1934
CSF Flow Dynamics and Volume Changes in Sigmoid Sinus Wall Dehiscence-Pulsatile Tinnitus with Idiopathic Intracranial Hypertension1Beijing Tongren Hospital, Beijing, China, 2Clinical & Technical Support, Philips Healthcare, Beijing, China
Synopsis
Keywords: Head & Neck/ENT, Fat, Pulsatile tinnitus. Sigmoid sinus dehiscence. Intracranial hypertension. Cerebrospinal fluid dynamics. Cerebrospinal fluid volume.
Motivation: The mechanism of sigmoid sinus dehiscence (SSWD) in pulsatile tinnitus (PT) patients remains unclear.
Goal(s): To assess the cerebrospinal fluid (CSF) dynamics and volume of SSWD-PT with intracranial hypertension by phase-contrast magnetic resonance imaging (PC-MRI).
Approach: Thirty-five PT patients with SSWD and intracranial hypertension identified on dual-phase contrast-enhanced CT (DP-CECT) and brain magnetic resonance venogram (MRV), respectively. And 35 age-, gender-, and handiness-matched healthy volunteers. All participants underwent T1-weighted volumetric and PC-MRI.
Results: The body mass index, regurgitant fraction and CSF volume were significantly higher and the mean velocity, peak velocity and mean flux were significantly slower in SSWD-PT.
Impact: We found the CSF dynamics and volume changes in SSWD-PT with intracranial hypertension, which may be related to blood flow dynamics changes in sigmoid sinus and presence of PT. These results suggest treatment for SSWD-PT should be more comprehensive.
Introduction
Sigmoid sinus abnormalities (SSA), especially sigmoid sinus wall dehiscence (SSWD), is the most common treatable etiology of pulsatile tinnitus (PT) [1-6]. Recent studies have proposed that SSA-PT occurrence are closely related to intracranial hypertension [7-11] and dysregulation of CSF dynamics has been considered to be the key for intracranial pressure abnormality [12-16]. Unfortunately, the changes of CSF have not been illustrated in SSA-PT patients. Therefore, we will study CSF dynamics and volume of SSWD-PT patients with phase-contrast magnetic resonance imaging (PC-MRI).Methods
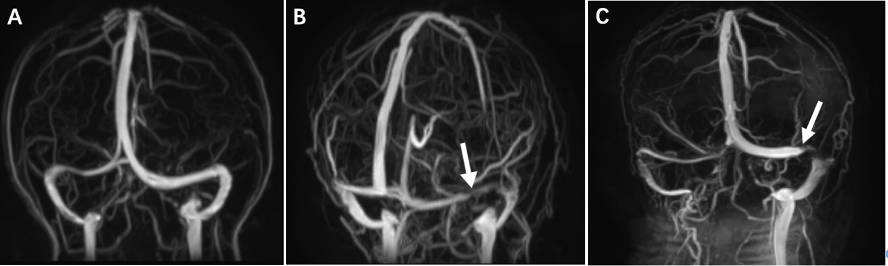
Thirty-five SSWD-PT patients with intracranial hypertension and 35 age-, gender-, and handiness-matched healthy volunteers underwent PC-MRI, brain magnetic resonance venogram (MRV), three-dimensional T1-weighted anatomical images on a Philips Ingenia 3.0 T MR scanner (Philips, Netherlands) and dual-phase contrast-enhanced CT (DP-CECT) on a 256-slice multi-detector CT (GE Heahhcare, USA).The DP-CECT parameters were: 200 mA, 80~140 kV, rotation time 0.5s, pitch 0.992, thickness 5mm, FOV=24×24 cm, matrix=512×512.The MRV parameters were: velocity encoding 15cm/s, TE=7.1ms, TR=17.9ms, flip angle=10°, FOV =23×23 cm, matrix=232×192. The three-dimensional T1-weighted anatomical images parameters were: TE=3.8ms, TR=8.3ms, flip angle=8°, FOV=24×24 cm, matrix=240×222, voxel size = 1 mm× 1 mm× 1 mm, thickness=1 mm, 170 slices. PC-MRI were located perpendicular to the midpoint of the midbrain aqueduct. The parameters were: TE=7.5ms, TR=12.6ms, flip angle =15°, FOV=15×15 cm, matrix=320×500, NSA=1, thickness=4 mm, PC velocity=12 cm/s.Intracranial pressure evaluation:The Index of transverse sinus stenosis (ITSS) method proposed by Carvalho was used to evaluate intracranial pressure on MRV [17]. An independent classification of right and left transverse sinus stenosis:0, normal; 1, stenosis <33%; 2,stenosis 33–66%; 3,stenosis >66%; 4, hypoplasia or agenesis. ITSS=degree of stenosis of the right transverse sinus × degree of stenosis of the left transverse sinus. When ITSS≥4, intracranial hypertension was considered, and when ITSS<4, the intracranial pressure was considered normal.
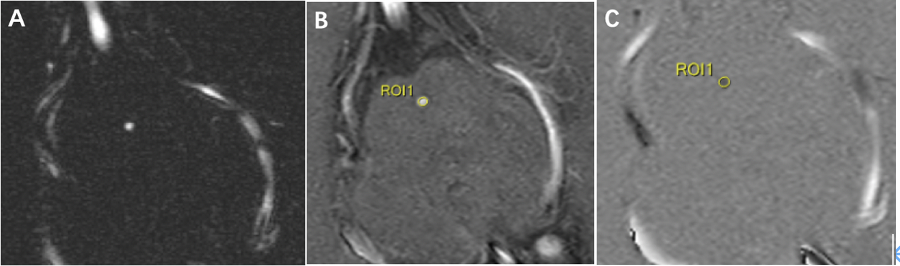
CSF flow dynamics:Through the PC-MRI, quantitative measurements of CSF flow at the level of the midbrain aqueduct were processed using the “Q Flow” software at the Intellispace Portal version 9.0 (Philips Healthcare, Best, Netherlands) and performed on phase images. The software automatically calculated the stroke volume (SV), forward flow volume (FFV), backward flow volume (BFV), regurgitant fraction (RF), mean flux (MF), stroke distance (SD), mean velocity (MV) and peak velocity (PV). The heart rate (HR) was also among the data presented by the software.
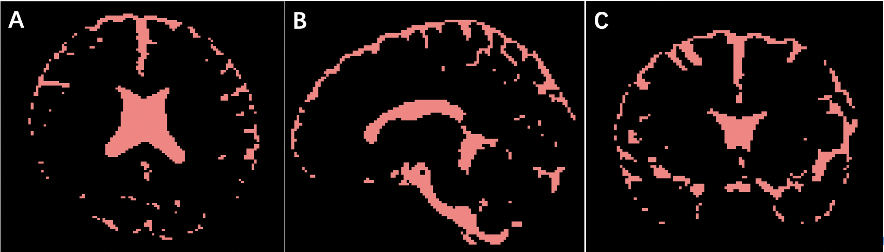
CSF volume:Measured on three-dimensional T1-weighted anatomical images by DPABI (http://rfmri.org/dpabi) and ITK-SNAP segmentation software (Cognitica, Philadelphia, PA, USA, http://www.itksnap.org). A probability greater than 0.5 was considered CSF.
Independent-samples t test or Mann-Whitney U test was used to analyze measurement data. The X2 test was used to analyze enumeration data.
Results
Compared with controls, BMI of PT patients was significantly higher than controls(P=0.046). The PV, MV and MF were significantly lower(P=0.023, 0.038, 0.017, respectively) and the RF and CSF volume were significantly higher(P=0.010, 0.024, respectively) in PT group. Other parameters were not significantly different.Discussion
This study evaluated the changes of CSF dynamics and volume in SSWD-PT with intracranial hypertension. Compared with controls, the CSF changes include significantly decreased PV, MV and MF and increased RF and CSF volume, which verified not only blood flow but also CSF associated with SSWD-PT occurrence.Karahalios and Sugerman thought that obesity would cause an increased in central venous pressure, resulting in reduced CSF reabsorption [18-19]. Furthermore, Tain reported reduced spinal/intracranial compliance in obese women with IIH. Reduced spinal canal compliance may result in a decreased ability to accommodate CSF volume within the spinal canal, which promotes the accumulation of CSF in the cranial compartment [20]. Therefore, the increased CSF volume maybe the result of a combination of absorption disorder and reduced spinal canal compliance.
The PV, MV and MF were significantly lower and the RF was significantly higher in PT patients, which may be due to the reduced compliance of the spinal canal.
According to our study, we suggest dynamics and volume of intracranial CSF changes owing to fat (increased BMI) give rise to intracranial hypertension, which lead to flow dynamics and morphology abnormalities of sigmoid sinus, ultimately occurrence of PT.
DPCT can obtain the arterial and venous phase images to find the cause of tinnitus. The ITSS diagnoses intracranial hypertension with a sensitivity and specificity of 94.7% and 93.5%, respectively [17].
Conclusions
The PV, MV and MF were significantly lower and the RF, and CSF volume were significantly higher in SSWD-PT with intracranial hypertension, which may be related to blood flow dynamics changes in sigmoid sinus and presence of PT. These results suggest treatment for SSWD-PT should be more comprehensive, not only focus on reconstruction of sigmoid plate dehiscence.Acknowledgements
The study was supported by National Natural Science Foundation of China (82071882) and Beijing Municipal Natural Science Foundation (7222029).References
[1]Eisenman DJ. Sinus wall reconstruction for sigmoid sinus diverticulum and dehiscence: a standardized surgical procedure for a range of radiographic findings. Otol Neurotol. 2011;32(7):1116-1119.
[2]Grewal AK, Kim HY, Comstock RH 3rd, et al. Clinical presentation and imaging findings in patients with pulsatile tinnitus and sigmoid sinus diverticulum/dehiscence. Otol Neurotol. 2014;35(1):16-21.
[3]Mattox DE, Hudgins P. Algorithm for evaluation of pulsatile tinnitus. Acta Otolaryngol. 2008;128(4):427-431.
[4]Geng W, Liu Z, Fan Z. CT characteristics of dehiscent sigmoid plates presenting as pulsatile tinnitus: a study of 23 patients. Acta Radiol. 2015;56(11):1404-1408.
[5]Wang GP, Zeng R, Liu ZH, et al. Clinical characteristics of pulsatile tinnitus caused by sigmoid sinus diverticulum and wall dehiscence: a study of 54 patients. Acta Otolaryngol. 2014;134(1):7-13.
[6]Schoeff S, Nicholas B, Mukherjee S, et al. Imaging prevalence of sigmoid sinus dehiscence among patients with and without pulsatile tinnitus. Otolaryngol Head Neck Surg. 2014;150(5):841-846.
[7]Eisenman DJ, Raghavan P, Hertzano R, et al. Evaluation and treatment of pulsatile tinnitus associated with sigmoid sinus wall anomalies. Laryngoscope. 2018;128 Suppl 2:S1-S13. doi:10.1002/lary.27218.
[8]Liu Z, Dong C, Wang X, et al. Association between idiopathic intracranial hypertension and sigmoid sinus dehiscence/diverticulum with pulsatile tinnitus: a retrospective imaging study. Neuroradiology. 2015;57(7):747-753. doi:10.1007/s00234-015-1517-5.
[9]Xu S, Ruan S, Liu S, et al. CTA/V detection of bilateral sigmoid sinus dehiscence and suspected idiopathic intracranial hypertension in unilateral pulsatile tinnitus. Neuroradiology. 2018;60(4):365-372. doi:10.1007/s00234-018-1987-3.
[10]Haraldsson H, Leach JR, Kao EI, et al. Reduced Jet Velocity in Venous Flow after CSF Drainage: Assessing Hemodynamic Causes of Pulsatile Tinnitus. AJNR Am J Neuroradiol. 2019;40(5):849-854.
[11]Boddu S, Dinkin M, Suurna M, et al. Resolution of Pulsatile Tinnitus after Venous Sinus Stenting in Patients with Idiopathic Intracranial Hypertension. PLoS One. 2016;11(10): e0164466. Published 2016 Oct 21.
[12]Donaldson JO. Pathogenesis of pseudotumor cerebri syndromes. Neurology. 1981;31(7):877-880. doi:10.1212/wnl.31.7.877.
[13]Donaldson JO. Cerebrospinal fluid hypersecretion in pseudotumor cerebri. Trans Am Neurol Assoc. 1979;104:196-198.
[14]Sørensen PS, Krogsaa B, Gjerris F. Clinical course and prognosis of pseudotumor cerebri. A prospective study of 24 patients. Acta Neurol Scand. 1988;77(2):164-172. doi:10.1111/j.1600-0404.1988.tb05888.x.
[15]Gjerris F, Børgesen SE. Current concepts of measurement of cerebrospinal fluid absorption and biomechanics of hydrocephalus. Adv Tech Stand Neurosurg. 1992;19:145-177. doi:10.1007/978-3-7091-6672-7_5.
[16]Gjerris F, Soelberg Sørensen P, Vorstrup S, et al. Intracranial pressure, conductance to cerebrospinal fluid outflow, and cerebral blood flow in patients with benign intracranial hypertension (pseudotumor cerebri). Ann Neurol. 1985;17(2):158-162. doi:10.1002/ana.410170209.
[17]Carvalho GB, Matas SL, Idagawa MH, et al. A new index for the assessment of transverse sinus stenosis for diagnosing idiopathic intracranial hypertension. J Neurointerv Surg. 2017;9(2):173-177.
[18]Karahalios DG, Rekate HL, Khayata MH, et al. Elevated intracranial venous pressure as a universal mechanism in pseudotumor cerebri of varying etiologies. Neurology. 1996;46(1):198-202.
[19]Sugerman HJ, DeMaria EJ, Felton WL 3rd, et al. Increased intra-abdominal pressure and cardiac filling pressures in obesity-associated pseudotumor cerebri. Neurology. 1997;49(2):507-511.
[20]Tain RW, Bagci AM, Lam BL, et al. Determination of cranio-spinal canal compliance distribution by MRI: Methodology and early application in idiopathic intracranial hypertension. J Magn Reson Imaging. 2011;34(6):1397-1404. doi:10.1002/jmri.22799.
Figures