1907
Partial Separable Model Combined with Spatial Constraint for Interventional MRI Reconstruction1Tsinghua University, Beijing, China
Synopsis
Keywords: Image Reconstruction, Simulations
Motivation: Real time interventional MRI (i-MRI) is essential for MR image guided therapy, but the requirement of high temporal resolution presents a great challenge for reconstruction of real-time i-MRI.
Goal(s): Our goal is modifying an improved Partial Separable (PS) model called PS-R model to explore the potential of the modified model to achieve real-time i-MRI.
Approach: We modified PS-R model with spatial constraint (PS-RSC) and performed retrospective experiments on simulation intervention MRI images to verify the effectiveness of the PS-RSC model.
Results: Satisfying results were obtained with only 7 k-space lines for reconstructing one frame, giving an acceleration up to 40 folds.
Impact: The reconstruction results of the simulation experiment showed that our method could obviously accelerate the acquisition time with good needle positioning, thus suggesting it has the potential for many MR guided interventional MRI application scenarios, such as MR image-guided therapy.
Introduction
Real-time interventional MRI (i-MRI) is essential for MR image-guided therapy since it could help visualize the interventional process and therefore improve the surgery performance and patient outcome1,2. However, the inherently slow acquisition time and the limitation of spatial and temporal resolution of dynamic MRI (dMRI) limits its application3. Different from k-t SPARSE SENSE model4 or L+S model5, partial separable (PS) model assumed MRI data has strong spatial-temporal correlations and could be decomposed into several basis functions6. An improved PS model called PS-R model fully exploited this prominent property to accelerate sampling speed7. Besides, dynamic images could be decomposed into static background which is low rank, and dynamic foreground which is high rank, therefore the location which is high rank in spatial basis could be used as prior information. Based on this, we modified PS-R model with spatial constraint to improve reconstruction performance and explored the potential of the modified PS model applied in interventional MRI application scenarios.Methods
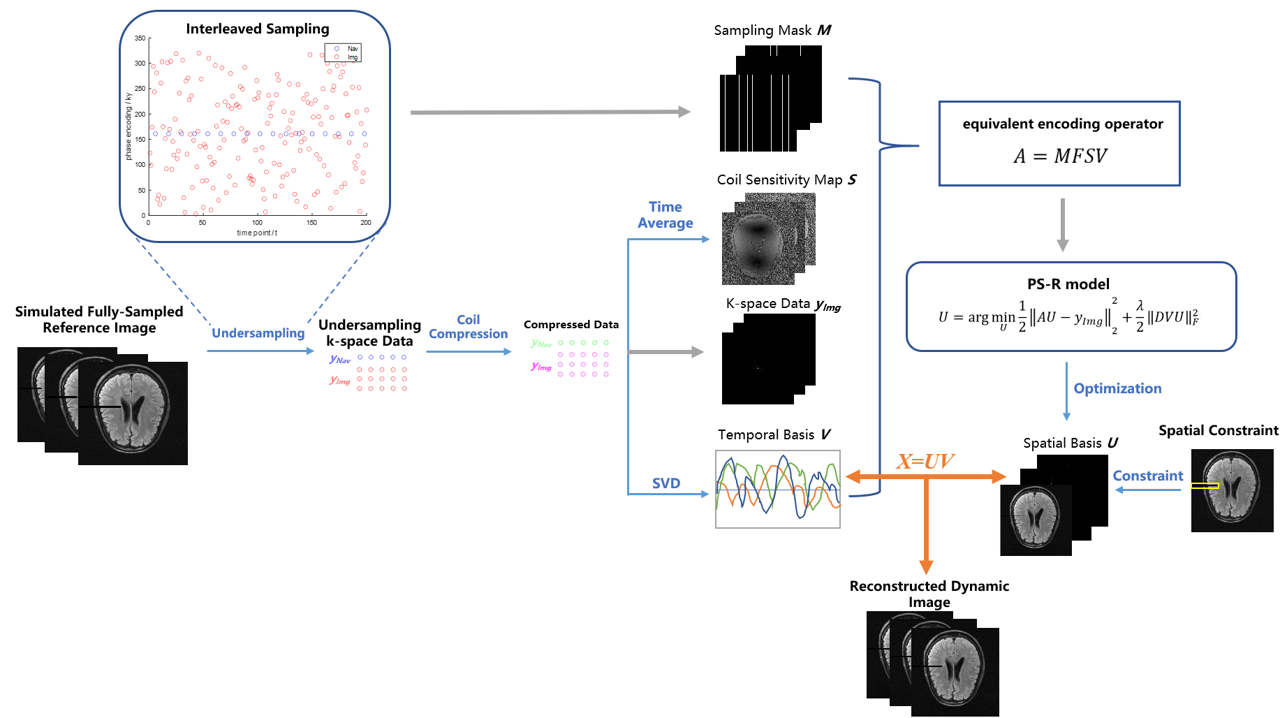
Model: We modified PS-R7 model with spatial constraint and used “PS-RSC model” to represent the modified model. The reconstruction problem formulation of PS-RSC model is the same as PS-R model. PS model assumes that the dynamic data can be decomposed into spatial basis function and temporal basis function. Therefore two datasets were sampled in an interleaved pattern. One is “Navigating data” yNAV samples center region of k-space to determine temporal basis, another is “Imaging data” yImg with extended k-space coverage to determine spatial basis 6,7. Our modification to PS-R model is adding extra spatial constraint. Since in our simulation experiments, simulated needle is dynamic while simulated brain is static, thus we assume that the location with high rank in spatial basis is where the needle located and could be useful prior information for reconstruction. Therefore we set zero to simulated needle locations to perform spatial constraint. Details are shown in Figure 1.Simulation of Brain Interventions: 320 brain intervention images were generated from reference brain MR images8. The reference image with a matrix size of 320×320 with 20 coil channels was used as Ground Truth of the experiment. We performed under-sampling in k-t space according to the interleaved sampling scheme to obtain undersampled raw data to be tested. We used Nkspc to represent the number of “Img data in k-space of one frame.
Comparison and Evaluation of Algorithms: The reconstruction results of PS-RSC model are compared with the PS-R model and another dynamic image reconstruction algorithm called k-t SPARSE SENSE. We calculated normalized mean square error (NMSE) and peak signal-to-noise ratio (PSNR) to quantitatively evaluate the performance models. The error map which represents the difference between reconstruction results and GT is shown as a visual comparison. Additionally, needle tip error was calculated, threshold segmentation and Hough transform were used to detect needle tip location on reconstructed images, and we can obtain the ground truth of needle tip location through simulation, thus tip error was the difference between them.
Results
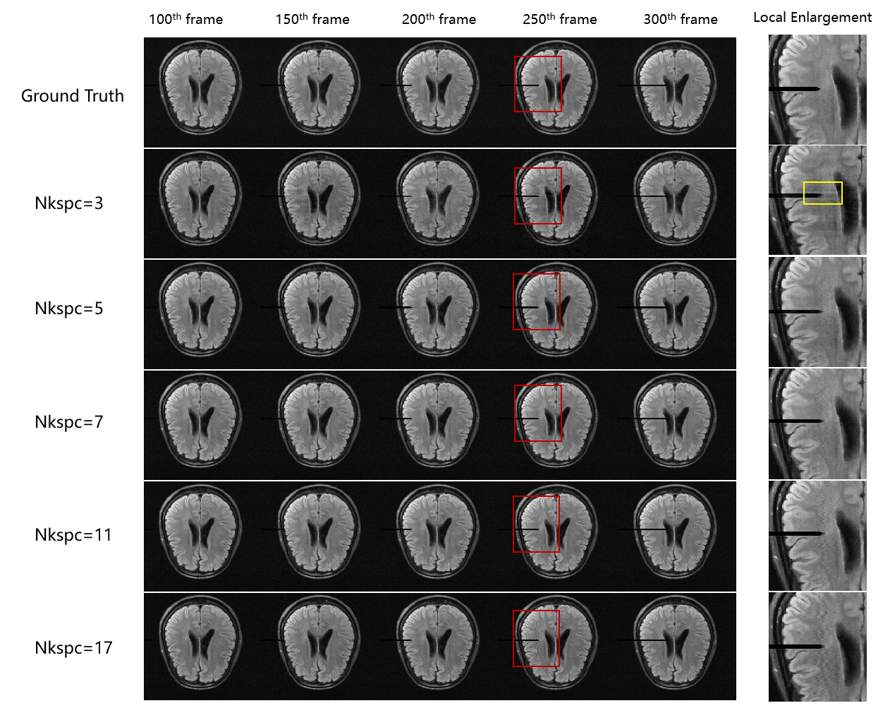
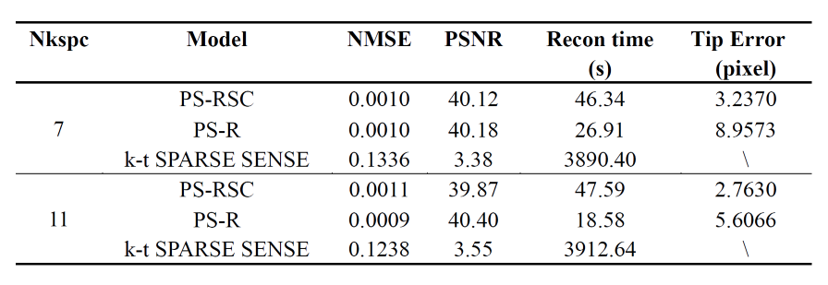
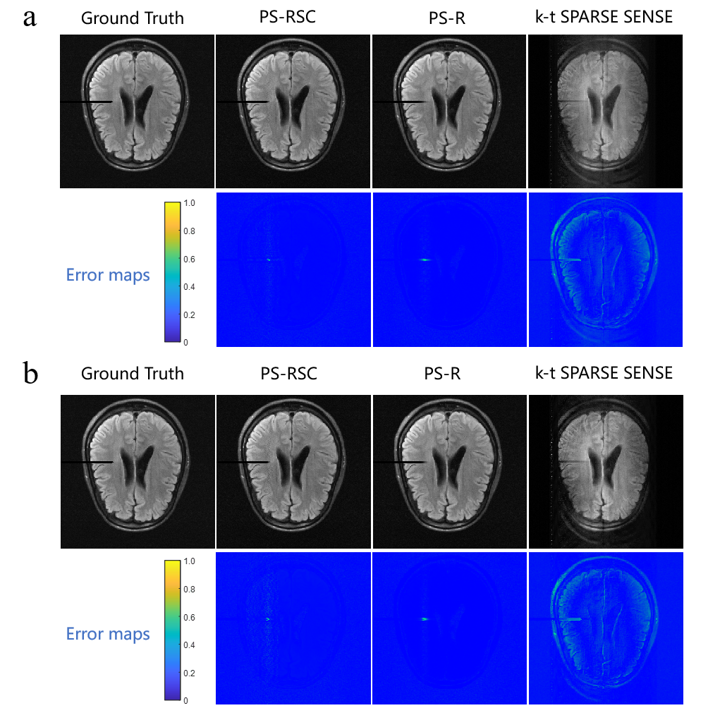
We first compared the reconstruction results with different Nkspc. When Nkspc is 3 or 17, the results were relatively poor, while the results were similar when Nkspc is 7 and 11(Table 1). Therefore, we fixed Nkspc to 7 or 11 for subsequent model comparison experiments. Five frames of GT and reconstruction results were selected to display the interventional process and visual comparison (Figure 2). Then we calculated NMSE, PSNR, reconstruction time, and tip error to demonstrate the effectiveness of the PS-RSC model and quantitatively compared it with k-t SPARSE SENSE and PS-R model (Table 2). Compared with k-t SPARSE SENSE, PS model spent less reconstruction time and obtained better performance, and PS-RSC model could track the intervention process more accurately than PS-R model. Finally, the 250th frame was selected to calculate error maps between GT and reconstruction results (Figure 3).Discussion and Conclusion
We modified PS-R model by adding spatial constraint and applied it in dynamic MRI image reconstruction for the first time to satisfy the higher temporal resolution of real-time interventional MRI. Satisfying results were obtained with only 7 k-space lines for reconstructing one frame, giving an acceleration up to 40 folds, which showed the great potential to achieve real-time i-MRI. It’s difficult for conventional dynamic reconstruction methods to obtain satisfactory results with such a high undersampling rate, and spatial constraint really improved the performance of PS-R model for dynamic MRI reconstruction. Future work includes considering other k-space trajectories, designing more generalized needle tip detection methods, and carrying out phantom and clinical animal experiments for exploring more effective and powerful reconstruction and evaluation methods in real-time i-MRI.Acknowledgements
No acknowledgement found.References
1. Zufiria B, Qiu S, Yan K, et al. A feature-based convolutional neural network for reconstruction of interventional MRI[J]. NMR in Biomedicine, 2022, 35(4): e4231.
2. Zhao R, He Z, Wang T, et al. A Long Short-term Memory Based Recurrent Neural Network for Interventional MRI Reconstruction[J]. arXiv preprint arXiv:2203.14769, 2022.
3. Ma S, Du H, Wu Q, et al. Dynamic MRI reconstruction exploiting partial separability and t-SVD[C]//2019 IEEE 7th International Conference on Bioinformatics and Computational Biology (ICBCB). IEEE, 2019: 179-184.
4. Otazo R, Kim D, Axel L, et al. Combination of compressed sensing and parallel imaging for highly accelerated first‐pass cardiac perfusion MRI[J]. Magnetic resonance in medicine, 2010, 64(3): 767-776. 5. Otazo R, Candes E, Sodickson D K. Low‐rank plus sparse matrix decomposition for accelerated dynamic MRI with separation of background and dynamic components[J]. Magnetic resonance in medicine, 2015, 73(3): 1125-1136.
6. Haldar J P, Liang Z P. Spatiotemporal imaging with partially separable functions: A matrix recovery approach[C]//2010 IEEE International Symposium on Biomedical Imaging: From Nano to Macro. IEEE, 2010: 716-719.
7. Li Z, Sun A, Liu C, et al. Accelerated partial separable model using dimension-reduced optimization technique for ultra-fast cardiac MRI[J]. Physics in Medicine & Biology, 2023, 68(10): 10NT01.
8. Zbontar J, Knoll F, Sriram A, et al. fastMRI: An open dataset and benchmarks for accelerated MRI[J]. arXiv preprint arXiv:1811.08839, 2018.
Figures