1899
Evaluation of Facial Nerve Imaging using CRANI for Parotid Gland Mass: Preliminary Experience.1Radiology, Manipal Hospital, Bengaluru, India, 2Philips India Limited, Bengaluru, India, 3Philips India Limited, Gurgaon, India
Synopsis
Keywords: Head & Neck/ENT, Neurography, CRANI (CRanial Nerve Imaging), Parotid Mass
Motivation: Restricted visualization of the extra foraminal facial nerve inhibits pre-operative decision-making in parotid gland mass regarding nerve preservation.
Goal(s): Using 3D CRANI (CRanial Nerve Imaging) MR sequence, extra foraminal facial nerve was studied, focusing its anatomical relationship to parotid gland mass.
Approach: In 10 patients, post-contrast CRANI sequence was obtained in 3T scanner with 32-ch coil and Compressed SENSE imaging to study its extraforaminal course. Multi-planar and maximum-intensity projections was generated to enhance visibility.
Results: Extraforaminal segments of the facial nerve was well visualized up to its bifurcation. However, the visualization of branches distal to bifurcation in relation to the lesion was poor.
Impact: Extraforaminal facial nerve and its relationship to parotid mass allows surgeons to make better preoperative assessments. CRANI sequence effectively enables proximal nerve tracking while lacks in distal branch visualization in presence of mass; an avenue for future refinements.
INTRODUCTION
The intracranial portions of the cranial nerves are visualised using heavily T2-weighted 3D imaging; however, visualising the extracranial nerves remains difficult due to their small diameters, tortuous courses, susceptibility artefacts, and blood vessels, all of which can confound nerve visualisation. Newly developed Post-contrast 3D CRANI (CRAnial Nerve Imaging) by Casselman et al. demonstrated that it can adequately suppress signals from surrounding blood vessels and fat, enabling better visualisation of extra foraminal cranial nerves 1,2. Previously, restricted visualisation of the facial nerve inhibited surgical pre-operative decision-making about whether to preserve the nerve and its function versus total enucleation 3. In this study, 3D CRANI was tested in its clinical application to view the extraforaminal facial nerve and its branches, particularly in relation to parotid gland masses.METHODS
A post-contrast CRANI (3D STIR TSE sequence in combination with MSDE / Motion Sensitised Driven Equilibrium pulses) was implemented in a 3T scanner (Ingenia, Philips, The Netherlands) with a 32-ch head coil to evaluate the extraforaminal course of the facial nerve in a total of 10 cases: 8 associated with parotid mass lesions, 1 with lymphomatous involvement of the nerve, and 1 with facial neuritis. Imaging parameters for the CRANI sequence are presented in Table 1.| Sequences | TR/TE | FOV | Voxel Size | Compressed SENSE | Number of slices | TSE factor | NSA | Scan time |
| 3D CRANI | 2300/188 | 200*114 | 0.8*0.8*0.8 | 3.5 | 255 | 43 | 1 | 8min, 21s |
The facial nerve was visualized and evaluated with multiplanar reformations and maximum intensity projections of post-gadolinium CRANI images with suitable thickness and an overlapping slice gap.
Two radiologists and a neuro-radiologist with varied durations of experience, ranging from three to thirty years, reviewed the CRANI images and reached a consensus.
RESULTS
The extraforaminal vertical segment of the facial nerve was well visualized in all cases (10/10); its bifurcation or one of divisions in most cases (9/10), demonstrating its relationship with the parotid mass. In a case of lymphoma, the extent of lymphomatous involvement of the extraforaminal portions of both facial nerves was well visualized, which was seen as focal, segmental thickening as compared to diffuse, uniform thickening of the nerve seen in a case of facial neuritis, i.e., Bell's palsy. The visualization and tracing of distal branches of the facial nerve after its bifurcation in relation to the parotid mass was, however, poor (3/10).| Part of Facial nerve imaged with CRANI | Imaging Outcome |
| Vertical proximal segment | Visualised in all 10 cases |
| Bifurcation / one of the branches | Visualised in 9/10 cases |
| Distal branches (at least one) | Visualised in 3/10 cases only |
DISCUSSION AND CONCLUSION
3D CRANI enables dedicated extraforaminal imaging of the cranial nerves by uniformly suppressing signals from fat, muscle, and blood. 32-channel head coil and 3T MRI provide the high SNR required to visualize these small suprahyoid portions of cranial nerves. Further Compressed SENSE and contrast administration has helped minimize any movement-related image quality degradation and enhanced background suppression respectively.The most critical part of any parotid surgery is finding the facial nerve (CN VII), which controls the movement of half of the face. The plane at which the facial nerve divides the parotid gland is used to delineate the superficial and deep lobes of the gland. This study illustrates the ability of this unique MR neurography sequence to create nerve-selective imaging and detail the relationship of the facial nerve in parotid pathologies within clinically reasonable acquisition times. This knowledge would enable surgeons to choose and perform extracapsular parotid dissections over superficial parotidectomies, significantly enhancing facial nerve preservation and function in selected cases.
However, visualization and tracing of distal branches of the facial nerve after its bifurcation in relation to the parotid mass was poor. This is partly likely due to the inherent bright signals of most parotid mass on T2 STIR sequence, especially if lesion is cystic. The parotid gland substance, which is inherently rich with lymphatics and ductules, likely further reduces nerve visualization. On the contrary, when the primary disease process involves a nerve substance per se, such as in the case of lymphoma or neuritis, the sequence results in excellent visualization and tracing of the affected nerve. The pattern of involvement further aids in identifying the primary pathology involving the nerve, such as diffuse uniform thickening seen with neuritis and focal segmental thickening seen with lymphoma.
This ongoing study presents preliminary work highlighting the utility of the promising neurography sequence in the evaluation of facial nerves, discussing its challenges and limitations, and providing scope for further research.
Acknowledgements
No acknowledgement found.References
- Van der Cruyssen F, Croonenborghs T-M, Hermans R, Jacobs R, Casselman J. 3D cranial nerve imaging, a novel MR neurography technique using black-blood STIR TSE with a pseudo steady-state sweep and motion-sensitized driven equilibrium pulse for the visualization of the extraforaminal cranial nerve branches. AJNR Am J Neuroradiol [Internet]. 2021;42(3):578–80.
- Casselman J, Van der Cruyssen F, Vanhove F, Peeters R, Hermans R, Politis C, et al. 3D CRANI, a novel MR neurography sequence, can reliably visualise the extraforaminal cranial and occipital nerves. Eur Radiol [Internet]. 2022;33(4):2861–70.
- Kato MG, Erkul E, Nguyen SA, Day TA, Hornig JD, Lentsch EJ, et al. Extracapsular dissection vs superficial parotidectomy of benign parotid lesions: Surgical outcomes and cost-effectiveness analysis. JAMA Otolaryngol Head Neck Surg [Internet]. 2017;143(11):1092.
Figures
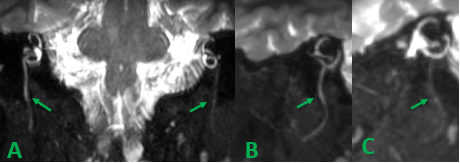
A. Coronal post-contrast 3D CRANI of a patient with right facial neuritis demonstrates diffuse uniform thickening of the right extraforaminal facial nerve (long arrow) compared to the normal nerve on the left (short arrow).
B. Sagittal post-contrast 3D CRANI demonstrates diffuse thickening of the right facial nerve (arrow).
C. Sagittal post-contrast 3D CRANI demonstrates normal caliber of the left facial nerve (arrow).
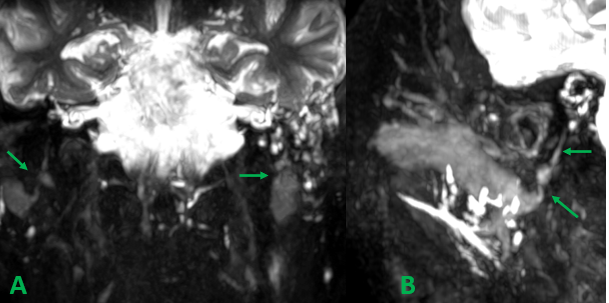
A. Coronal post-contrast 3D CRANI of a patient with lymphoma shows bilateral focal segmental thickening (arrows).
B. On sagittal post contrast 3D CRANI, it is observed to affect the buccal branch of the facial nerve (slanting arrow).
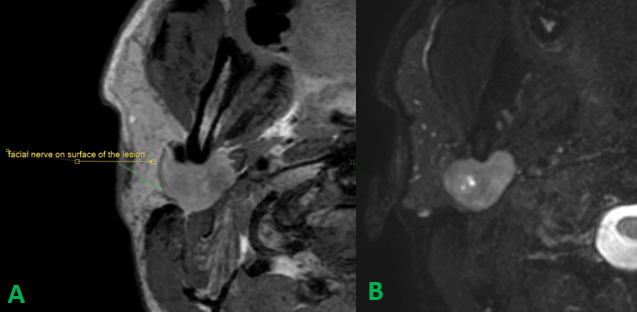
A. Axial post contrast T1 sequence without fat saturation of a patient with right parotid mass lesion shows the facial nerve coursing on the surface of the lesion (arrow).
B. In axial post-contrast 3D CRANI, the corresponding facial nerve segment could not be visualized.
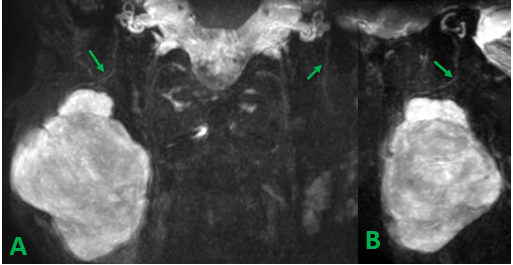
A. Lateral displacement of a division of the facial nerve is clearly seen on the coronal post-contrast 3D CRANI sequence of a patient with a right parotid mass (long arrow). The normal course of left facial nerve is also visualized (short arrow)
B. Sagittal reconstruction shows an additional cranial displacement (arrow) of the anterior division of the facial nerve.
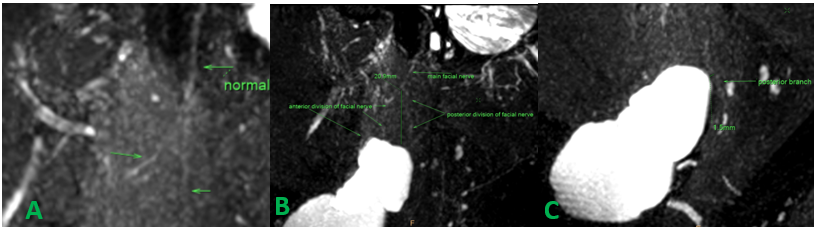
A. A magnified sagittal post-contrast 3D CRANI sequence slice depicts the proximal vertical segment of the facial nerve (arrow on top) dividing into anterior and posterior divisions distally (arrows below) on the normal, unaffected side.
B. Sagittal post-contrast sections on the contralateral side show a close relationship between the facial nerve divisions and the parotid gland mass lesion, with limited splaying at its bifurcation.
C. A magnified image of the similar sagittal section demonstrates posterior displacement of the facial nerve's posterior division (arrow).