1892
A Preliminary Study on MRI Water Imaging-based Radiomics Nomogram to Identify Symptomatic Nerves in Primary Trigeminal Neuralgia Patients1Affiliated Hospital of North Sichuan Medical College, Nanchong, China, 2Department of Radiology, Bishan Hospital of Chongqing Medical University, Chongqing, China, 3The First Affiliated Hospital of Chengdu Medical College, Chengdu, China, 4United Imaging Research Institute of Intelligent Imaging, Beijing, China
Synopsis
Keywords: Peripheral Nerves, Nervous system, Radiomics, trigeminal neuralgia, nomogram, MRI
Motivation: Addressing the diagnostic challenges of Primary trigeminal neuralgia (PTN) and exploring the potential of radiomics combined with clinical features for better accuracy.
Goal(s): To establish an auxiliary diagnostic model for PTN using radiomic and clinical features.
Approach: Retrospectively analyzed 116 patients with trigeminal neuralgia, extracting 1316 radiomics features using 3D slicer and studying 13 clinical features. Lasso regression, ICC analysis, univariate and multivariate logistic regression were used for analysis.
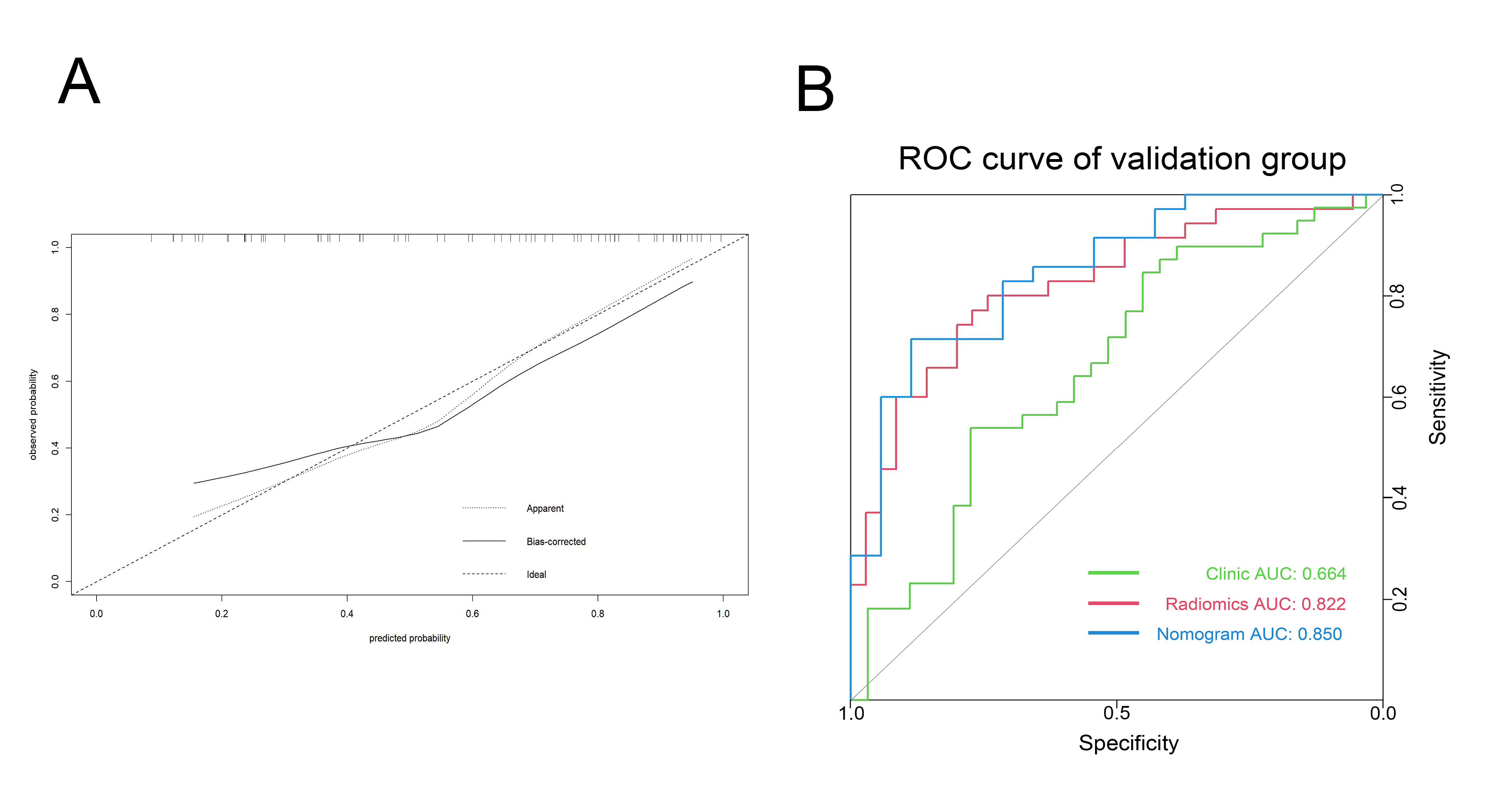
Results: Combining radiomic and clinical characteristics improved the model's AUC values to 0.85. Atrophy of the trigeminal roots might be significant in PTN diagnosis.
Impact: This study enhances PTN diagnosis, guiding clinicians with improved accuracy, potentially benefiting patients. It paves the way for further research on trigeminal root atrophy's role, optimizing treatment strategies and patient care.
Introduction
Primary trigeminal neuralgia (PTN) is a prevalent neuropathic pain condition in the brain characterized by recurring episodes of intense unilateral facial trigeminal nerve pain. The widely accepted neurovascular compression (NVC) theory explains PTN occurrence. Imaging that shows vascular compression of the trigeminal nerve pool segment is fundamental for PTN diagnostic. However, the NVC theory is debated, some PTN patients don’t exhibit vascular compression signs, while some without PTN do[1-3]. Hence, relying solely on neurovascular compression for diagnosis is inadequate. Given that PTN makes up 75% of TN cases, with its cause largely unknown and harder to diagnose than secondary TN, it’s crucial to develop a robust diagnostic method for PTN [4]. Using radiomics to pinpoint symptomatic nerves is a promising approach. Can clinical features like TPA, though challenging to discern visually, be effectively measured and incorporated into clinical models? Research in this area is notably limited. Integrating radiomics with clinical features might enhance the model’s clinical relevance.Method
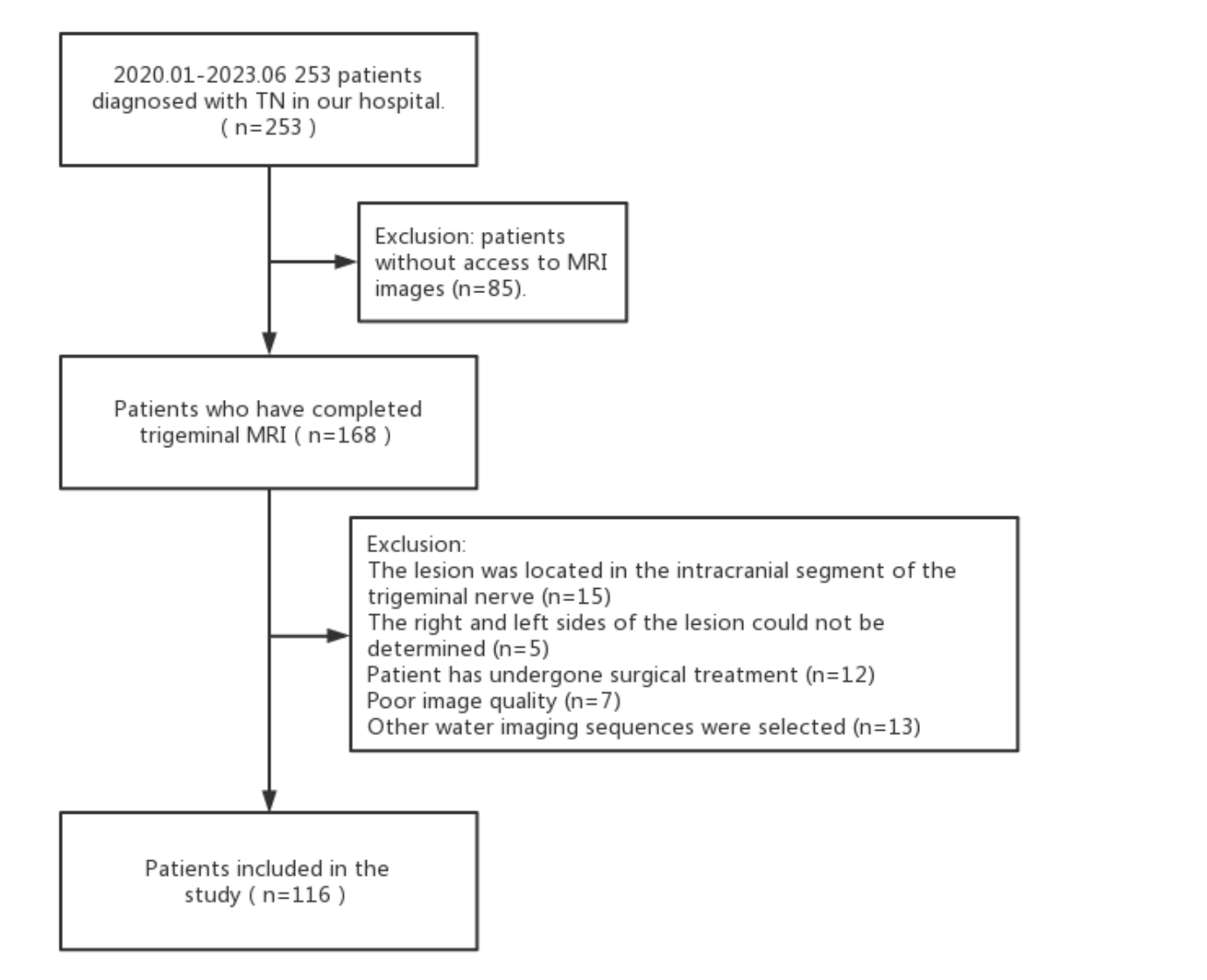
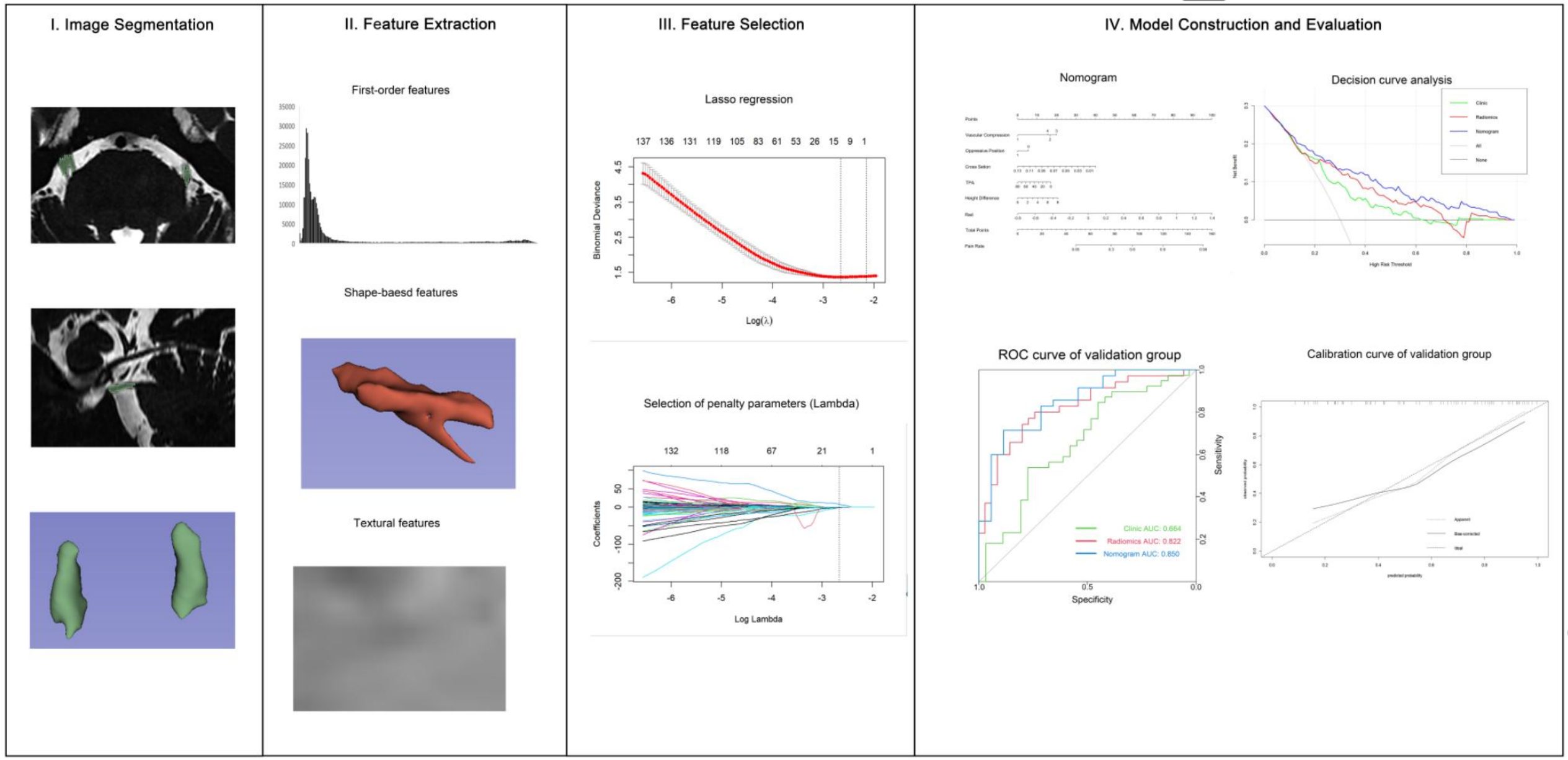
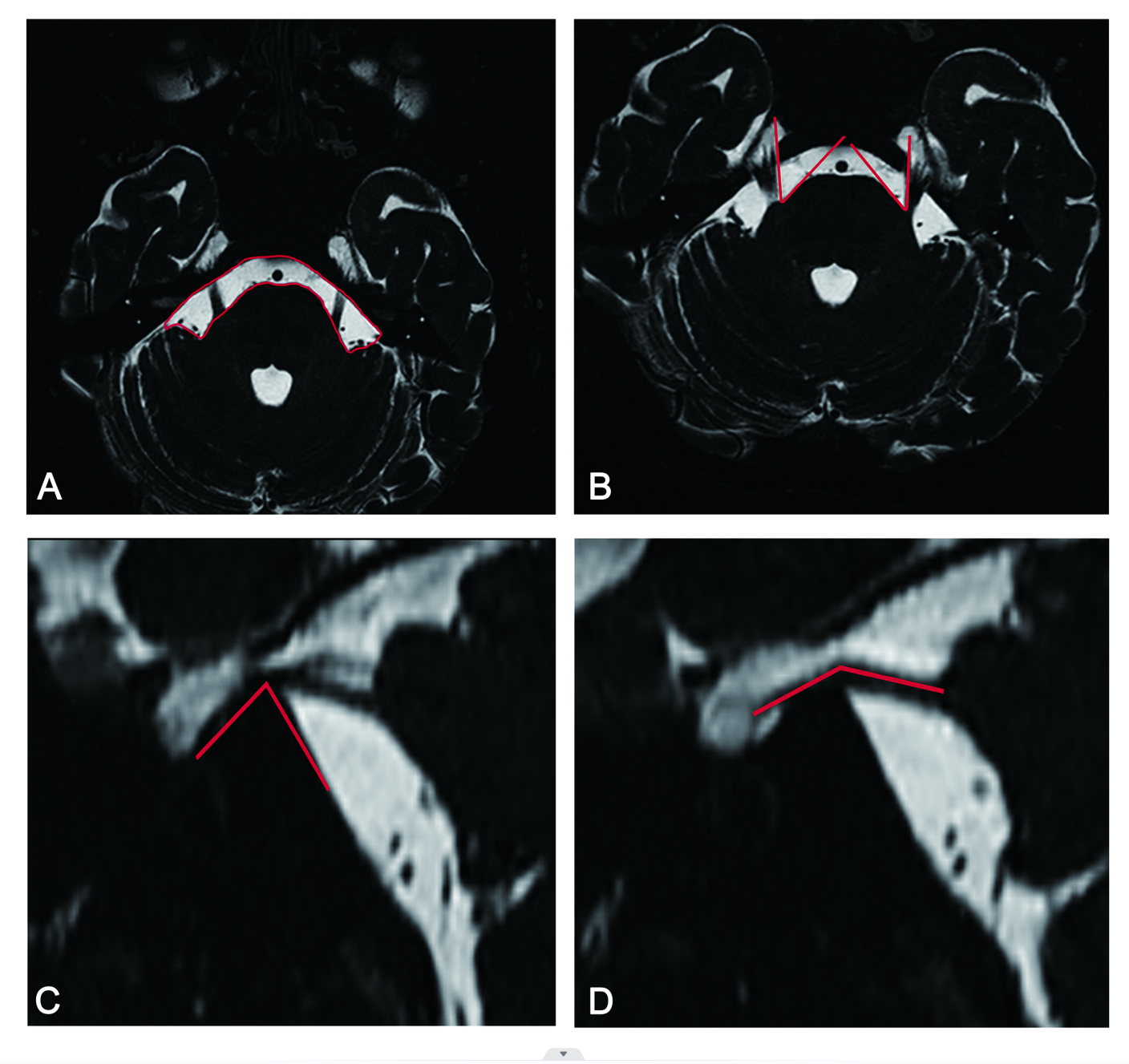
Between January 2020 to June 2023, 116 patients diagnosed with trigeminal neuralgia were retrospectively studied. One nerve was discarded due to subpar image quality, resulting in 231 nerves from 116 patients - 117 symptomatic and 114 normal. Figure 1 and Figure 2 illustrate the patient recruitment and study flowcharts, respectively.Figure 3 shows the measurement methods for some clinical features.Inclusion Criteria: 1. Pre-surgery MRI completion.2. MRI sequence is t2-mix3d-tra-spair heavy t2 water imaging.3. Clinical diagnosis of trigeminal neuralgia based on the Third Edition of International Classification of Headache Disorders[5].Exclusion criteria were:1. Patient's affected nerve is a peripheral trigeminal nerve branch.2. Indeterminate side affected by trigeminal neuralgia.3. Prior surgical treatment.4. Images unsuitable for analysis due to clarity issues or artifacts.5. Use of alternative water imaging sequences.6. Secondary trigeminal neuralgia.Using a 3.0T MRI, the trigeminal(t2-mix3d-tra-spair)data were obtained. Manual segmentation of axial images was done via the 3D slicer software, defining the region of interest (ROI) from the trigeminal nerve’s onset at the brainstem to Merkel's cave’s entrance. A total of 1316 radiomics features were extracted, alongside 13 general clinical features.Result
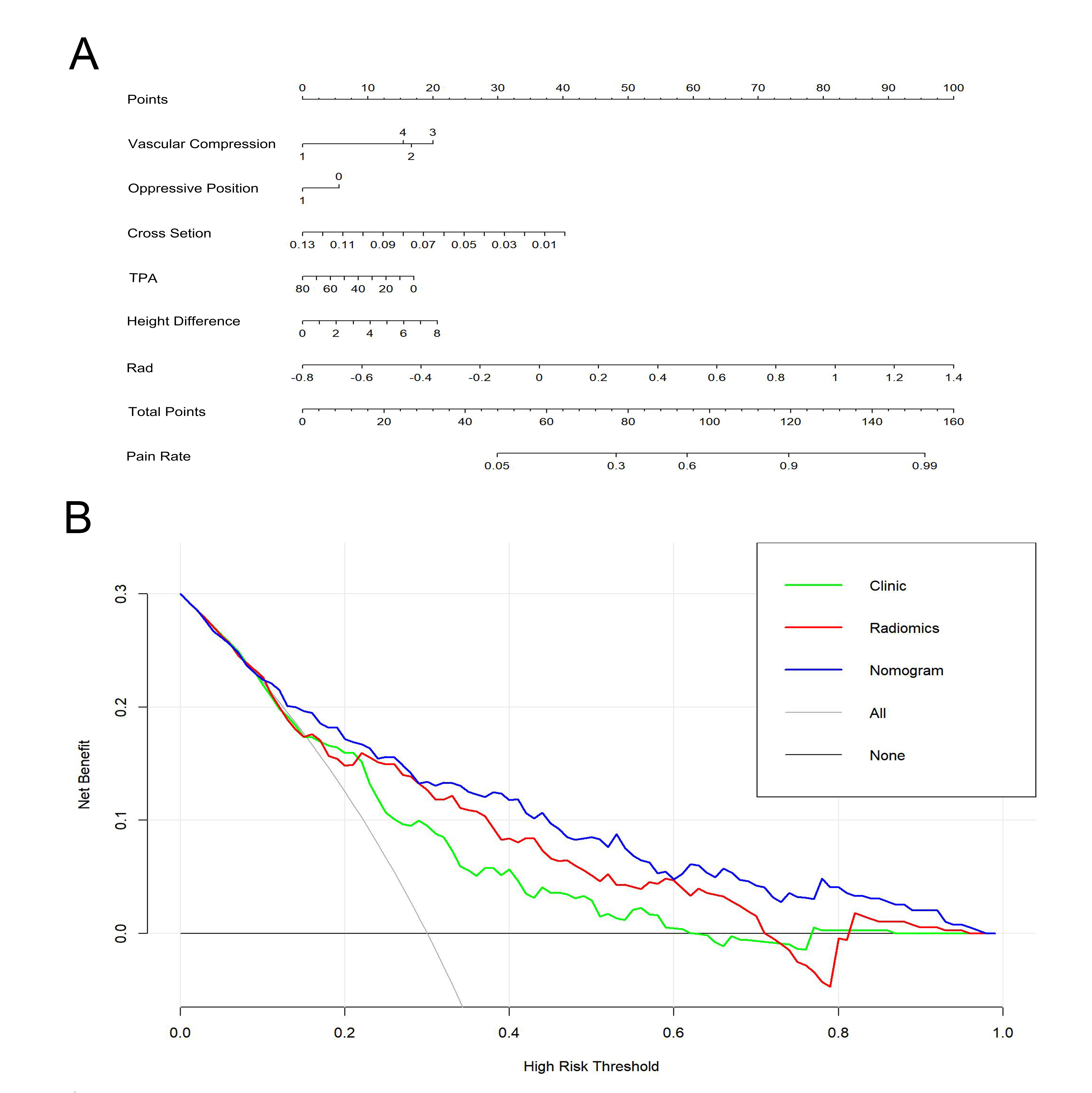
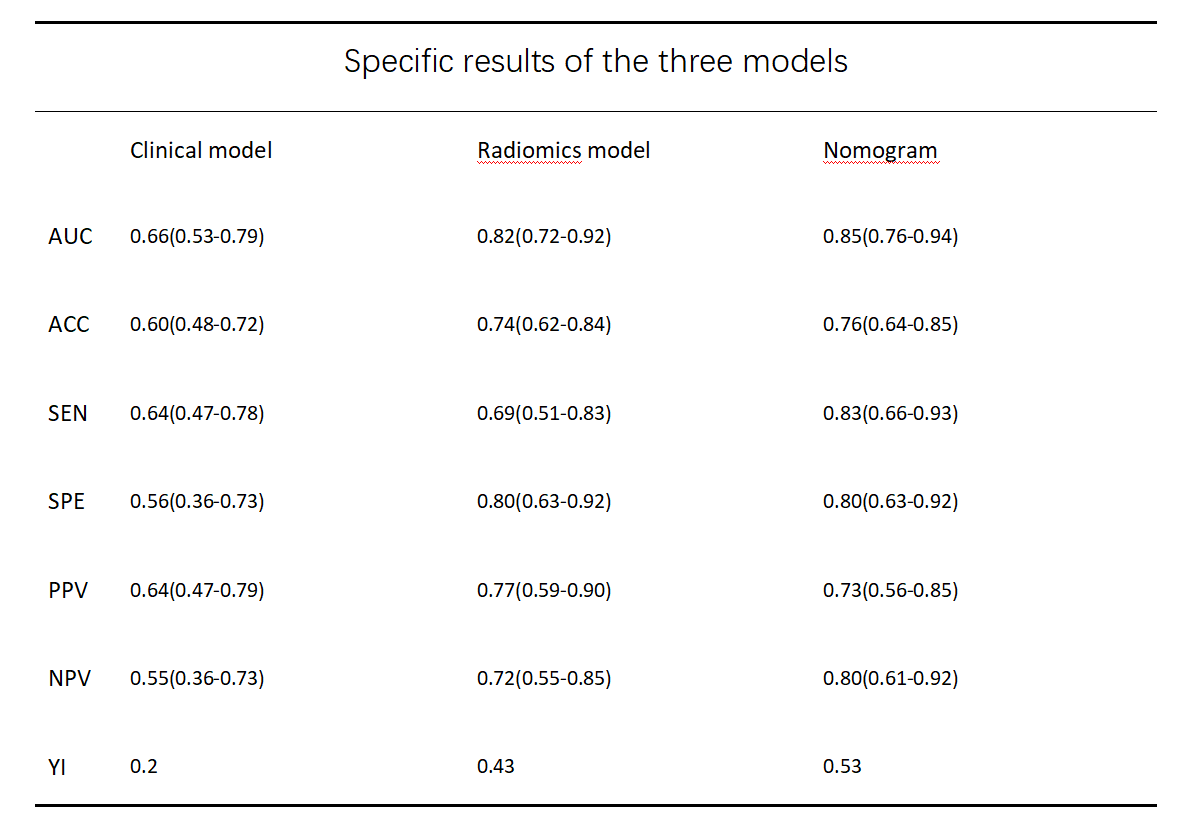
13 radiomic features were selected using Lasso regression and ICC analysis. Univariate and multivariate logistic regression revealed five clinical features as independent symptomatic nerve risk factors. Table 1 presents the combined model’s AUC values, accuracy, and the relevant 95% confidence intervals. By merging radiomic and clinical features, the combined model’s AUC values saw significant improvement. Various results are shown in Figures 4 and 5.Discussion
Our study highlights differences in radiomic textural features and clinical anatomical features in PTN patients, unrelated to vascular compression presence. Interestingly, even after excluding variables tied to the trigeminal nerve’s maximum cross-sectional area and vascular compression, the combined model’s diagnostic performance improved minimally. This suggests that the poor segment’s atrophy and thinning could be the most pivotal morphological variable in trigeminal neuralgia, with NVC as the primary catalyst. Prior research indicates that trigeminal root atrophy might be linked to pain generation, irrespective of vascular compression. These pathophysiological model could account for PTN arising from various causes, including genetic and idiosyncratic factors, even without NVC[6-8]. Our findings align with these conclusions.Conclusion
We employed radiomics to extract symptomatic and normal nerves’ radiomic features, amalgamating them with clinical attributes to create a supplementary diagnostic model for trigeminal neuralgia, demonstrating outstanding diagnostic efficiency.Acknowledgements
Not applicable.References
[1] Bendtsen L, Zakrzewska J M, Heinskou T B, et al. Advances in diagnosis, classification, pathophysiology, and management of trigeminal neuralgia[J]. Lancet Neurol, 2020,19(9):784-796. https://doi.org/10.1016/S1474-4422(20)30233-7 [2] Cruccu G, Di Stefano G, Truini A. Trigeminal Neuralgia[J]. N Engl J Med, 2020,383(8):754-762. https://doi.org/10.1056/NEJMra1914484.https://doi.org/ 10.3171/2018.9.JNS181768 [3] Hardaway F A, Holste K, Ozturk G, et al. Sex-dependent posterior fossa anatomical differences in trigeminal neuralgia patients with and without neurovascular compression: a volumetric MRI age- and sex-matched case-control study[J]. J Neurosurg, 2019,132(2):631-638. https://doi.org/ 10.3171/2018.9. JNS181768 [4] Zakrzewska J M, Wu J, Mon-Williams M, et al. Evaluating the impact of trigeminal neuralgia[J]. Pain, 2017,158(6):1166-1174. https://doi.org/10.1097/j.pain.0000000000000853[5] Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition[J]. Cephalalgia, 2018,38(1):1-211. https://doi.org/10.1177/0333102417738202[6] Di Stefano G, De Stefano G, Leone C, et al. Concomitant continuous pain in patients with trigeminal neuralgia is associated with trigeminal nerve root atrophy[J]. Cephalalgia, 2020,40(13):1502-1510. https://doi.org/10.1177/0333102420949206[7] Allam A K, Sharma H, Larkin M B, et al. Trigeminal Neuralgia: Diagnosis and Treatment[J]. Neurol Clin, 2023,41(1):107-121. https://doi.org/10.1016/j.ncl.2022.09.001[8] Bennett D L, Clark A J, Huang J, et al. The Role of Voltage-Gated Sodium Channels in Pain Signaling[J]. Physiol Rev, 2019,99(2):1079-1151. https://doi.org/10.1152/physrev.00052.2017Figures