DE. Deterministic Tractography of the Descending Tract of the Spinal Trigeminal Nerve Using Diffusion Tensor Imaging. J Neuroimaging 27:539-544.2017 9. Guyenet PG, Stornetta RL, Souza G, Abbott SBG, Brooks VL. Neuronal Networks in Hypertension: Recent Advances. Hypertension 76:300-311.2020 10. Michael B. Horowitz M. Brainstem Compression as a Cause of Neurogenic Hypertension. Curr Hypertens Rep 3:264–267.1999 11. Patel S, Krishna V, Nicholas J, Welzig CM, Vera C. Preliminary observations on the vasomotor responses to electrical stimulation of the ventrolateral surface of the human medulla. J Neurosurg 117:150-155.2012 12. Elad I. Levy MD, Alan M. Scarrow, M.D., J.D., and Peter J. Jannetta, M.D., D.Sc. Microvascular Decompression in the Treatment of Hypertension: Review and Update. Surg Neurol 55:2–11.2001 13. Lin L, Xie l. Neurogenic hypertension. Chin J Hypertens 25:834-840.2017 14. Elad I. Levy MD, Brent Clyde, M.D.,, Mark R. McLaughlin MD, Peter J. Jannetta, M.D. Microvascular Decompression of the Left Lateral Medulla Oblongata for Severe Refractory Neurogenic Hypertension. Neurosurgery 43:1-6.1998 15. Vanaclocha V, Herrera JM, Martinez-Gomez D, et al. Is There a Safe and Effective Way to Treat Trigeminal Neuralgia Associated with Vertebrobasilar Dolichoectasia? Presentation of 8 Cases and Literature Review. World Neurosurg 96:516-529.2016 16. Arrese I, Sarabia R. Microvascular decompression for trigeminal neuralgia secondary to vertebrobasilar dolichoectasia. Case report, literature review, and pooled case analysis. Neurocirugia (Astur) 27:304-309.2016 17. Lei J, Zhang J, Luo J, et al. MVD treated left multicranial nerve compression with neurogenic hypertension: Two cases report. Chin J Neurosurg Dis Res 16:462-464.2017 18. Hamasaki T, Yamakawa T, Fujiwara K, et al. Sympathetic hyperactivity, hypertension, and tachycardia induced by stimulation of the ponto-medullary junction in humans. Clin Neurophysiol 132:1264-1273.2021Figures