1935
Multiparameter Quantitative MRI in Diagnosing Dysthyroid Optic Neuropathy in Thyroid Associated Orbitopathy1Peking University People's Hospital, Beijing, China, 2Peking University Third Hospital, Beijing, China, 3Philips Healthcare, Beijing, China
Synopsis
Keywords: Head & Neck/ENT, Multimodal, Multiparameter Quantitative MRI
Motivation: Dysthyroid optic neuropathy (DON) is a rare yet highly significant complication of thyroid associated orbitopathy (TAO), which requires urgent treatment. However, diagnosing this condition is a formidable challenge due to the absence of well-defined criteria for its identification.
Goal(s): The aim of this study was to use multiparameter MRI for diagnosing DON.
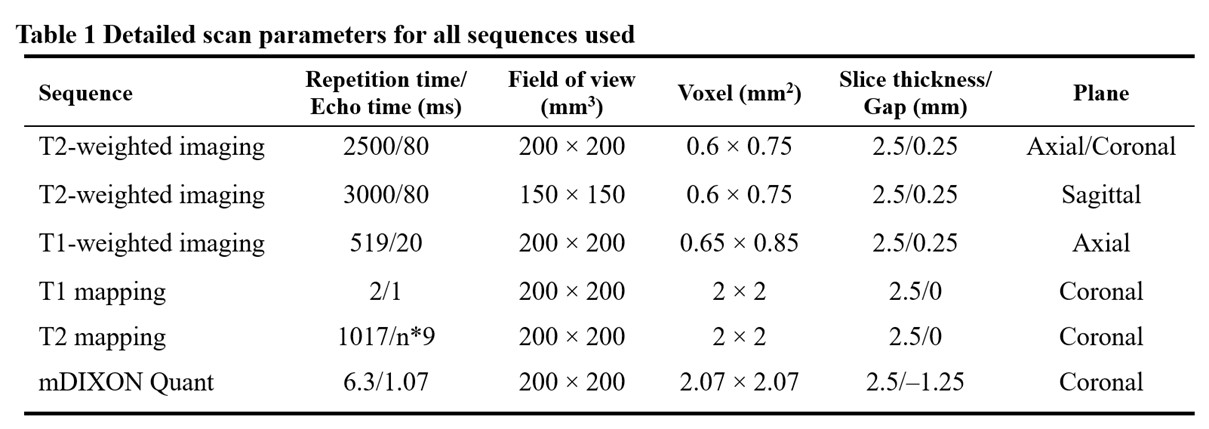
Approach: Fifty-five patients were enrolled, who underwent MRI, including conventional imaging, T1 mapping, T2 mapping, and mDIXON Quant sequences for providing quantitative parameters.
Results: The quantitative parameters could offer reliable evidence for the differentiation of DON from TAO, especially T1 values of extraocular muscles and water fraction of orbital fat.
Impact: The native T1 values of extraocular muscles combined with water fraction of orbital fat provided more accurate diagnostic ability of DON in TAO patients. Moreover, the pathological presentation of fibrosis of extraocular muscles associated with DON may occur.
Introduction
Dysthyroid optic neuropathy (DON) is a rare but with serious complication of thyroid associated orbitopathy (TAO) that demands immediate treatment, including orbital decompression surgery for preventing permanent vision loss1,2. Differentiating DON from active TAO is essential but challenges exhibit due to lack of clear criteria regarding diagnosis of DON3,4. Previous studies have shown that qualitative imaging features, such as muscle crowding and optic nerve stretching, are not sufficient to diagnose DON5. Conventional imaging, T1 mapping, T2 mapping, and mDIXON Quant sequences were used for providing quantitative parameters. The aim of this study was to evaluate the diagnostic ability of multiparameter quantitative MRI for DON by quantitative MR techniques, such as native T1 and T2 mappings.Methods
TAO patients with suspected DON before treatment were scanned using a 3.0 T MRI system (Ingenia, Philips, Netherland) with a 16-channel head coil. Fifty-five patients were enrolled and divided into two groups according to comprehensive clinical criteria3,5,6. The parameters of MR sequences were shown in Table 1 and Figure 1. The indicators of imaging features included degree of proptosis, thickness of all extraocular muscle (EOM), T2 signal intensity ratio (SIR), and muscle index (MI)7. The quantitative parameters included T1, T2 values and fat fraction (FF) values of EOMs as well as water fraction [SIwater/(SIwater+SIfat)] (WF) of orbital fat (OF). T test, Mann-Whitney U test or Fisher exact tests were used to compare parameters between two groups, respectively. Based on selective parameters by stepwise regression, the logistic regression model was constructed and validated by 5-fold cross validation. Receiver operating characteristic (ROC) curves were calculated, and DeLong test were used to compare the performance of single parameters and logistic regression model.Results
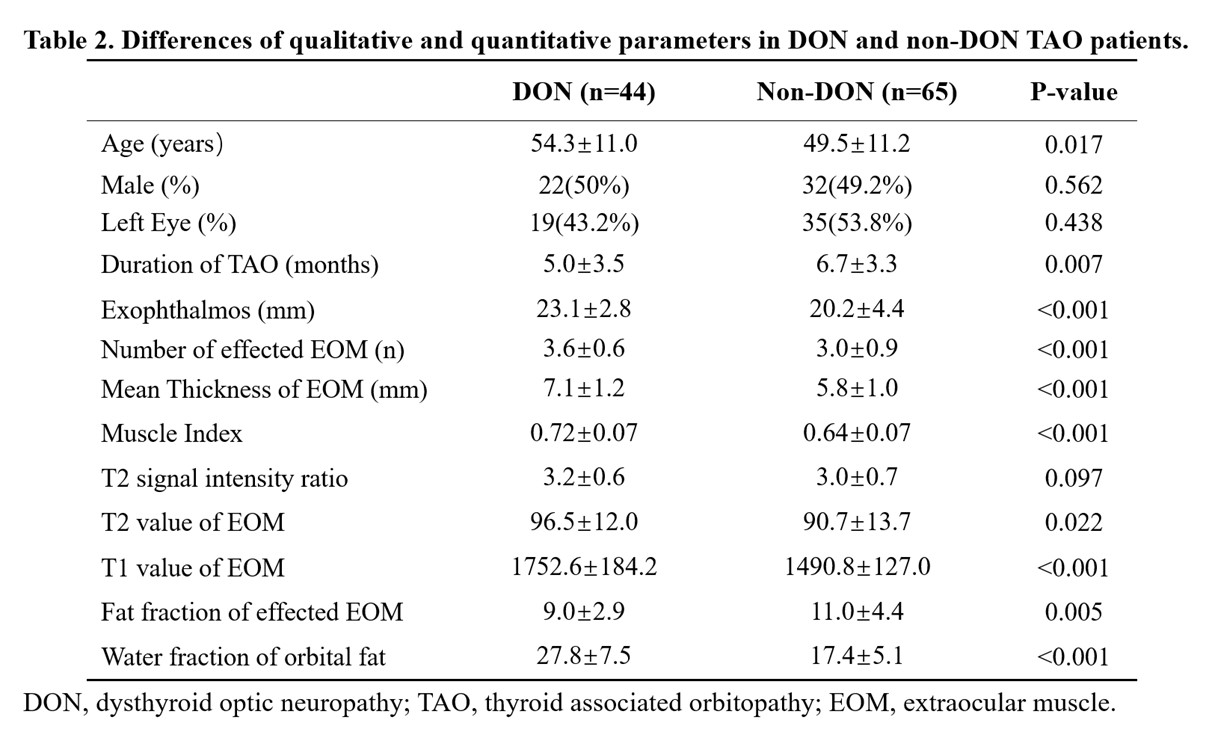
A total of 55 TAO patients with suspected DON underwent orbital MRI from May 2021 to Oct 2023 enrolled in this prospective study. Eventually, 44 eyes were diagnosed as DON, while 65 eyes were ruled out (Table 2). The number and thickness of EOMs, MI, and the degree of exophthalmos were significant higher in DON group (P<0.001). Furthermore, the average T1 value of affected EOMs was longer and the WF of OF were higher in DON group with significant differences(P<0.001). However, SIR, T2 values of EOMs, and FF of EOMs exhibited no significant difference between these two groups (P>0.001). The discriminative performance of logistic regression selected parameters and was presented in Table 3 and Figure 2. The T1 value of EOMs (AUC, 0.876; Sensitivity, 0.867; Specificity, 0.891), WF of OF (AUC, 0.888; Sensitivity, 0.822; Specificity, 0.953) and logistic regression model (AUC, 0.940; Sensitivity, 0.911; Specificity, 0.922) have good diagnostic performance.Discussion
The difficulties in distinguishing DON from other TAO may lead to sight-threatening delays in treatment, but there is still a lack of clear and universally recognized diagnostic criteria5. This study revealed that T1 value of EOM and WF of OF showed significant difference between DON and non-DON group. Moreover, T1 value of EOM and WF of OF could provide effective evidence in distinguishing DON.Compared with subjective imaging characters, T1, T2 mapping and mDIXON-Quant sequences could provide more objective parameters in evaluating the severity of TAO. As a complex autoimmune disease, TAO is characterized by orbital inflammation (active disease) and subsequent tissue remodeling with fibrosis when the disease under the condition of inactive8. We found severe fibrosis in patients with DON with clinical activity score6 ≥ 3. Furthermore, T1 value of EOM and WF of OF were higher in DON patients, but there was no significant difference on T2 value. It could be explained that there were different orbital pathological components between DON and other TAO patients. In DON, orbital edema is primarily attributed to the obstruction of venous reflex rather than accumulation of hydrophilic and interstitial glycosaminoglycans9. Higher water fraction indicated that edema in DON patients was more severe than other active TAO patients10. In the meantime, edema with long T2 and fibrosis with short T2 relaxation time induced the neutralization of T2 value in DON patients, with no significant difference between the two groups. Significant edema and fibrosis could induce the stiffness of EOM, making it easier for them to compress the optic nerve. Furthermore, quantitative imaging parameters could be built as the more effective criteria to evaluate active and inactive TAO than clinical activity score.
Conclusion
T1 values of extraocular muscles and water fraction of orbital tissue have more potential to diagnose TAO patients with DON, which revealed the main pathological presentation of orbital edema caused by venous obstruction and fibrosis in DON.Acknowledgements
None.References
1. Agarwal A, Khanam S. Dysthyroid Optic Neuropathy. In: StatPearls. StatPearls Publishing; 2023. Accessed June 24, 2023. http://www.ncbi.nlm.nih.gov/books/NBK564299/
2. Poonam NS, Alam MS, Oberoi P, Mukherjee B. Dysthyroid optic neuropathy: Demographics, risk factors, investigations, and management outcomes. Indian J Ophthalmol. 2022;70(12):4419-4426. doi:10.4103/ijo.IJO_719_22
3. Dolman PJ. Dysthyroid optic neuropathy: evaluation and management. J Endocrinol Invest. 2021;44(3):421-429. doi:10.1007/s40618-020-01361-y
4. Pelewicz-Sowa M, Miśkiewicz P. Dysthyroid optic neuropathy: emerging treatment strategies. J Endocrinol Invest. 2023;46(7):1305-1316. doi:10.1007/s40618-023-02036-0
5. Rutkowska-Hinc B, Maj E, Jabłońska A, Milczarek-Banach J, Bednarczuk T, Miśkiewicz P. Prevalence of Radiological Signs of Dysthyroid Optic Neuropathy in Magnetic Resonance Imaging in Patients with Active, Moderate-to-Severe, and Very Severe Graves Orbitopathy. Eur Thyroid J. 2018;7(2):88-94. doi:10.1159/000486828
6. Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43-G67. doi:10.1530/EJE-21-0479
7. Giaconi JA, Kazim M, Rho T, Pfaff C. CT scan evidence of dysthyroid optic neuropathy. Ophthalmic Plast Reconstr Surg. 2002;18(3):177-182. doi:10.1097/00002341-200205000-00005
8. Smith TJ. New advances in understanding thyroid-associated ophthalmopathy and the potential role for insulin-like growth factor-I receptor. F1000Res. 2018;7:134. doi:10.12688/f1000research.12787.1
9. Men CJ, Kossler AL, Wester ST. Updates on the understanding and management of thyroid eye disease. Ther Adv Ophthalmol. 2021;13:25158414211027760. doi:10.1177/25158414211027760
10. Kaichi Y, Tanitame K, Terada H, et al. Thyroid-associated Orbitopathy: Quantitative Evaluation of the Orbital Fat Volume and Edema Using IDEAL-FSE. Eur J Radiol Open. 2019;6:182-186. doi:10.1016/j.ejro.2019.05.003
Figures
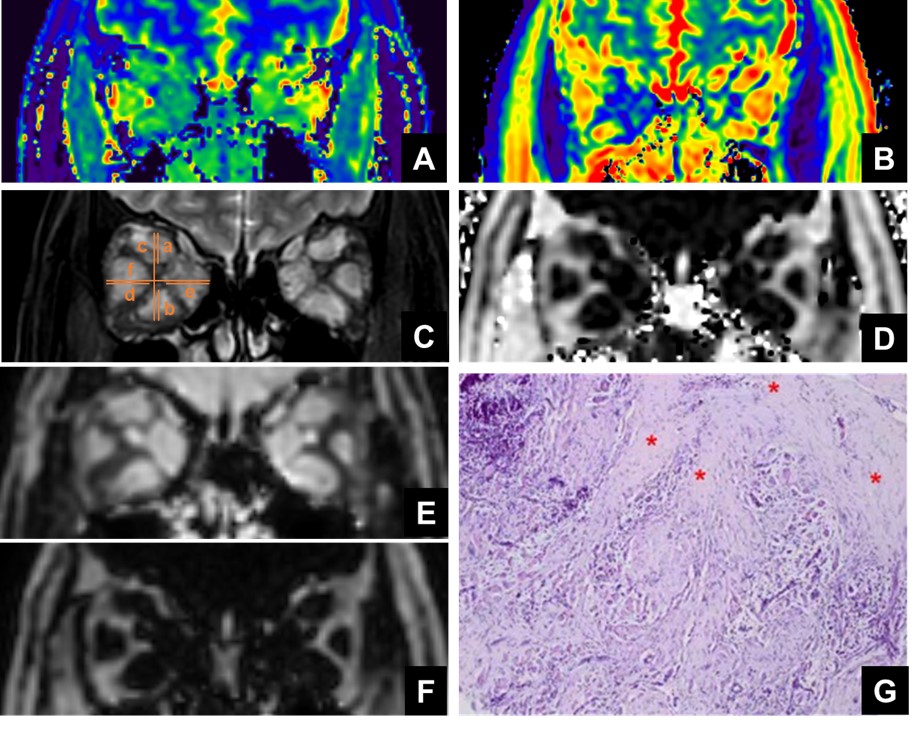
Figure 1: A 67-year-old female patient with DON. A, T1 mapping; B, T2mapping; C, Muscle index was identified as the bigger value of (a+b)/c and (d+e)/f for each eye in T2WI; D, Fat fraction; Water (E) and fat (F) phases of coronal plains were presented. G, H&E stain slice of EOM biopsy showed diffused fibrosis.
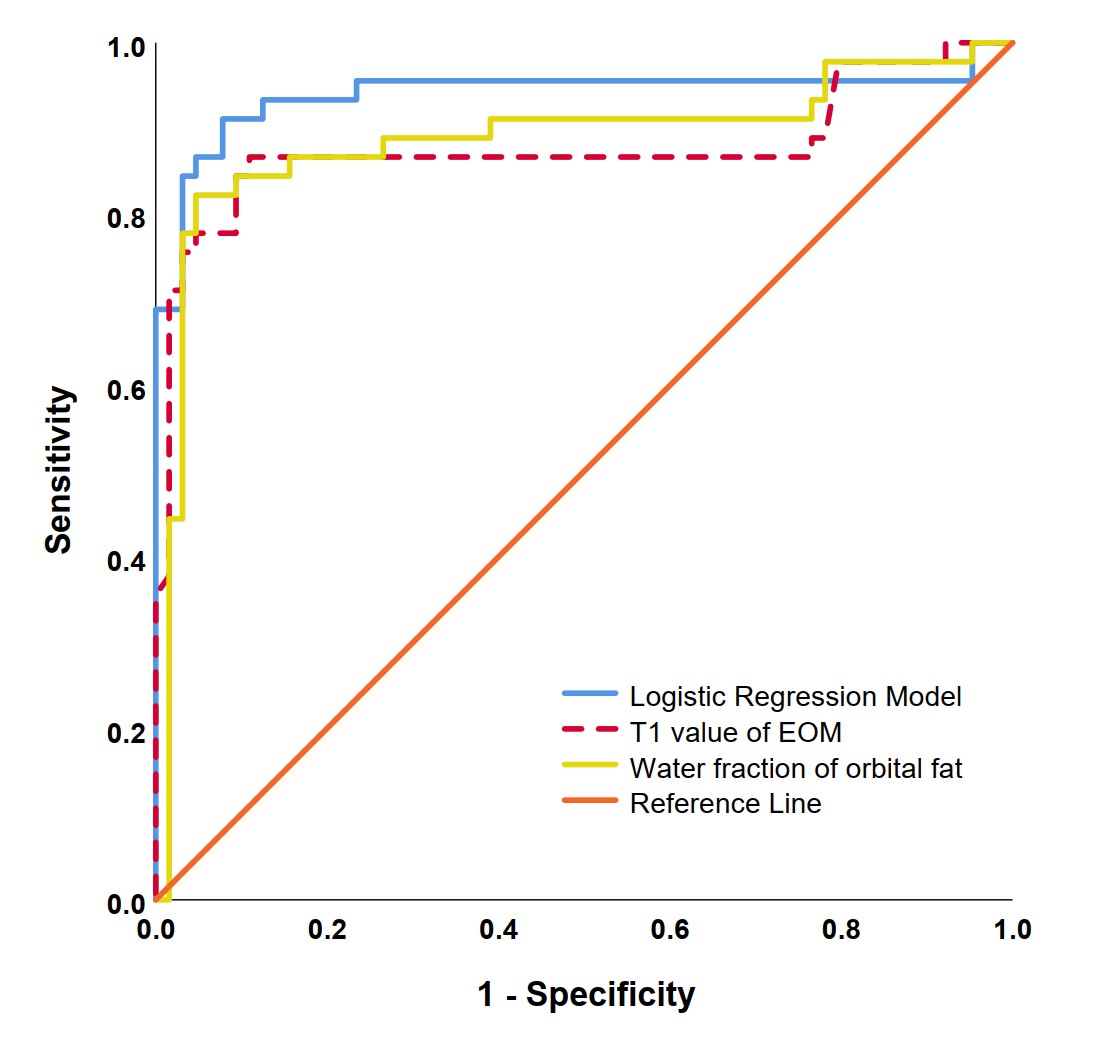
Figure 2. Receiver operating characteristic curves of T1 value of EOM, water fraction of orbital fat, and logistic regression model in distinguishing DON.