1890
Feasibility of 3D Reduced-FOV Multi-shot Isotropic DWI in Optic Nerves1Department of Biomedical Engineering, The Chinese University of Hong Kong, Hong Kong, China, 2Multi-Scale Medical Robotics Center, Hong Kong, China, 3Department of Diagnostic Radiology, The University of Hong Kong, Hong Kong, China
Synopsis
Keywords: Head & Neck/ENT, Nerves, multi-shot, reduced-FOV, 3D isotropic DWI, optic nerves
Motivation: Conventional 2D DWI sequences suffer from several disadvantages, therefore hindering the clinical visual assessment of optic nerves.
Goal(s): This study aims to enable a 3D reduced-FOV multi-shot isotropic DWI sequence for optic nerves DWI and verify its feasibility.
Approach: The pulse sequence and corresponding reconstruction algorithm of 3D reduced-FOV 2-shot isotropic DWI was developed to achieve effective and accurate reconstruction of optic nerves.
Results: Preliminary results have shown the feasibility of our method in depicting the optic nerves with high resolution and high fidelity, therefore potentially benefiting the clinical applications of optic nerves DWI.
Impact: 3D reduced-FOV multi-shot isotropic optic nerves DWI shows superior advantages of high resolution and high fidelity compared with other conventional DWI sequences, which should be further investigated and applied for clinical applications of optic nerves.
Introduction
High-resolution diffusion-weighted imaging (DWI) can probe subtle microstructural changes in optic nerves, and several studies have demonstrated its clinical relationship related to corresponding optic nerve diseases1~3. Among them, 2D single-shot diffusion-weighted echo-planar imaging is the most commonly used sequence for data acquisition. Despite high scan efficiency, 2D single-shot DWI suffers from 1) low SNR level and signal loss associated with reduced slice thickness in pursuit of high spatial resolution, and 2) severe geometric distortion and susceptibility artifacts, therefore hindering the clinical visual assessment of optic nerves. Previous studies have proposed to apply reduced-FOV with 2D-RF, or multi-shot techniques (e.g., multiplexed sensitivity encoding; MUSE4) to improve the quality of 2D single-shot DWI5~6. However, 2D reduced-FOV multi-shot optic nerves DWI with thin slice thickness (e.g., <1.9mm) may encounter intractable aliasing artifacts due to the limitation of 2D-RF excitation. Our previous study7 demonstrated that the 3D DWI with MUSE can effectively achieve high SNR and spatial resolution in the human brain. Therefore, this study aims to enable a 3D reduced-FOV multi-shot isotropic DWI sequence for optic nerves DWI and verify its feasibility.Methods
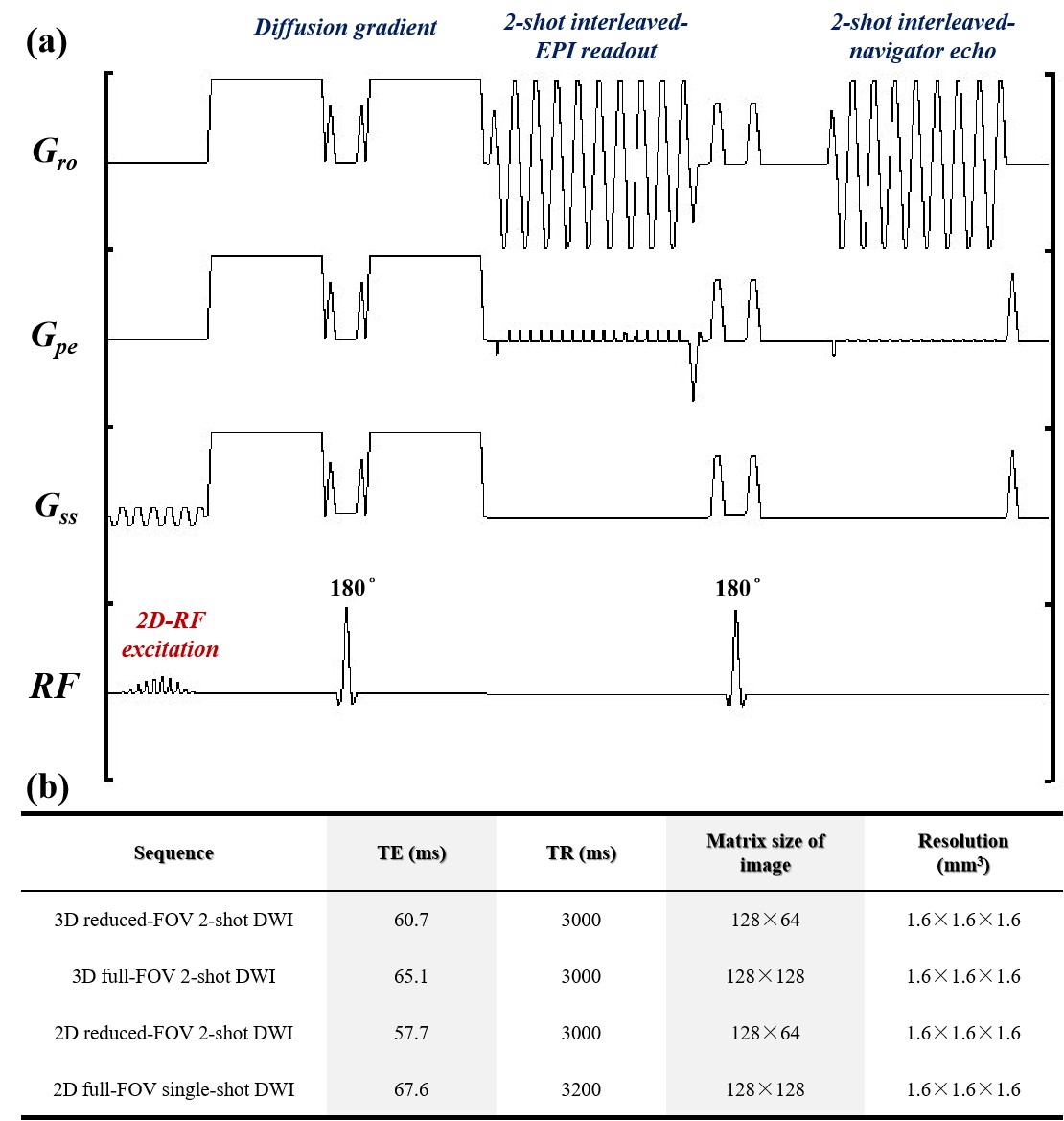
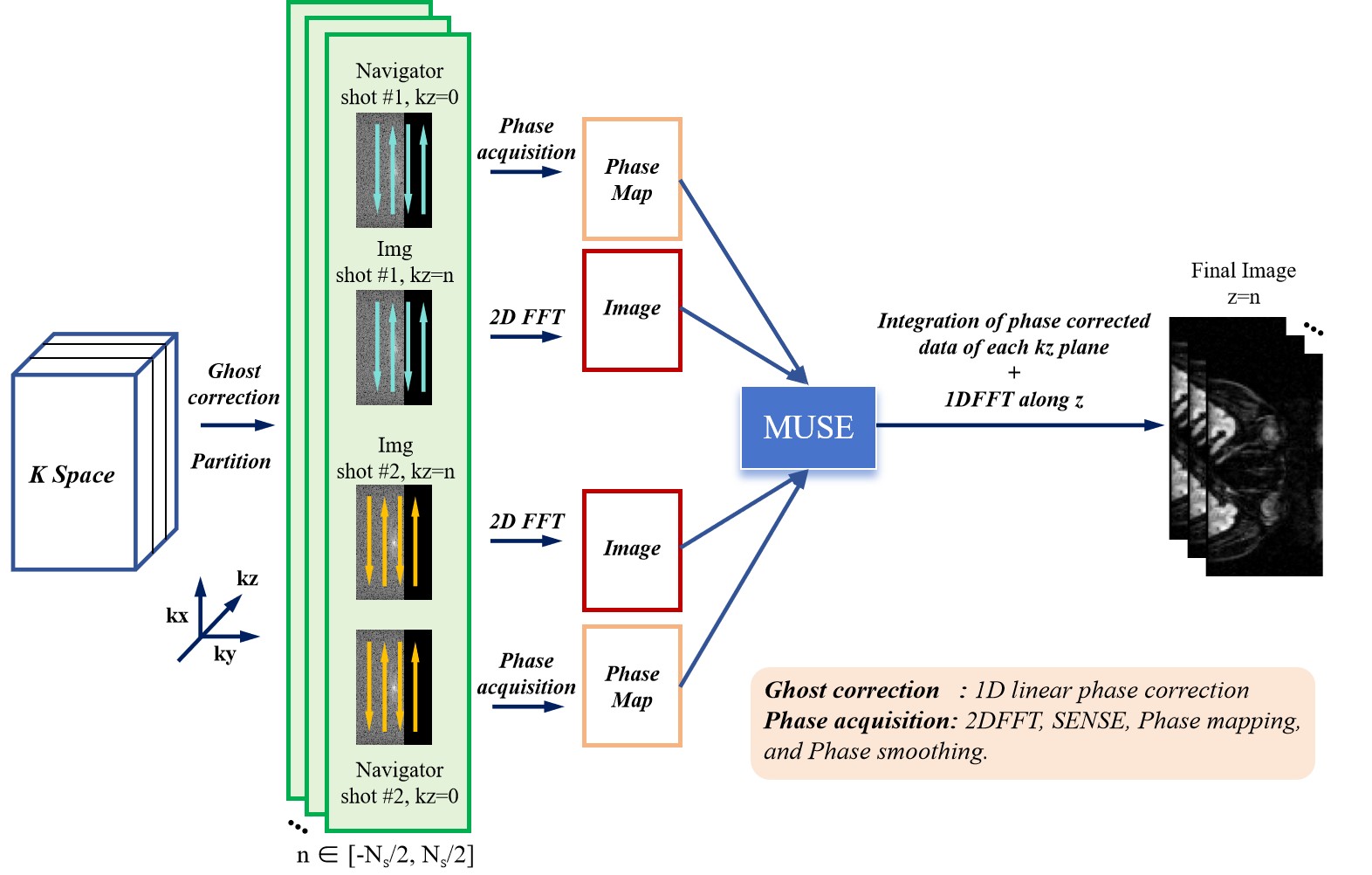
Sequence design and reconstructionFig.1(a) demonstrates the design of the proposed 3D reduced-FOV multi-shot DWI pulse sequence with a 2D-RF excitation pulse. 2D navigator echo was used to measure the inter-shot phase variations with the assumption that through-slab phase variation can be neglected for the relatively thin slab. Fig.2 illustrates the flowchart of the 3D-MUSE algorithm for reconstructing each kz plane individually7. The ghost artifacts were first corrected by 1D linear phase correction8. Subsequently, inter-shot phase variations were accurately estimated via 2-shot-interleaved navigators with strong DWI signals at zero kz and integrated into the MUSE framework with 2-shot-interleaved EPI readout for acquiring high-fidelity optic nerve DWI. To investigate the feasibility and demonstrate the effectiveness of our method for optic nerves DWI, we visually compared the reconstructed images of the proposed technique with that of other three techniques: i) 2D single-shot DWI, ii) 2D multi-shot reduced-FOV DWI, and iii) 3D multi-shot DWI.
Data acquisition
3D reduced-FOV multi-shot DWI data were collected from two healthy volunteers on a 1.5T MRI scanner (Artist, GE Healthcare) using a 19-channel head coil with the scan parameters as follows: interleaved-shot number=2, phase-FOV factor=0.50, TE/TR=60.7/3000ms, partial-Fourier factors=69% (for image signals) and 75% (for navigator echoes), excited slab thickness=25.6mm, FOVz=38.4mm, number of kz phase-encoding steps Ns=24, FOVxy=20.5cm, matrix size=128×64×24 per slab, voxel size=1.6×1.6×1.6mm3, b=500s/mm2. Scan parameters of other comparative sequences with the same isotropic resolution were listed in Fig.1(b).
Results
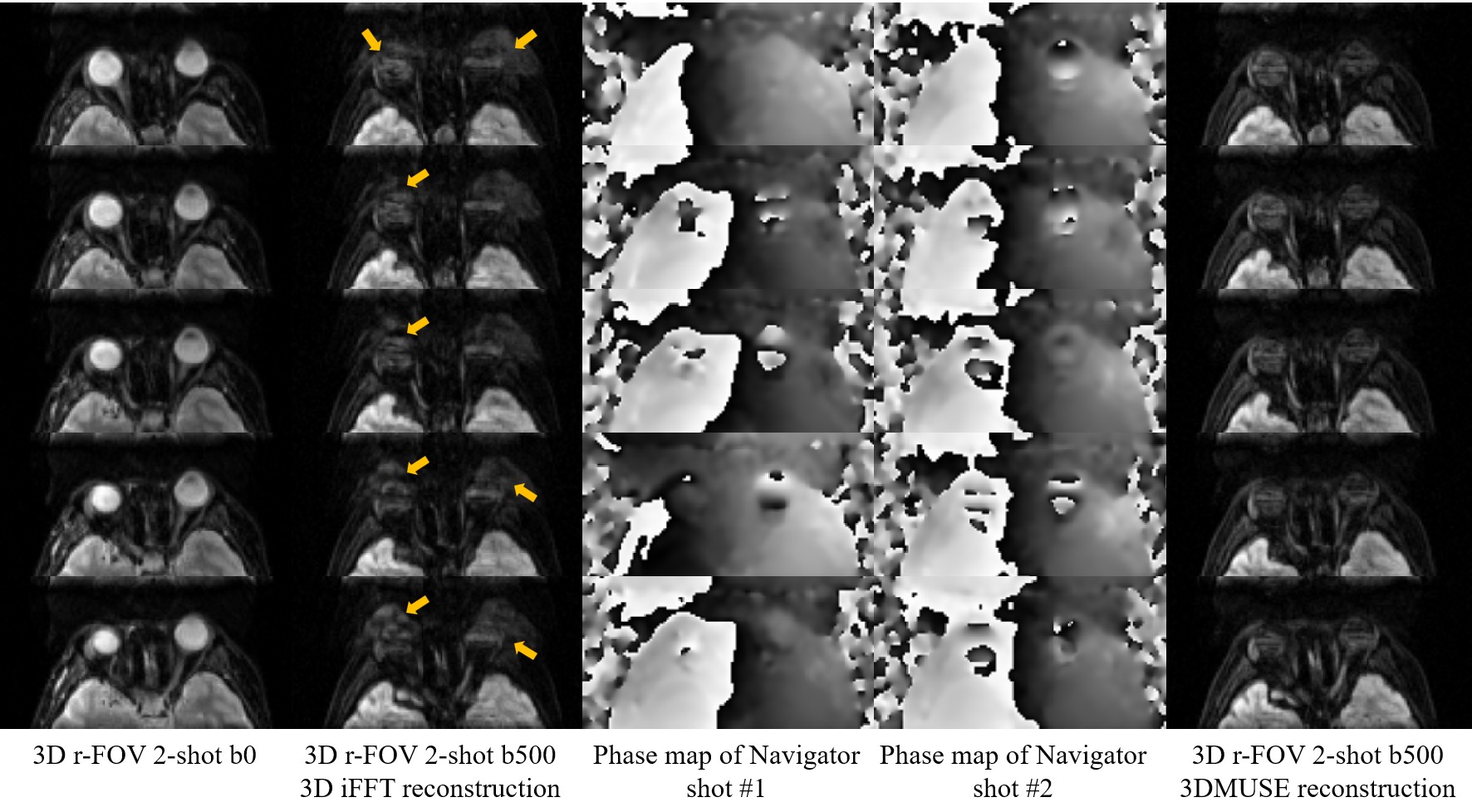
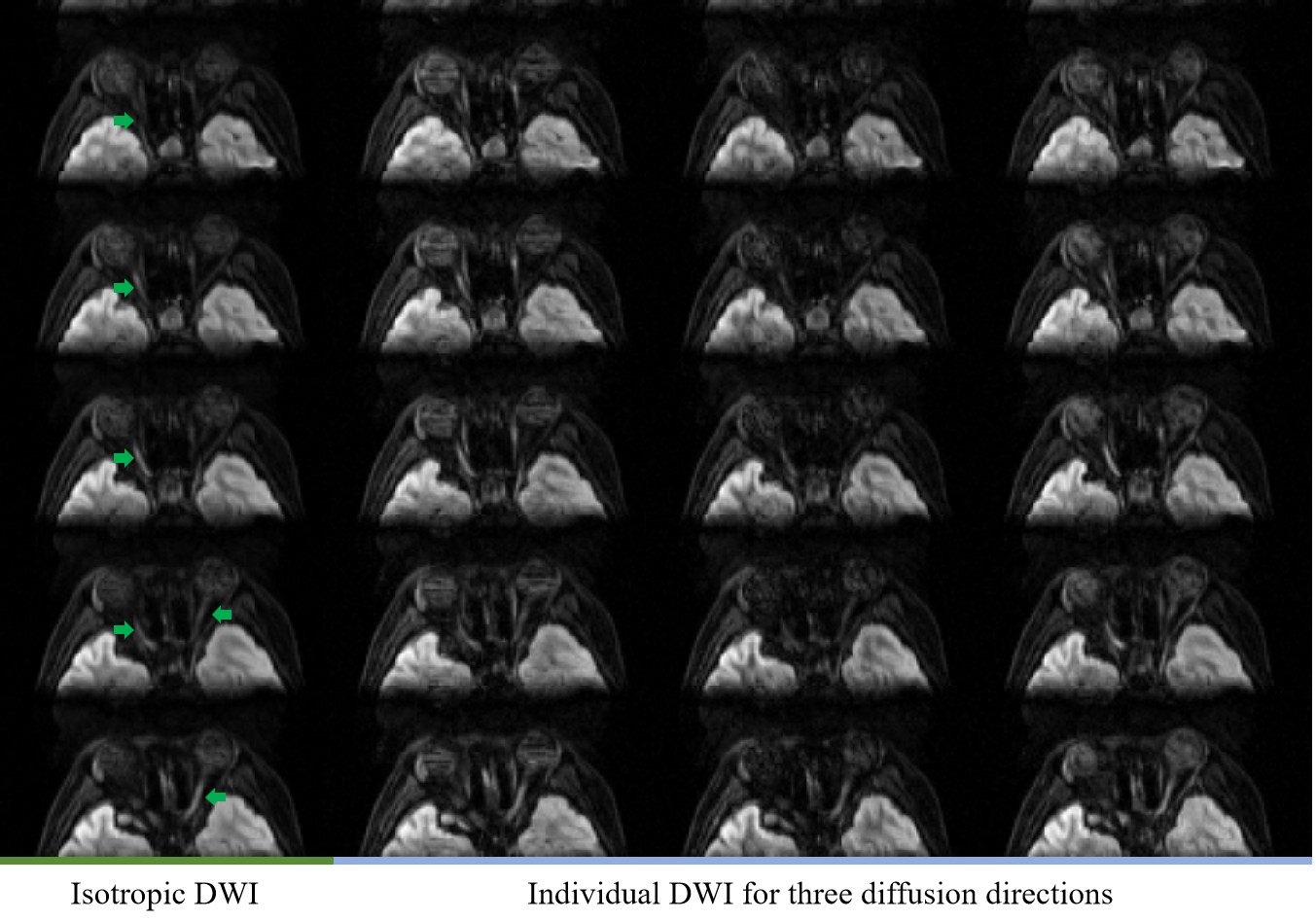
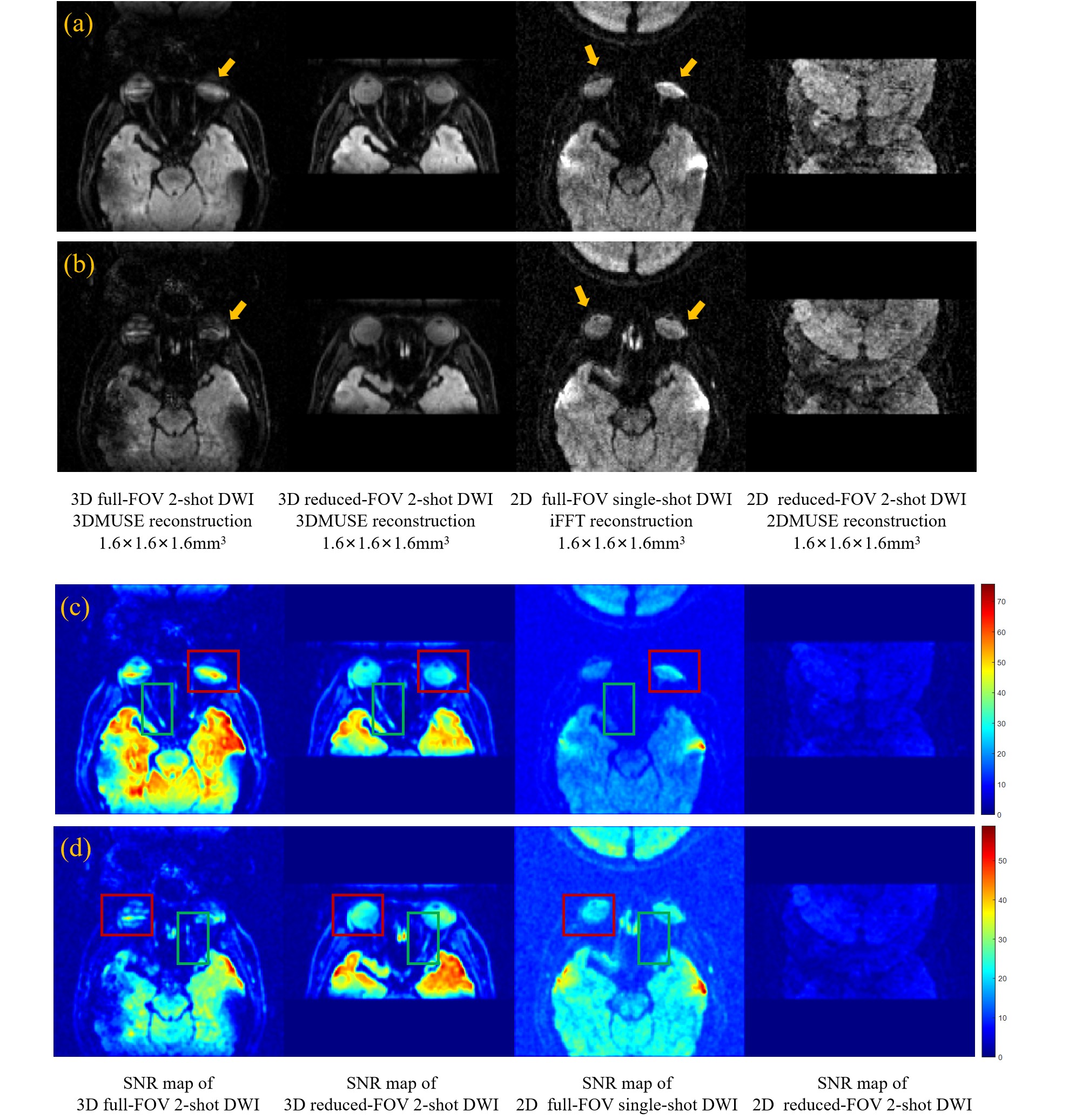
Fig.3 demonstrates the reconstruction results of 3D reduced-FOV multi-shot DWI between direct 3D-iFFT and 3D-MUSE reconstruction, suggesting the importance of inter-shot phase correction for 3D DWI. Fig.4 presents the reconstruction results of optic nerves DWI in different diffusion directions, verifying the spatial characterization capabilities of our method for optic nerves. Fig.5 compares the reconstruction results and SNR maps of DWI among different techniques, demonstrating that the proposed 3D reduced-FOV multi-shot DWI can better depict the optic nerves.Discussion
Because the optic nerve is a small bundle of nerve fibers, probing any change in its microstructure requires high-resolution and high-fidelity DWI techniques. However, the 2D DWI techniques are limited by the low SNR levels when acquiring the DWI data with 1.6-mm isotropic resolution, making the depiction of optic nerves extremely challenging (Fig.5). In addition, the 2D single-shot DWI also shows severe distortion and image blurring due to the long echo train length. Furthermore, the 2D 2-shot reduced-FOV DWI encountered reconstruction failures due to the extreme aliasing of the tissues, and requires further modification of MUSE reconstruction framework to accommodate the multi-shot DWI data acquired with tight FOV. Therefore, it is challenging for 2D DWI techniques to depict the optic nerves. As for 3D DWI, 3D 2-shot DWI still presents noticeable distortion, particularly at the eyeball region. In contrast, the 3D reduced-FOV 2-shot DWI could further reduce distortion and achieve improved depiction of optic nerves (Figs.4&5), indicating the preliminary feasibility and applicability of high-resolution and high-fidelity optic nerves DWI. This study still has two major limitations. Firstly, signal loss of optic nerves originating from phase dispersion induced by eye motion might exist. Integrating prospective or retrospective motion correction techniques into the proposed technique may possibly improve the robustness. Secondly, more quantitative analysis is needed for evaluating the diagnostic performance of 3D reduced-FOV 2-shot DWI for patients with optic nerve diseases.Conclusion
The study has preliminarily shown the feasibility of 3D reduced-FOV multi-shot DWI in depicting the optic nerves with high resolution and high fidelity, therefore potentially benefiting the clinical applications of optic nerves DWI.Acknowledgements
The work was in part supported by grants from Hong Kong Research Grant Council (GRF17106820, GRF17125321, GRF14206723, and ECS24213522).References
[1] Smith S A, Williams Z R, Ratchford J N, et al. Diffusion tensor imaging of the optic nerve in multiple sclerosis: association with retinal damage and visual disability[J]. American journal of neuroradiology, 2011, 32(9): 1662-1668.
[2] Liu J, Xu X, Yan J, et al. Diffusion‐Weighted MR Imaging of the Optic Nerve Can Improve the Detection of Post‐Laminar Optic Nerve Invasion from Retinoblastoma[J]. Journal of Magnetic Resonance Imaging, 2023, 57(5): 1587-1593.
[3] Bender B, Heine C, Danz S, et al. Diffusion restriction of the optic nerve in patients with acute visual deficit[J]. Journal of Magnetic Resonance Imaging, 2014, 40(2): 334-340.
[4] Chen N, Guidon A, Chang H C, et al. A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE)[J]. Neuroimage, 2013, 72: 41-47.
[5] Saritas E U, Cunningham C H, Lee J H, et al. DWI of the spinal cord with reduced FOV single‐shot EPI[J]. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 2008, 60(2): 468-473.
[6] Xu X, Zhang B, Sun K, et al. Reliability and validity of multi-shot DWI in diagnosis of cervical spondylotic myelopathy: a study based on 3-T MRI[J]. European Spine Journal, 2020, 29: 1219-1226.
[7] Chang H C, Sundman M, Petit L, et al. Human brain diffusion tensor imaging at submillimeter isotropic resolution on a 3 Tesla clinical MRI scanner[J]. Neuroimage, 2015, 118: 667-675.
[8] Skare S, Clayton D, Newbould R, et al. A fast and robust minimum entropy based non-interactive Nyquist ghost correction algorithm[C]//Proceedings of the 14th Annual Meeting of ISMRM. 2006: 460.
Figures