1894
Feasibility of diffusion-weighted and magnetization transfer imaging of the tibial nerve in vivo using 7 Tesla: a pilot reproducibility study1NMR Research Unit, Queen Square MS Centre, Department of Neuroinflammation, UCL Queen Square Institute of Neurology, University College London, London, United Kingdom, 2Queen Square Centre for Neuromuscular Diseases, University College London, London, United Kingdom, 3Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 4London Collaborative Ultra high field System (LoCUS), London, UK, Kings College London, London, United Kingdom, 5Guys and St Thomas’ NHS Foundation Trust, Kings College London, London, United Kingdom, 6Department of Bioengineering, Imperial College London, London, United Kingdom, 7Centre for Care Research and Technology, UK Dementia Research Institute, London, United Kingdom, 8Neuroradiological Academic Unit, UCL Queen Square Institute of Neurology, University College London, London, United Kingdom, 9Lysholm Department of Neuroradiology, National Hospital for Neurology and Neurosurgery, London, United Kingdom, 10Department of Brain and Behavioural Sciences, University of Pavia, Pavia, Italy, 11Digital Neuroscience Centre, IRCCS Mondino Foundation, Pavia, Italy
Synopsis
Keywords: Peripheral Nerves, Diffusion Tensor Imaging, Magnetization Transfer
Motivation: Quantitative and semi-quantitative magnetic resonance imaging investigations of the peripheral nerves in vivo using 7 Tesla are currently limited.
Goal(s): To obtain standard diffusion tensor imaging (DTI) metrics and magnetization transfer ratio (MTR) in the healthy tibial nerve in vivo and to assess the reproducibility of these measures.
Approach: Reproducibility was assessed through repeated measurements (scan-rescan) and calculation of the coefficient of variation between measurements.
Results: The reproducibility assessment results are presented along with normative DTI and MTR measures in the tibial nerve, which can serve as reference in future studies of pathological conditions affecting the lower peripheral nerves.
Impact: This pilot study demonstrates the feasibility of using 7 Tesla magnetic resonance imaging to assess the healthy tibial nerve in vivo using diffusion-weighted and magnetization transfer imaging, opening up the possibilities to investigate lower peripheral neuropathies with higher spatial resolution.
Introduction
Magnetic resonance imaging (MRI) has been used successfully for assessing the peripheral nervous system (PNS) in a number of pathological conditions affecting the peripheral nerves. However, studies have been hampered by various technical factors, mainly related to the small size of the peripheral nerves1-3. High-field 7 Tesla (T) MRI offers inherently enhanced signal-to-noise ratio and contrast-to-noise ratio, compared to lower field strength MRI systems2,4, thus enabling imaging with superior spatial resolution. The value of combining conventional anatomical MRI with quantitative and semi-quantitative MRI methods such as diffusion tensor imaging (DTI) and magnetization transfer ratio (MTR) for assessing the peripheral nerves has previously been demonstrated in several studies using lower magnetic field strength, such as 3T MRI. However, similar investigations using 7T MRI are limited, with only a few studies so far reporting results from assessments of the upper extremity nerves5-7. Given the limited number of studies using 7T MRI to assess the PNS at various anatomical locations, coupled with the fact that the lower extremity nerves are also damaged in a number of pathological conditions8,9, this pilot study aimed to assess the reproducibility of DTI and MTR measurements in the tibial nerve of healthy volunteers and to determine normative values to serve as reference in future investigations of pathological conditions affecting the lower peripheral nerves.Methods
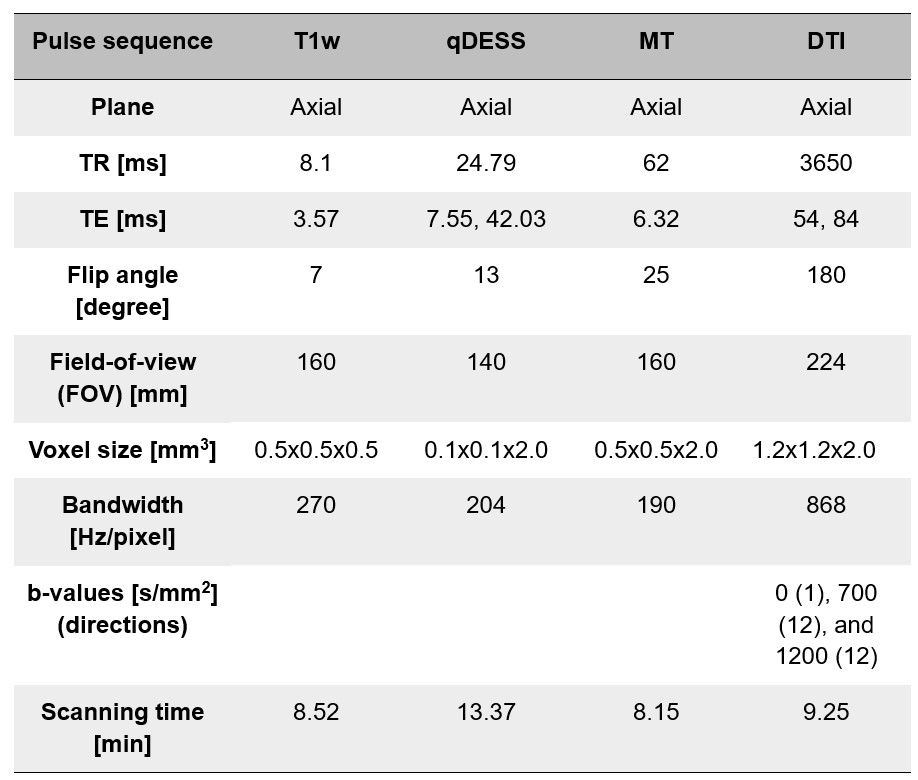
Participants: Six healthy volunteers (2 females, mean age 38.8 years, range 27-49 years) were recruited. The study was approved by the local review board and informed consent was obtained from all study participants. As part of the reproducibility assessment, half of the participants (N=3/6) returned for a re-scan session at least one week after their first scan.MR imaging: Imaging was performed using a 7T MRI system (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany). Each participant had their right ankle imaged in the feet-first supine position using the 1Tx/28Rx RAPID knee coil (https://www.rapidbiomed.de/). High-resolution T1-weighted (T1w) and quantitative double-echo steady-state (qDESS10,11) sequences were acquired in the axial plane for high-resolution anatomical imaging. DTI was performed using readout-segmented echo-planar imaging. MTR data was collected both with and without magnetization transfer saturation pulses using a 3D multi-echo gradient-echo sequence. Details of the acquisition parameters used are shown in Table 1.
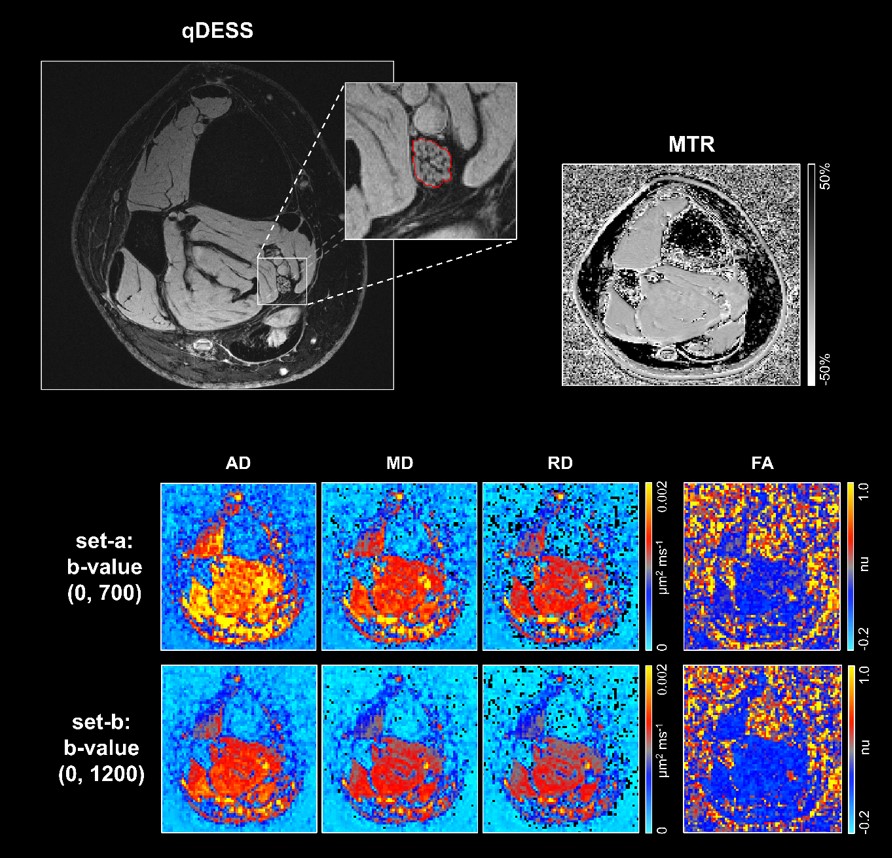
Image analysis: The tibial nerve was manually segmented in FSLview (http://www.fmrib.ox.ac.uk/fsl/) using the images from the first qDESS echo, resulting in binary masks for each image slice. The qDESS images and masks were resampled to match the DTI and MTR image resolution, aligned and registered with the NiftyReg registration toolkit12. Diffusion-weighted data were fitted using Dipy13,14 to obtain standard DTI metrics of axial, radial, mean diffusivity (AD, RD, MD, respectively) and fractional anisotropy (FA) in two different ways, to account for the range of b-values used in previously published reports in the upper extremities5,15, using: set-a) b=0 and b=700 s/mm2 and set-b) b=0 and b=1200 s/mm2. MTR was calculated from the on- and off-resonance acquisitions. To evaluate scan-rescan reproducibility, the same rater performed tibial nerve segmentation on the images obtained from both scan sessions. The mean and standard deviation (±SD) of MTR and DTI measures were calculated across all participants. The percent coefficient of variation (%COV) was calculated to determine the scan-rescan reproducibility.
Results
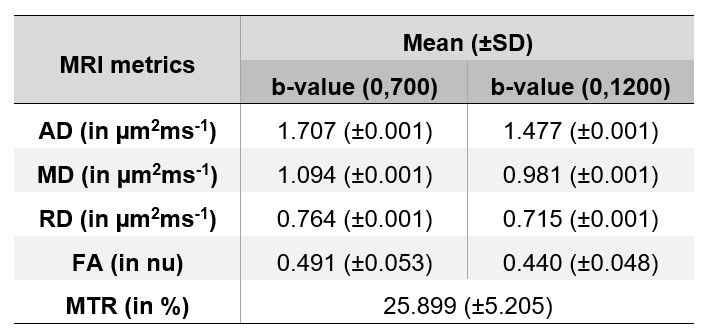
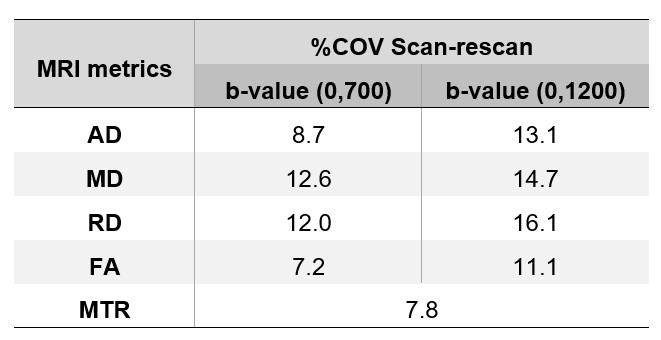
Example maps of DTI metrics (AD, RD, MD, and FA) for set-a) and set-b), and MTR maps are shown in Figure 1. Table 2 presents mean (±SD) MTR and DTI measures across all 6 participants. Table 3 displays the scan-rescan reproducibility as %COV for each MRI-derived measure separately.Discussion and Conclusion
This pilot study demonstrates the feasibility of using 7T high-resolution anatomical MRI combined with DTI and MTR to assess the healthy tibial nerve in vivo. DTI and MTR measures were in line with existing literature5-7. Moreover, they were obtained with sufficiently high reproducibility, as demonstrated by the low scan-rescan %COV values (worst case scenario: %COV=16.1%), indicative of the 7T potential value of detecting subtle changes in nerve composition and microstructure with high spatial resolution, otherwise not possible in clinically feasible times on standard 1.5T/3T MRI. Future investigations in a larger sample population will be required to verify the reproducibility results obtained in this study and to determine the potential role of these measures (with the use of 7T MRI) in characterizing pathological conditions affecting the peripheral nerves.Acknowledgements
This work using 7T MRI is supported by the Wellcome Trust Collaboration in Science grant [WT201526/Z/16/Z]. RB receives a scholarship from Chiang Mai University, Chiang Mai, Thailand. RS receives funding from the BRC (BRC1130/HEI/RS/11041). PJL receives funding from The Wellcome Trust (220473/Z/20/Z), The Edmond J Safra Foundation, NIHR Imperial BRC, and NIH (R01EB002524). CGWK receives funding from Horizon 2020 (Research and Innovation Action Grants Human Brain Project 945539 (SGA3)), BRC (#BRC704/CAP/CGW), MRC (#MR/S026088/1), Ataxia UK, Rosetrees Trust (#PGL22/100041 and #PGL21/10079). CGWK is a shareholder in Queen Square Analytics Ltd. MCY received funding from the National Brain Appeal’s Innovation Fund (https://www.nationalbrainappeal.org/).References
- Chhabra A, et al. MR neurography: advances. Radiology research and practice 2013; 2013.
- Vaughan JT, et al. 7T vs. 4T: RF power, homogeneity, and signal‐to‐noise comparison in head images. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 2001; 46: 24-30.
- Pohmann R, et al. Signal‐to‐noise ratio and MR tissue parameters in human brain imaging at 3, 7, and 9.4 tesla using current receive coil arrays. Magnetic resonance in medicine 2016; 75: 801-809.
- Juras V, et al. Comparison of 3 T and 7 T MRI clinical sequences for ankle imaging. European journal of radiology 2012; 81: 1846-1850.
- Schmid AB, et al. Feasibility of diffusion tensor and morphologic imaging of peripheral nerves at ultra-high field strength. Investigative Radiology 2018; 53: 705.
- Raval SB, et al. Ultra-high field upper extremity peripheral nerve and non-contrast enhanced vascular imaging. PloS one 2017; 12: e0175629.
- Haakma W, et al. 7T diffusion MRI of the forearm nerves. In: International Society Magnetic Resonance in Medicine, p.3473.
- Pham M, et al. Peripheral nerves and plexus: imaging by MR-neurography and high-resolution ultrasound. Current opinion in neurology 2014; 27: 370-379.
- Kollmer J, et al. MR neurography: diagnostic imaging in the PNS. Clinical neuroradiology 2015; 25: 283-289.
- Chaudhari AS, et al. Combined 5‐minute double‐echo in steady‐state with separated echoes and 2‐minute proton‐density‐weighted 2D FSE sequence for comprehensive whole‐joint knee MRI assessment. Journal of Magnetic Resonance Imaging 2019; 49: e183-e194.
- Sveinsson B, et al. Feasibility of simultaneous high‐resolution anatomical and quantitative magnetic resonance imaging of sciatic nerves in patients with Charcot–Marie–Tooth type 1A (CMT1A) at 7T. Muscle & Nerve 2022; 66: 206-211.
- Ourselin S, et al. Reconstructing a 3D structure from serial histological sections. Image and vision computing 2001; 19: 25-31.
- Garyfallidis E, et al. Dipy, a library for the analysis of diffusion MRI data. Front Neuroinform 2014; 8: 8.
- Hansen B, et al. Data for evaluation of fast kurtosis strategies, b-value optimization and exploration of diffusion MRI contrast. Sci Data 2016; 3: 1-5.
- Bao S-S, et al. Effect of Value on Imaging Quality for Diffusion Tensor Imaging of the Spinal Cord at Ultrahigh Field Strength. BioMed Research International 2021; 2021.
Figures