1893
Super-resolution MRI of Human Olfactory Bulb and Tract at 3T1Philips Healthcare, New York, NY, United States, 2Philips Healthcare, BEST, Netherlands, 3Philips Healthcare, Boston, MA, United States, 4Memorial Sloan Kettering Cancer Center, New York, NY, United States, 5Albert Einstein College of Medicine and Montefiore Medical Center, New York, NY, United States
Synopsis
Keywords: Structural Connectivity, Neurodegeneration
Motivation: Olfactory bulb and tract imaging with high resolution is required for patient evaluation
Goal(s): Optimized protocol along with super resolution deep learning to improve olfactory bulb and tract imaging
Approach: Optimized T2 weighted and DTI imaging along with deep learning reconstruction was performed and results were evaluated
Results: Good agreement between existing and proposed methods were observed while the proposed methods improves resolution with better noise performance.
Impact: This work will allow olfactory system high resolution imaging to serve as a diagnostic tool for patient evaluation.
Introduction
Human olfaction supports cognitive and behavioral functions. Olfactory dysfunction is correlated with neurological conditions such as depression, dementia, epilepsy and has been shown to play a role in COVID 19 patients related anosmia [1]. Imaging Olfactory bulb (OB) and olfactory tract (OT) is challenging due to their small size, and their location within the sinus cavities with high magnetic susceptibility variations. This is particularly true for diffusion , which is sensitive to neurological microstructural fidelity and its function [2,3]. The clinically widely used T2 weighted TSE (for structural) and single-shot SE EPI (for DWI and DTI) sequences suffer from limited spatial resolution. High-resolution OB and OT MRI has been proposed on human 7T scanner in a clinical research study [4]. In this work, we present optimized protocols with sub-millimeter resolution customized for structural and DTI sequences in combination with an AI-based super-resolution (AI-SR) reconstruction for OB/OT imaging on human at 3T, paving the way for human clinical research .Methods
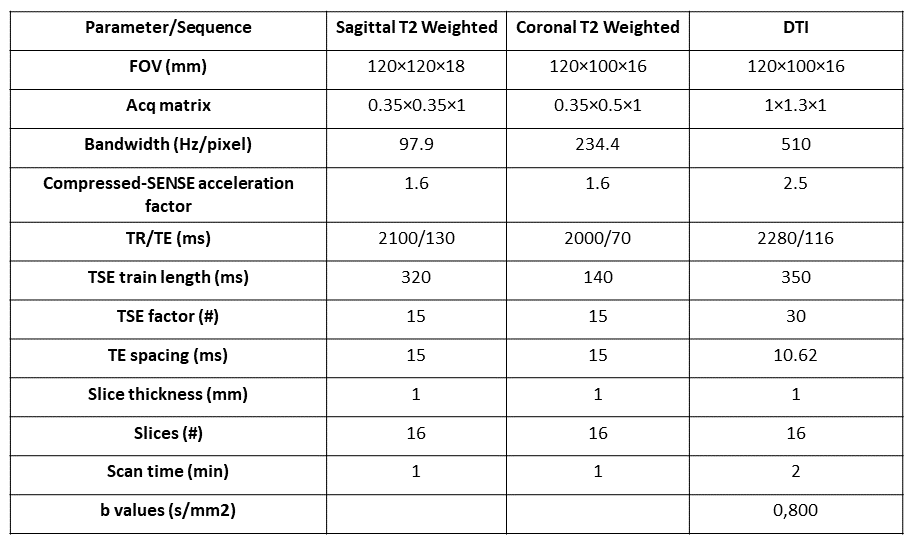
MRI was acquired with a 3T MR scanner (Philips Healthcare, Best, Netherlands) with a 32-channel head coil. To maximize SNR for the OB, the subject was asked to lie prone, which reduced the distance between OB/OT and the coil elements, doubling SNR compared to typical supine head position [2]. Both sagittal and coronal T2W TSE sequences were acquired (Table 1). Diffusion tensor imaging was acquired in the quasi-axial and quasi-coronal planes using a high-resolution, multi-slice 2D single-shot, diffusion-weighted TSE sequence with 32 diffusion encoding directions (Table 1).Acquired images were first reconstructed using vendor’s default compressed-SENSE reconstruction, followed by AI-based (AI-SR) reconstruction to both remove noise and increase resolution. The algorithm (SmartSpeed) consists of an iterative method to reconstruct images from acquired k-space data [5,6,7]. Apparent diffusion coefficient (ADC), Fractional anisotropy (FA) and fiber-tracking images were then generated on the MR console using the default algorithms.
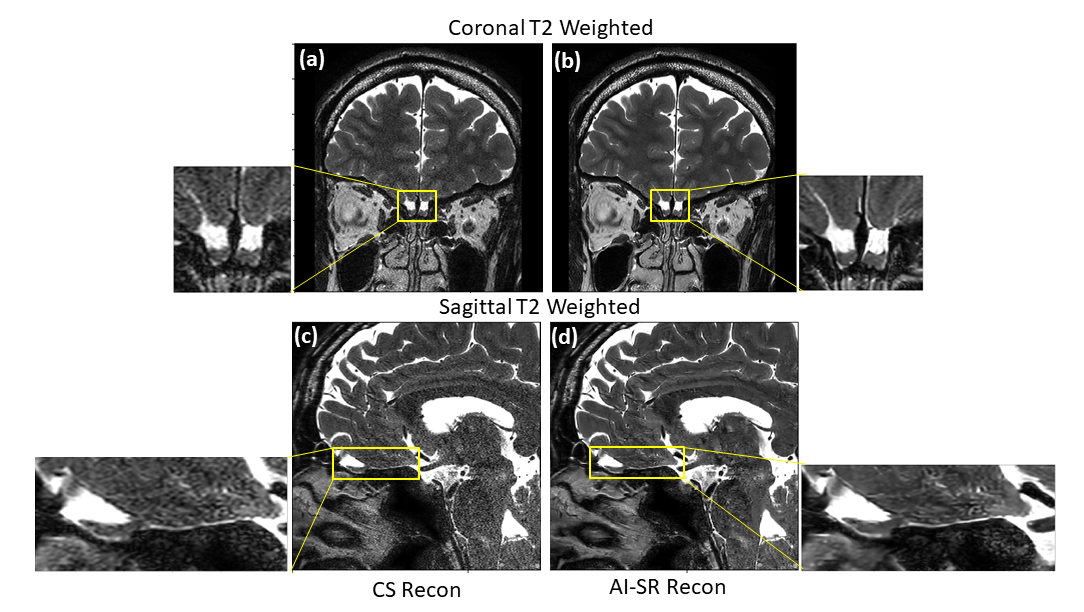
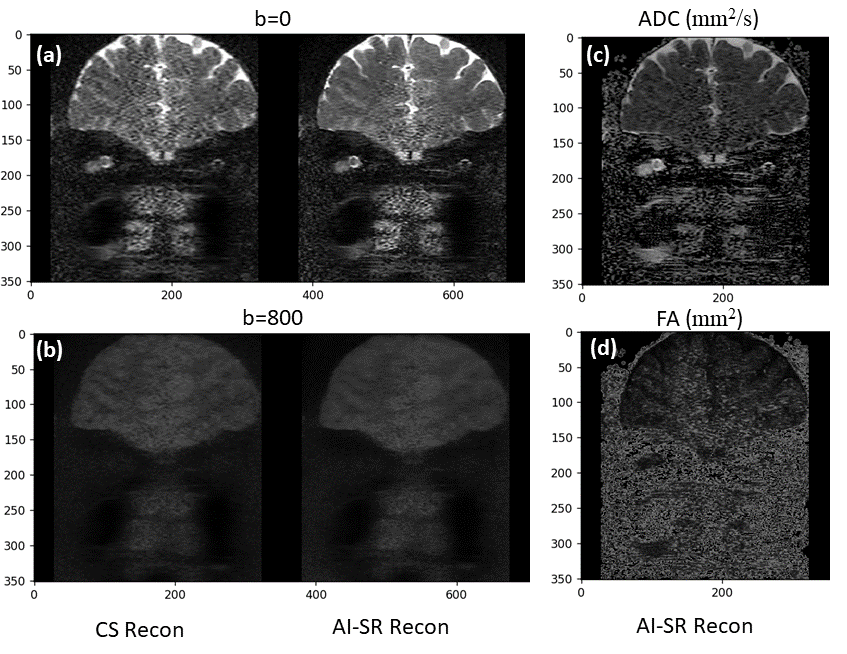
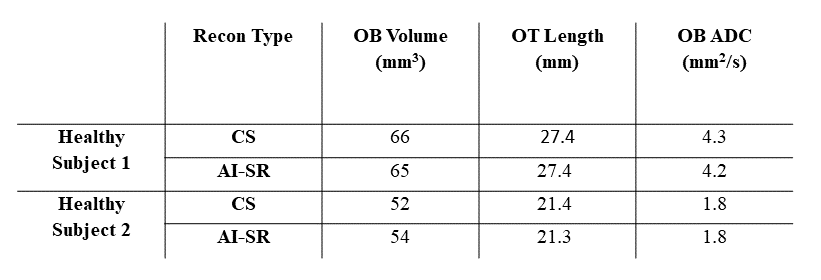
To compare results, both CS and AI-SR recon for sagittal and coronal T2-weighted images in one subject are shown. In addition, b-values from both reconstruction methods along ADC and FA maps for AI-SR recon is shown. Quantitative analysis including OB volume, ADC values, and OT length are reported in both reconstruction methods and in two healthy volunteers. For OB volume and OT length calculations, ROIs and lines were drawn on coronal T2-weighed images.
Results
In Figure 1, comparison of CS (a) recon with AI-SR (b) in coronal acquisition image (top) shows while contrast in the brain including white and grey matter remains similar, noise has been effectively removed in the AI-SR reconstruction. OB and OT structure and boundaries in AI-SR reconstruction are sharper with more details compared to CS recon. Similar trends can be observed in sagittal acquisition image (bottom) where OB volume and specifically OT show more details and less artifacts in AI-SR (d) recon compared to CS (c). In Figure 2, comparison of b=0 (a) and b=800 s/mm2(b) using conventional CS recon vs AI-SR, shows good contrast agreement while the latter method significantly reduces noise and improves image sharpness. Corresponding ADC and fractional anisotropy (FA) maps calculated from AI-SR recons demonstrate improved image quality. Images in both recon methods minimally suffer from geometric distortion and susceptibility-related artifacts.In Table 2, comparison of OB ADC value and OB volume in two subjects demonstrate consistent values in healthy volunteers as reported before [3]. Comparison of values in CS and AI-SR methods shows good agreement between the two.
Discussion and Conclusion
We showed the feasibility of imaging OB and OT with high spatial resolution at 3T, suitable for clinical research studies. This is achieved by combining the optimized the clinical protocols for higher SNR and spatial-resolution imaging, and a super-resolution AI algorithm for higher spatial-resolution and noise reduction during reconstruction. Except for its inherent relatively lower SNR, 3T MRI of OB and OT has advantage compared to 7T including system and coils availability, lower SAR and magnetic susceptibilities and lower image distortion (TSE sequence). In addition for diffusion, lower signal loss and image distortion can be achieved with 3T. In this study, we show that a 1-min TSE sequences optimized of olfactory MRI had high SNR and high spatial resolution, adequate for clinical research studies. The OBT and OTL measurements were consistent between the CS and AI-SR reconstructions. While we only presented 2D TSE, 3D sequences can provide additional SNR and allow for higher spatial resolution with multi-plane reconstructions. In conclusion, high spatial resolution structural and functional human OB and OT MRI are feasible at 3T, potentially facilitate clinical research studies on human olfactory system and its interaction with other disease conditions.Acknowledgements
References
[1] Frosolini A, Parrino D, Fabbris C, Fantin F, Inches I, Invitto S, Spinato G, Filippis C. Magnetic Resonance Imaging Confirmed Olfactory Bulb Reduction in Long COVID-19: Literature Review and Case Series. Brain Sci. 2022 Mar 24;12(4):430. doi: 10.3390/brainsci12040430. PMID: 35447962; PMCID: PMC9029157.
[2] Woo, Cynthia C., Blake Miranda, Mithra Sathishkumar, Farideh Dehkordi-Vakil, Michael A. Yassa, and Michael Leon. "Overnight olfactory enrichment using an odorant diffuser improves memory and modifies the uncinate fasciculus in older adults." Frontiers in Neuroscience 17 (2023): 1200448.
[3] Paolini, M., Keeser, D., Ingrisch, M., Werner, N., Kindermann, N., Reiser, M., & Blautzik, J. (2015). Resting-state networks in healthy adult subjects: a comparison between a 32-element and an 8-element phased array head coil at 3.0 Tesla. Acta Radiologica, 56(5), 605-613.
[4] Miao, Xinyuan et al. “Functional Activities Detected in the Olfactory Bulb and Associated Olfactory Regions in the Human Brain Using T2-Prepared BOLD Functional MRI at 7T.” Frontiers in neuroscience vol. 15 723441. 13 Sep. 2021, doi:10.3389/fnins.2021.723441
[5] N. Pezzotti et al., "An Adaptive Intelligence Algorithm for Undersampled Knee MRI Reconstruction," in IEEE Access, vol. 8, pp. 204825-204838, 2020, doi: 10.1109/ACCESS.2020.3034287.
[6] Pezzotti, Nicola et al. “Adaptive-CS-Net: FastMRI with Adaptive Intelligence.” arXiv: Image and Video Processing (2019)
[7] Bischoff, Leon M et al. “Deep Learning Super-Resolution Reconstruction for Fast and Motion-Robust T2-weighted Prostate MRI.” Radiology vol. 308,3 (2023): e230427. doi:10.1148/radiol.230427
Figures