1901
Inline SNR-driven automatic quality control of UTE pulmonary imaging for patient-specific scan time adaptation1Laboratory of Imaging Technology, National Heart, Lung & Blood Institute, NIH, Bethesda, MD, United States, 2Siemens Healthcare Ltd., Calgary, AB, Canada
Synopsis
Keywords: Image Reconstruction, Low-Field MRI, MR value
Motivation: Image quality with fixed scan-duration is patient-dependent, leading to potentially insufficient quality for some patients and unnecessarily long scan time for others.
Goal(s): We propose inline automatic quality control based on signal-to-noise ratio (SNR) to efficiently achieve consistent diagnostic image quality for 3D pulmonary imaging.
Approach: We designed a closed-loop feedback framework between image reconstruction and data acquisition to automatically stop the acquisition when a target SNR is achieved. 6 healthy volunteers (HV) were imaged at 0.55T.
Results: Target SNR was achieved at 3mins 57s±1min 9s across the population.
Impact: The inline automatic quality control enables a subject-specific optimized scan time while ensuring sufficient data for highly resolved complex reconstruction. The distribution of early stopping times (1min 9s) across the population revealed the value of subject-specific scan time.
Introduction
We recently demonstrated a stack-of-spirals ultra-short echo time (UTE) method for high-resolution pulmonary imaging at 0.55T1 and improved its acquisition efficiently using an iterative concomitant field and motion-corrected reconstruction(iCoMoCo) reconstruction framework2. Nevertheless, image quality as measured by SNR was highly patient-dependent. It varied based on body habitus, irregular respiration. To improve the efficiency of our protocols and achieve consistent SNR across subjects, we propose an inline SNR-driven automatic quality control of UTE pulmonary imaging. Our method predicts the optimal subject-specific scan time, based on an early snapshot of image quality, to ensure consistent diagnostic image quality.Methods
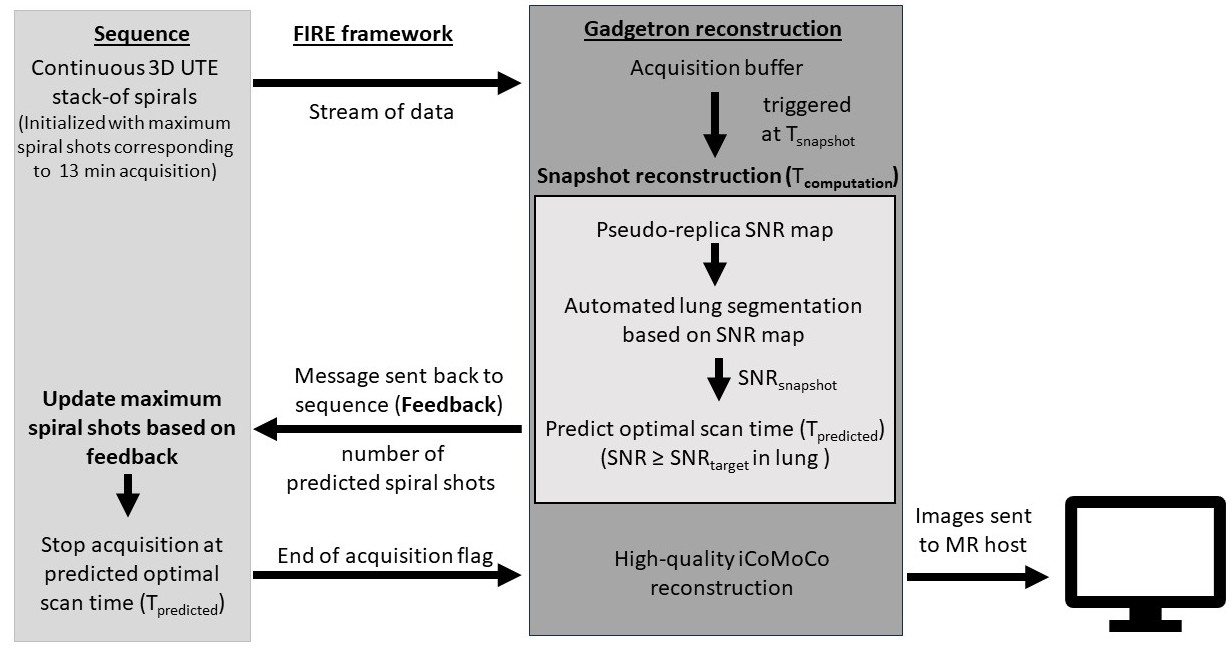
The inline SNR-driven automatic quality control was designed for minimal computational latency as follows(Figure 1). At an intermediate time after the start of imaging(Tsnapshot), a snapshot reconstruction was triggered, and an SNR map was estimated in Gadgetron3 using pseudo replica methods4. The SNR of the lung parenchyma(SNRsnapshot) was extracted automatically using a previously described segmentation method5. Based on this SNRsnapshot , the total optimal subject-specific scan duration (Tpredicted) needed to achieve the target SNR (SNRtarget) was calculated using this formula: $$T_{predicted}= T_{snapshot}* \left (\frac{SNR_{target}}{SNR_{snapshot}}\right )^{2} $$The predicted number of spiral shots corresponding to this duration(Tpredicted) is sent to the sequence controller via the “FIRE” research framework6 (Siemens Healthineers AG, Erlangen, Germany) and the acquisition is automatically stopped as soon as this number is reached.
At the end of the scan, data were retrospectively binned into 12 respiratory phases based on the superior-inferior(SI) navigator readouts and reconstructed using iterative concomitant field and motion corrected (iCoMoCo) reconstruction.
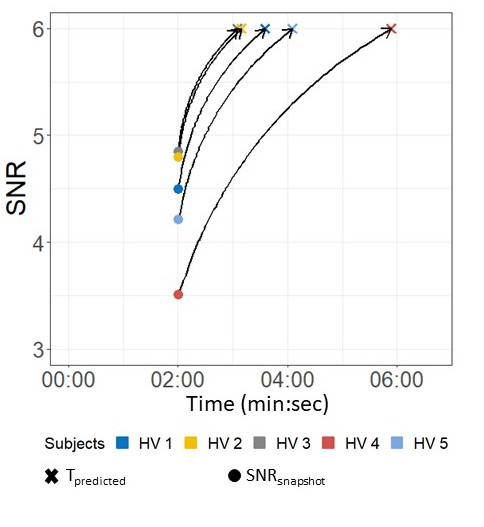
A retrospective analysis of five healthy volunteers(HV) (BMI=24.8±3.0, age=39±17 years old, male/female =2/3) assessed optimal scan time duration with a target mean lung SNRtarget=6 as the stopping criteria. Image acquisition used a prototype free-breathing golden angle stack-of-spirals 3D UTE spoiled gradient echo sequence (TE/TR=0.5/7.8ms, FA=4°, resolution=1.75mm3, FOV=450x450x224mm3, total acquisition time=8.5min) on a 0.55T MRI system (prototype MAGNETOM Aera, Siemens Healthineers AG, Erlangen, Germany). Healthy volunteer imaging was performed with IRB approval.
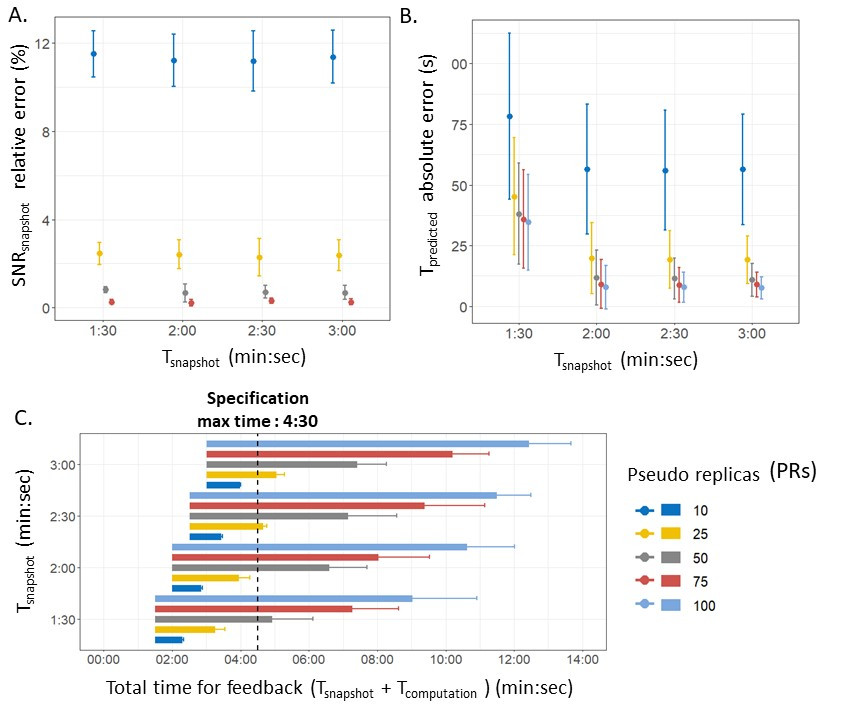
The 3D-UTE sequence generates large data sizes, and therefore computation time of the intermediate snapshot image must be considered. The choice of timing for the intermediate snapshot(Tsnapshot) and the number of pseudo replicas are constrained in order to keep sufficiently short computational time that feedback could be provided to the sequence, and the selection of these parameters can influence SNR accuracy. A range of snapshot times (Tsnapshot=1min30, 2min, 2min30, 3min) and number of pseudo replicas (PRs=10, 25, 50, 75, 100) were assessed retrospectively for feasibility of inline deployment.
One HV was prospectively imaged with a sequence which modifies the total number of spiral shots based on feedback from the SNRsnapshot. This imaging was performed on a commercial 0.55T MRI system (MAGNETOM Free.Max, Siemens Healthineers AG, Erlangen, Germany) with the following parameters (TE/TR=0.8/7.5ms, FA=5°, resolution=1.75mm3, FOV=480x480x190mm3). The acquisition was initialized with a maximum acquisition time of 13 minutes.
Results
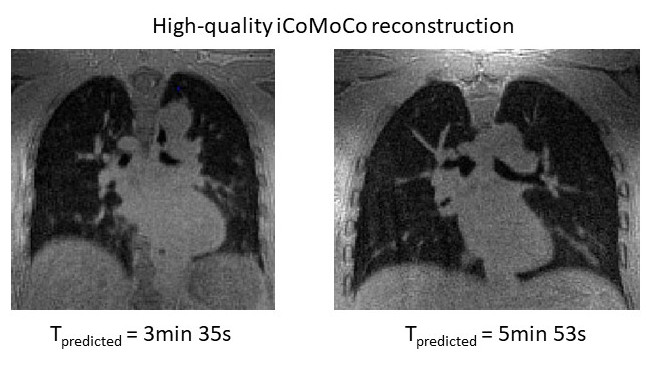
At least 25 PRs were required to obtain an SNRsnapshot relative error <5% (Figure 2). Tsnapshot≥2 min was also necessary to predict correctly (<25s) the optimal subject-specific scan duration (Tpredicted). Finally, because this quality control feedback will be applied inline, the computational time(Tcomputation) plus the acquisition time(Tsnapshot) must be less than the expected total duration of the scan (4min30). Only 1 set of parameters (Tsnapshot=2 min and PRs=25) met all the criteria. Retrospective analysis using these selected parameters demonstrated that the SNRtarget was achieved at 3min57s with a standard deviation of 1min9s across the population (Figure 3,4). Tcomputation required 1min56s±19s. In the subject where the automated stop was deployed prospectively(Figure 5), we used a reduced SNRtarget of 3 because imaging was performed on a different MRI system and sequence implementation. The SNRsnaphot at 2 min was 1.65, leading to a Tpredicted=6min17s and stopped the acquisition at the same time, with a final SNR=3.01 calculated from the unbinned images. The image quality was compared to the full 13min acquisition.Discussion
We demonstrated a framework for inline quality control and applied it for SNR-driven imaging. This workflow can improve imaging efficiency by reducing scan time in patients with good image quality and avoiding unnecessary scan repetition in patients with sub-optimal image quality. The variability of predicted early stopping times (standard deviation 1min9s) across the population from the retrospective analysis revealed the value of subject-specific acquisition time for consistent image quality. A limitation of inline quality control is the computation time(Figure 2.C) that limits the accuracy of SNRsnapshot estimation and total scan time prediction(Tpredicted).Conclusion
Our proposed SNR-driven inline quality control enables a subject-specific optimized scan time for pulmonary imaging while ensuring consistent diagnostic image quality.Acknowledgements
This work was supported by the National Heart, Lung, and Blood Institute (NHLBI) Division of Intramural Research (Z01-HL006257, Z01-HL006213). The authors are investigators on a US Government Cooperative Research and Development Agreement (CRADA) with Siemens Healthcare to develop 0.55T MRI.References
1. Javed A, Ramasawmy R, O’Brien K, et al. Self‐gated 3D stack‐of‐spirals UTE pulmonary imaging at 0.55T. Magn Reson Med. 2022;87(4):1784-1798. doi:10.1002/mrm.29079
2. Javed A, Ramasawmy R, Moss J, et al. Improved 3D stack-of-spiral UTE pulmonary imaging at 0.55T using iterative concomitant field and motion corrected reconstruction (iCoMoCo). In: ISMRM-ESMRMB & ISMRMT 31st Annual Meeting, 07-12 May. 2022 ISMRM-ESMRMB & ISMRT 31st Annual Meeting, 07-12 May. London, UK; 2022.
3. Hansen MS, Sørensen TS. Gadgetron: An open source framework for medical image reconstruction: Gadgetron. Magn Reson Med. 2013;69(6):1768-1776. doi:10.1002/mrm.24389
4. Robson PM, Grant AK, Madhuranthakam AJ, Lattanzi R, Sodickson DK, McKenzie CA. Comprehensive quantification of signal-to-noise ratio and g -factor for image-based and k -space-based parallel imaging reconstructions. Magn Reson Med. 2008;60(4):895-907. doi:10.1002/mrm.21728
5. Seemann F, Javed A, Chae R, et al. Imaging gravity-induced lung water redistribution with automated inline processing at 0.55 T cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2022;24(1):35. doi:10.1186/s12968-022-00862-4
6. Chow K, Kellman P, Xue H. Prototyping Image Reconstruction and Analysis with FIRE. In: SCMR. Virtual Scientific Sessions. ; 2021:838972.
Figures