1896
Visualizing the Vagus Nerve in Cadavers with High-Resolution MRI1Radiology, Case Western Reserve University and University Hospitals Cleveland Medical Center, Cleveland, OH, United States, 2Biomedical Engineering, Case Western Reserve University, Cleveland, OH, United States, 3Anatomy, Case Western Reserve University, Cleveland, OH, United States, 4Biomedical Engineering, Duke University, Durham, NC, United States, 5Pediatrics, Case Western Reserve University, Cleveland, OH, United States, 6L. Stokes Cleveland VA Medical Center, Cleveland, OH, United States
Synopsis
Keywords: Peripheral Nerves, Neurography, Nervous System, cadaveric MRI, vagus nerve
Motivation: Clinical visualization of the vagus nerve is challenging due to nerve diameter and tortuosity, as well as variation between subjects, making implementation of stimulation therapies difficult.
Goal(s): Determine feasibility of bilateral vagus visualization in embalmed cadavers using high-resolution imaging.
Approach: Thirteen cadavers were imaged at 0.5-0.6 mm isotropic resolution using 3D constructive interference in steady state (CISS) and volumetric interpolated breath-hold sequence (VIBE). Scanning covered the extent of the vagus from the skull base to the abdomen and imaging was correlated to gross dissection.
Results: The vagus nerve was visualized bilaterally most clearly with CISS and 0.5mm uninterpolated spatial resolution.
Impact: MRI visualization of the vagus, cranial nerve X, could be used to direct future interventions including potential percutaneous MRI-guided procedures. Cadaveric imaging can help optimize acquisitions for future in vivo translation.
Introduction
The vagus nerve, Cranial Nerve X, connects parasympathetic sensory and motor fibers to the heart, lungs and digestive tract and is the longest nerve of the autonomic system. The vagus has complex anatomy, and is difficult to visualize due to its nerve diameter (<5mm at origin), multiplicity of branching points, and formation of a plexus.The vagus is the target of intervention consisting of stimulation by controlled electrical currents.1,2 However, actual visualization of the vagus in standard clinical imaging is challenging due to the natively small diameter of the nerve, its tortuosity, as well as its unkown variability in trajectory across subjects.
We explore the feasibility of imaging the vagus nerve from the jugular foramen to the abdomen in cadavers and aim to develop optimized protocols that will be clinically translatable. The resultant scans will enable characterization of vagus nerve path, including considerations for surgical accessibility for new stimulation targets and surrounding tissues that affect the distribution of the electric field.
Methods
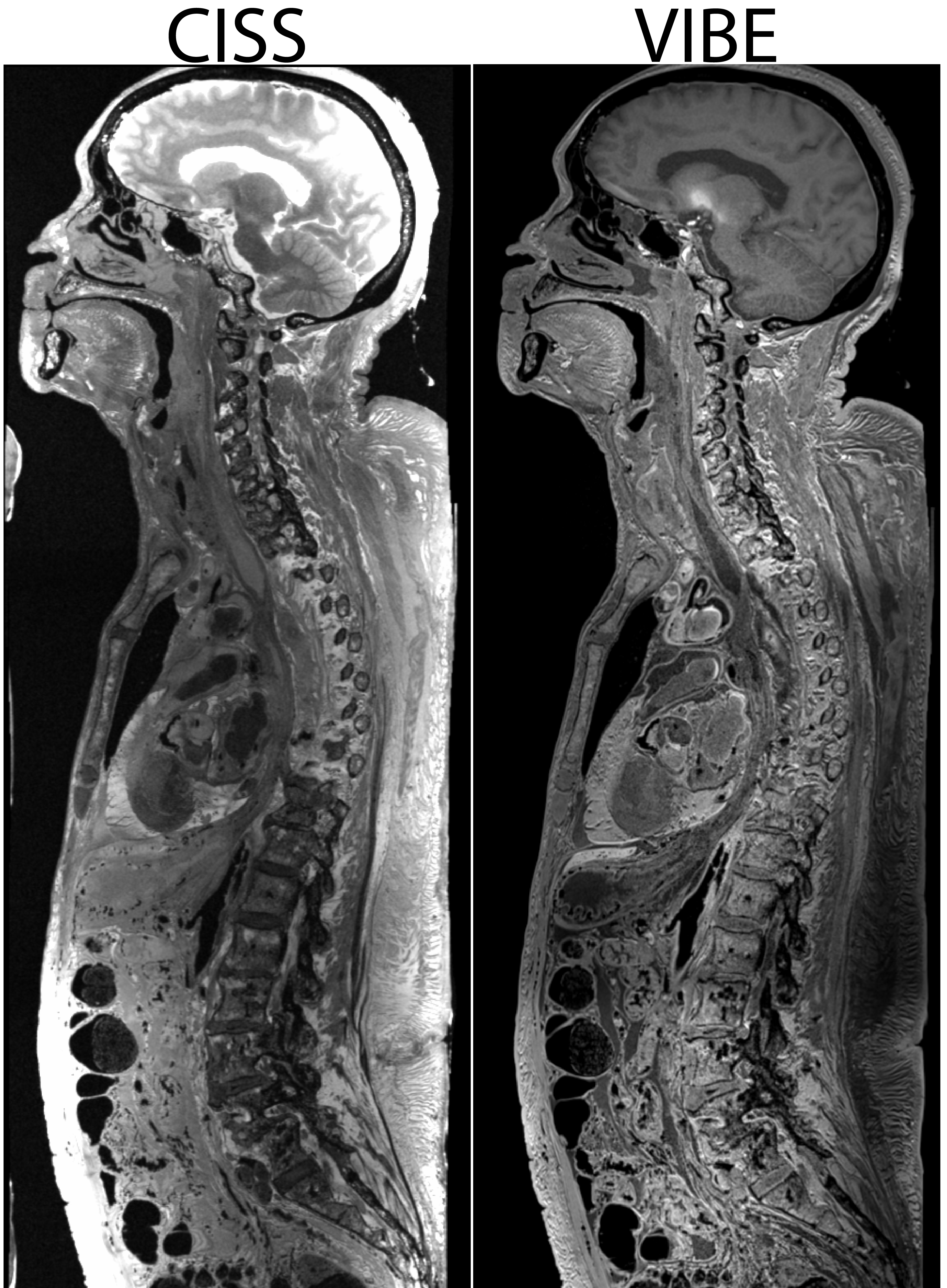
Cadavers were screened for existing implants with potential effects on imaging field of view.[NP1] Thirteen preserved cadavers were imaged using a 3T system (Vida, Siemens Healthineers) with maximum gradient strength of 60 mT/m. Data acquisition used a 20-channel head and neck coil and one or two torso coils.For nerve visualization, two 3D imaging pulse sequences were modified to enable larger coverage and higher resolution: (1) constructive interference in steady state (CISS) which is T2/T1-weighted and exhibits high signal-to-noise ratio efficiency and bright fat and fluids; and (2) volumetric interpolated breath-hold sequence (VIBE) which is a T1-weighted spoiled gradient echo acquisition. Both these techniques have been successful at visualizing neural structures.3-6
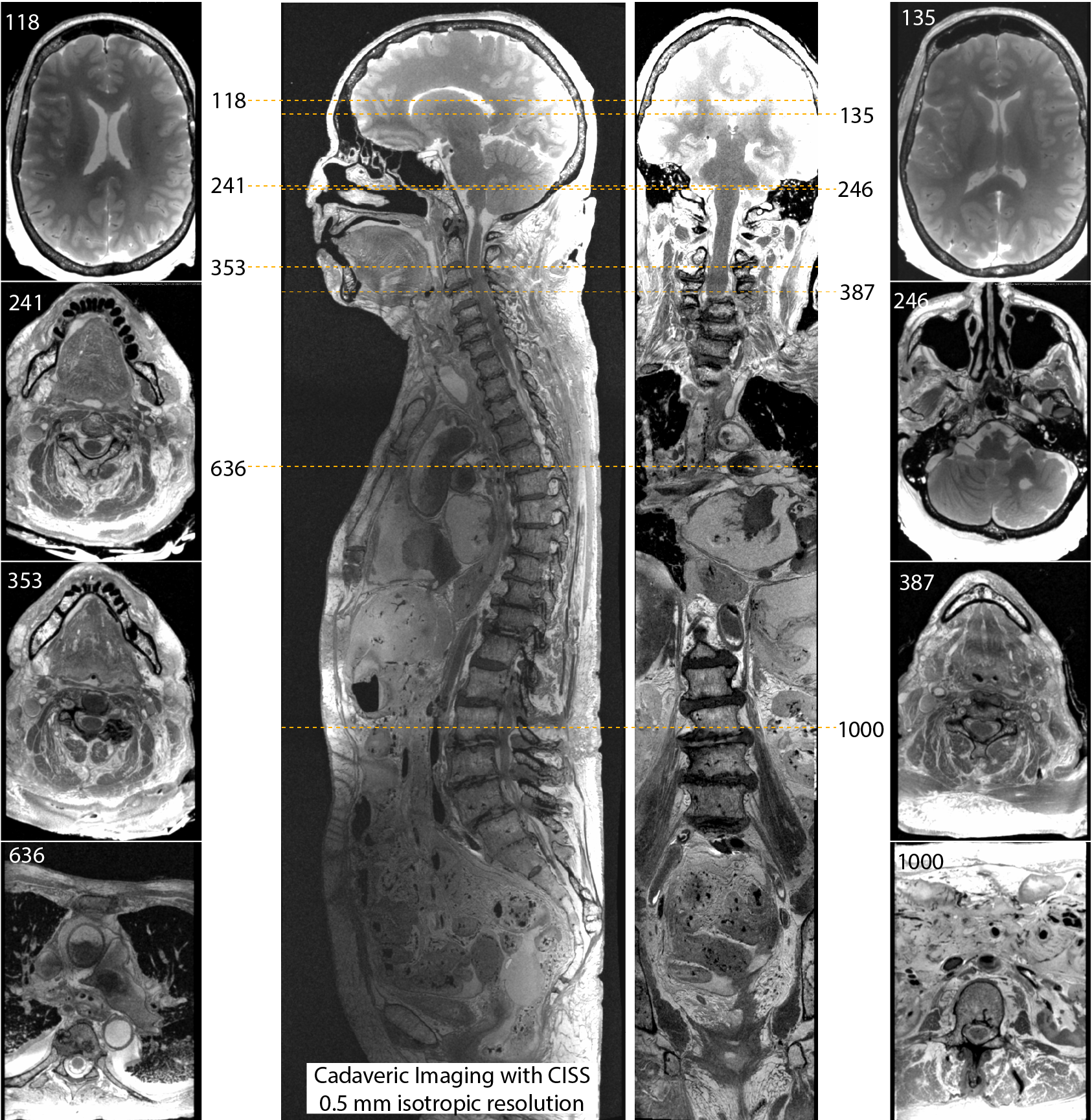
The CISS and VIBE scans were acquired in sagittal orientation with 12.5 cm coverage in the left-right dimension and variable phase encoding field of view sufficient to prevent foldover. The readout matrix was 640 using a 600 and 230 Hz/pixel receiver bandwidth for CISS and VIBE, respectively, with an elliptical window and no interpolation. Multiple imaging slabs with ~20% overlap were acquired sequentially and the resulting images were merged automatically.
MRI-derived vagal anatomy was correlated with gross dissection and 3D registration.
Results
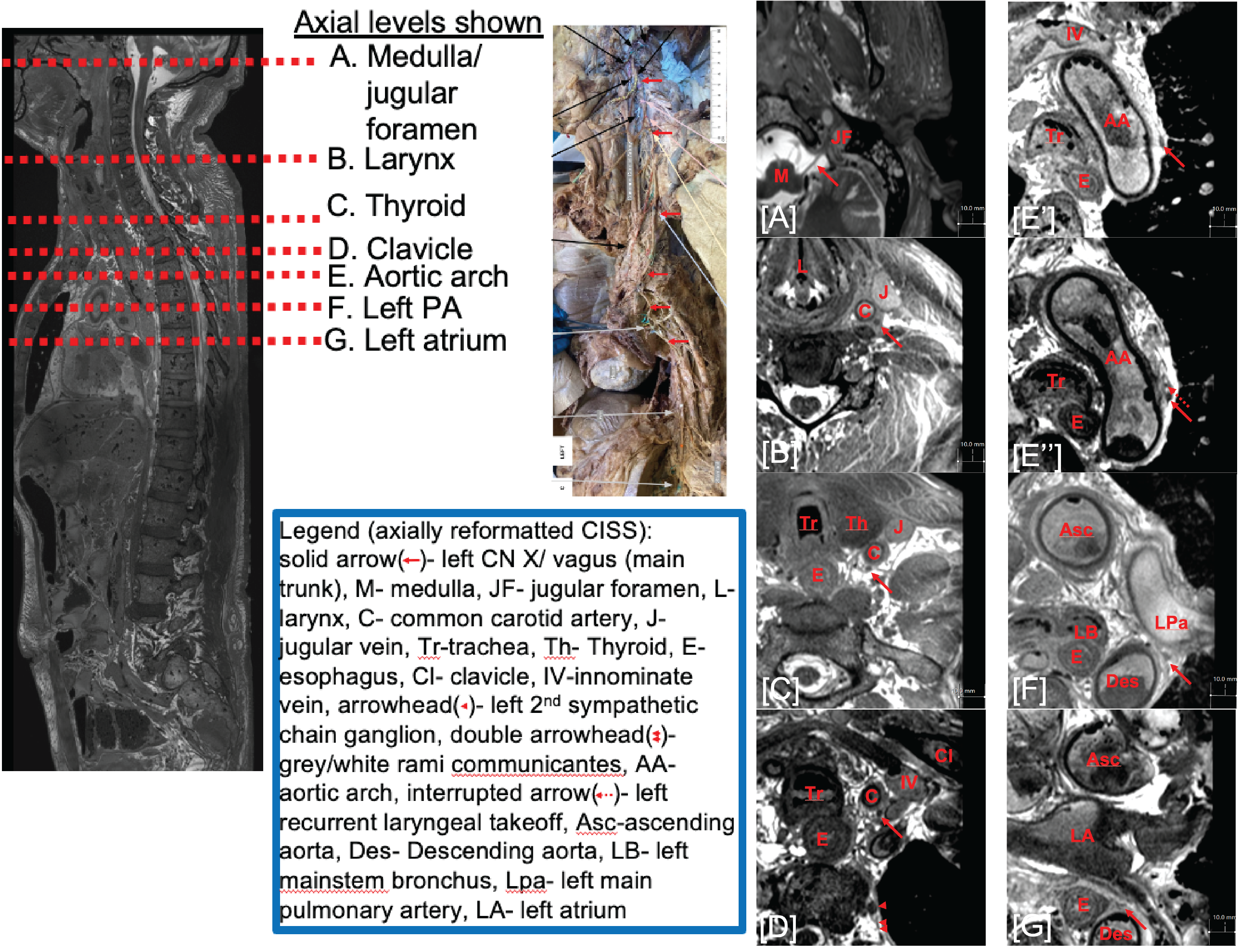
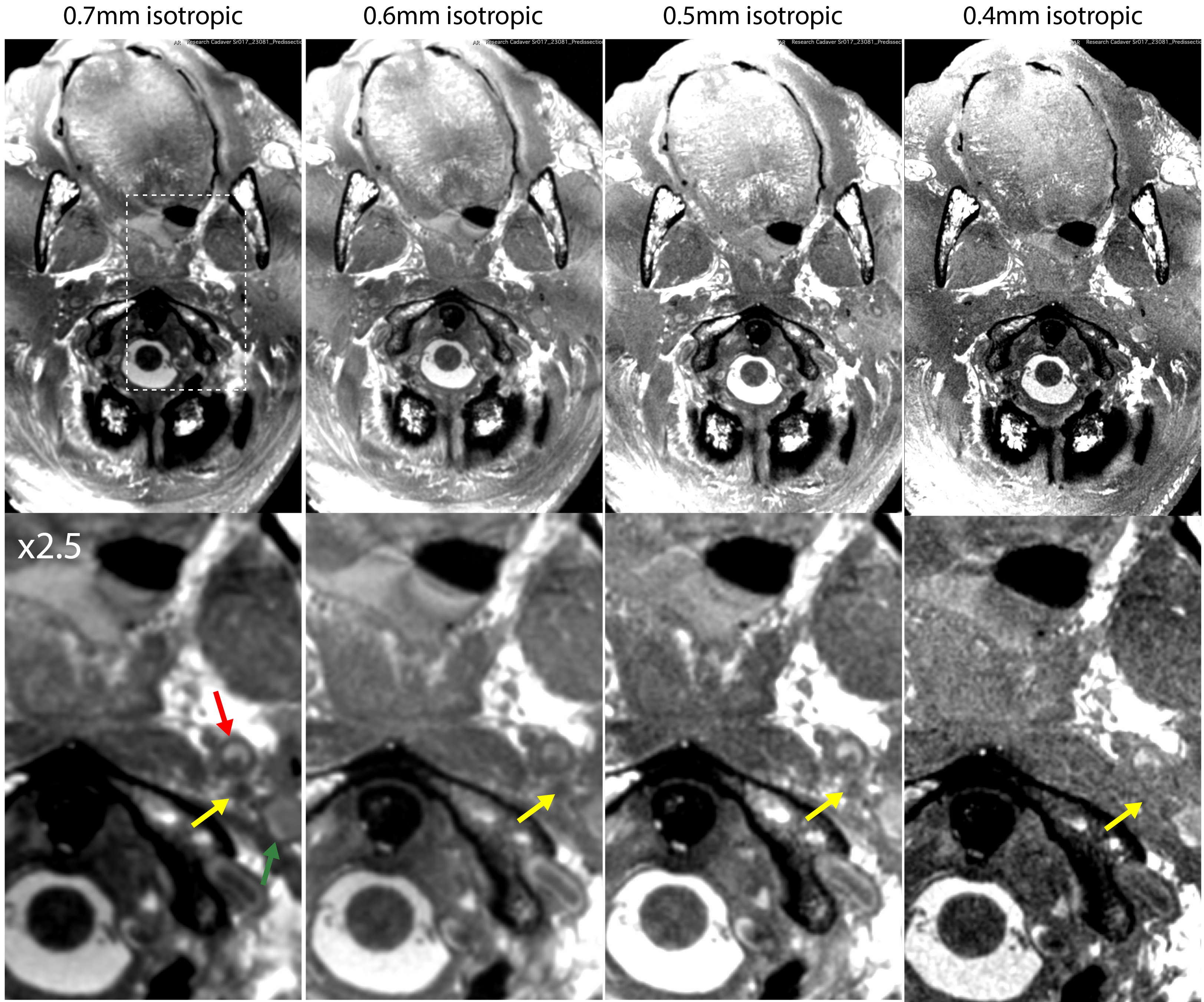
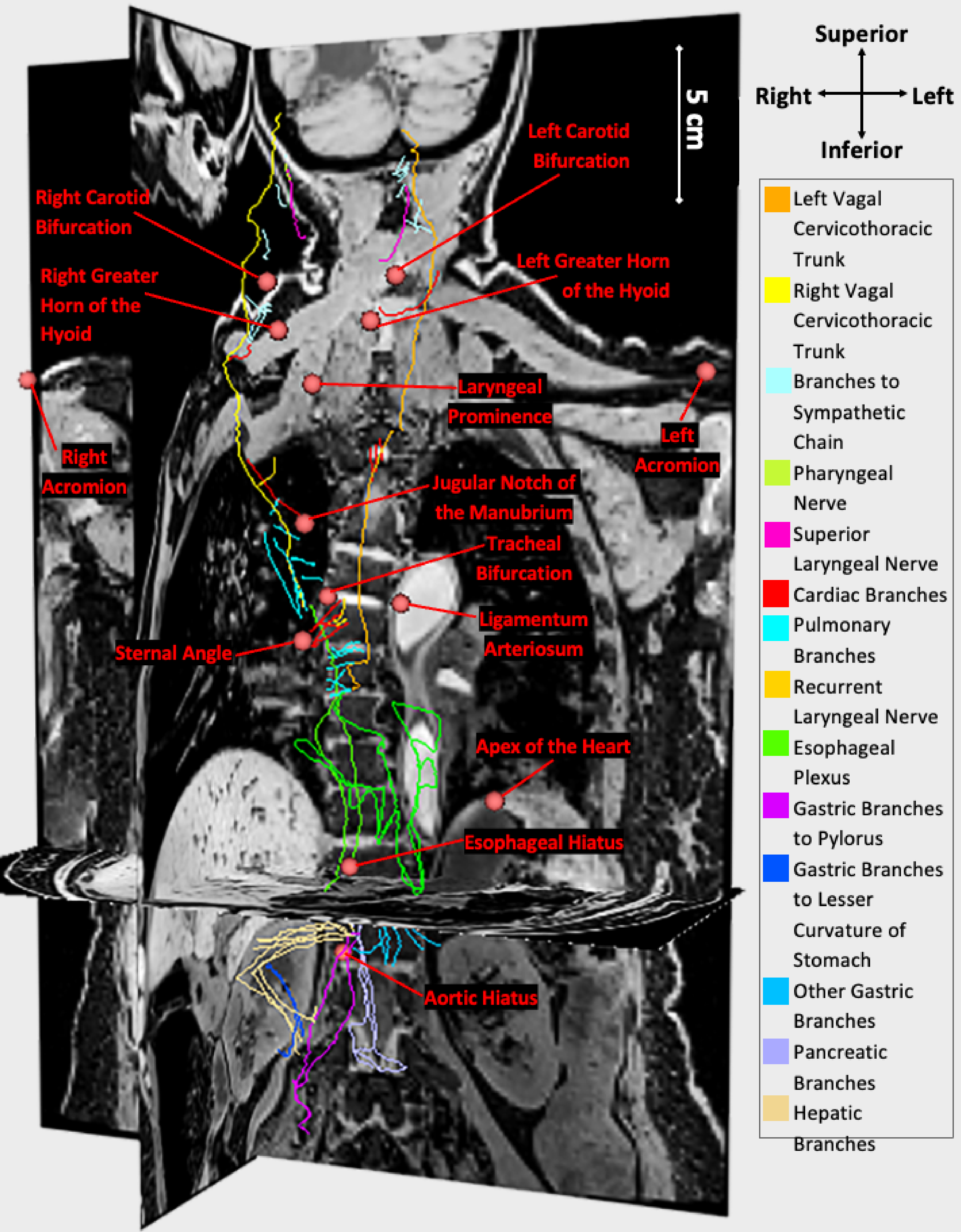
All cadavers were imaged successfully at either 0.5- or 0.6-mm isotropic resolution. Cadaver age and quality of fixation affected quality of results due to generation of small gas pockets and susceptibility artifacts. CISS provided the clearest visualization of the vagus, with tracking of the nerve trajectory as verified by gross dissection. Tracking of the right vagus was not achieved in some cadavers due to disturbance of the nerve during the fixation process.Figure 1 displays a sample 0.5 mm 3D CISS acquisition and axial reformats. Figure 2 displays colocalized CISS and VIBE images. Figure 3 displays tracking of the left vagus nerve along with relevant anatomical structures and a comparison with a photo from the gross dissection. Figure 4 displays a comparison of CISS scans acquired with isotropic 0.4-0.7 mm resolution to demonstrate the need for high resolution acquisitions.
Discussion & Conclusion
We demonstrated bilateral tracking of the vagus nerve in embalmed human cadavers using high-resolution CISS imaging. Current vagus nerve interventions focus on locating the nerve in the neck, but better imaging and characterization can lead better treatment with clearer understanding of nerve trajectory. Future work aims to incorporate acceleration via parallel imaging as part of translation towards in vivo MRI as part of planning of therapy including neuromodulation strategies.Acknowledgements
This work was funded by NIH’s Stimulation Peripheral Activity to Relieve Conditions (SPARC) - Reconstructing Vagal Anatomy (REVA) 75N98022-SPARC.References
1 Horn, C. C., Ardell, J. L. & Fisher, L. E. Electroceutical Targeting of the Autonomic Nervous System. Physiology (Bethesda) 34, 150-162 (2019). https://doi.org/10.1152/physiol.00030.2018
2 Opie, N. L. & O'Brien, T. J. The potential of closed-loop endovascular neurostimulation as a viable therapeutic approach for drug-resistant epilepsy: A critical review. Artif Organs 46, 337-348 (2022). https://doi.org/10.1111/aor.14007
3 Blitz, A. M., Aygun, N., Herzka, D. A., Ishii, M. & Gallia, G. L. High Resolution Three-Dimensional MR Imaging of the Skull Base: Compartments, Boundaries, and Critical Structures. Radiol Clin North Am 55, 17-30 (2017). https://doi.org/10.1016/j.rcl.2016.08.011
4 Blitz, A. M. et al. Contrast-Enhanced CISS Imaging for Evaluation of Neurovascular Compression in Trigeminal Neuralgia: Improved Correlation with Symptoms and Prediction of Surgical Outcomes. AJNR Am J Neuroradiol 39, 1724-1732 (2018). https://doi.org/10.3174/ajnr.A5743
5 Chaudhry, A. et al. Detection of the Stellate and Thoracic Sympathetic Chain Ganglia with High-Resolution 3D-CISS MR Imaging. AJNR Am J Neuroradiol 39, 1550-1554 (2018). https://doi.org/10.3174/ajnr.A5698
6 Northcutt, B. G. et al. High-Resolution MRI Findings following Trigeminal Rhizotomy. AJNR Am J Neuroradiol 37, 1920-1924 (2016). https://doi.org/10.3174/ajnr.A4868
Figures